

Abstract
Objective. Although most patients with rheumatoid arthritis (RA) respond to anti–tumor necrosis factor (anti-TNF) treatment, some present with initial nonresponse (1ry nonresponse) or lose initial responsiveness (2ry nonresponse). We compared the rate of real-world “nonresponse” to first anti-TNF as reported by treating physicians to the nonresponse rate per accepted definitions and recommended treat-to-target strategies.
Methods. Patients were included from the Biologic Treatment Registry Across Canada (BioTRAC) and Ontario Best Practices Research Initiative (OBRI) registries who were taking their first anti-TNF, with ≥ 1 followup visit. Posthoc reclassification of physician-reported nonresponse was based on prior achievement of 28-joint count Disease Activity Score based on erythrocyte sedimentation rate (DAS28-ESR) low disease activity (LDA), Clinical Disease Activity Index (CDAI) LDA, or good/moderate European League Against Rheumatism (EULAR) response, and actual time of physician-reported nonresponse.
Results. Among 736 BioTRAC and 640 OBRI patients, 13.7% and 18%, respectively, discontinued their anti-TNF because of physician-reported nonresponse. Based on reclassification using disease activity, 65.6% (BioTRAC) and 87.2% (OBRI) of 1ry nonresponders did not achieve DAS28-ESR LDA, 65.6%/90.7% CDAI LDA, and 46.9%/61.5% good/moderate EULAR response. Among 2ry nonresponders, 50.7%/47.8% did not achieve DAS28-ESR LDA, 37.7%/52.9% CDAI LDA, and 15.9%/19.6% good/moderate EULAR response before treatment discontinuation. Regarding actual time of nonresponse, 18.8% of BioTRAC and 60.8% of OBRI 1ry nonresponders discontinued at ≤ 6 months. In both registries, a high proportion of 2ry nonresponders discontinued their anti-TNF after 12 months (87.0% BioTRAC, 60.9% OBRI).
Conclusion. Physician-reported 1ry nonresponse was more correlated with non-achievement of DAS28-ESR LDA or CDAI LDA, whereas 2ry nonresponse with actual time of discontinuation. Further work is needed to confirm the importance of response and type of response to the initial anti-TNF in identifying patients most likely to benefit from a second biologic agent treatment.
- TUMOR NECROSIS FACTOR INHIBITORS
- BIOLOGICAL THERAPY
- REGISTRIES
- PHYSICIAN PRACTICE PATTERNS
- RHEUMATOID ARTHRITIS
Current rheumatoid arthritis (RA) treatment guidelines advocate the use of biological DMARD (bDMARD) for patients with RA who have failed treatment with methotrexate (MTX) and/or other conventional synthetic DMARD (csDMARD). These patients are labeled as MTX/csDMARD incomplete responders (MTX/csDMARD-IR)1. Nine biologics and 1 small molecule DMARD are currently available for use, which, in a recent Cochrane review, were found to improve prognosis by attenuating radiographic progression and conferring greater rates of treatment response and remission when used in MTX/csDMARD-IR patients1.
Nevertheless, about one-third of patients with RA continue to miss clinical endpoints of response on bDMARD/csDMARD combination therapy2,3. For these patients, successive biologic switching, either within the same, or to different mechanistic class(es), is advocated by all major international treatment guidelines4,5,6. Patients not responding to biologic therapy may be categorized as primary (1ry) or secondary (2ry) nonresponders, the former owing to initial lack of response, and the latter owing to loss of responsiveness over time3.
Although current best practice guidelines advocate the implementation of patient-centric treatment goals and treat-to-target strategies, the criteria for response differ across guidelines4,5,6, potentially fragmenting the application of outcome measures into regionally specific preferences. Consequently, clinical studies use definitions of treatment response that may differ in both the timing and criteria used2,7–16, limiting their comparability. Further, more recent data suggest that primary anti–tumor necrosis factor (anti-TNF) nonresponders differ in their response to a second anti-TNF compared to 2ry nonresponders17,18,19; 1ry nonresponders of the first anti-TNF are less likely to respond to a second anti-TNF while 2ry nonresponders are more likely to respond to a second anti-TNF. These data have implications for the current algorithm of care using anti-TNF therapy, which suggests that prior primary failure of an anti-TNF should lead to use of a biologic with a different mechanism of action.
Characterization of this heterogeneity in response definitions, and the associated implications, remains to be done in routine clinical practice settings. Using data derived from patients with RA enrolled in the Biologic Treatment Registry Across Canada (BioTRAC) registry and the Ontario Best Practices Research Initiative (OBRI) clinical registry, 2 analyses were independently conducted to examine what treating rheumatologists considered 1ry or 2ry nonresponse of anti-TNF therapy in their routine clinical practice. To answer this question, we assessed the rate of “nonresponse” based on the judgment of the treating physicians, among RA patients treated with their first anti-TNF in Canadian routine clinical practice and contrasted them to the rate of nonresponse using standard guideline definitions4,5,6.
MATERIALS AND METHODS
Registry descriptions
In accordance with the observational features of a registry, the management of patients enrolled in both the BioTRAC and OBRI registries, including the frequency of assessments, is based on the medical judgment of the treating physician, and all treatment(s) must be prescribed in accordance with the respective Canadian product monograph(s)6,20,21,22,23. All patients enrolled provided written informed consent, and approvals for participation were obtained from the local Research Ethics Boards of participating academic sites, and central Institutional Review Boards (IRB) for non-academic sites (OBRI REB#: 07-0729 AE; BioTRAC REB: IRB Services, Ontario, Canada). The BioTRAC and OBRI registries are conducted as per the tenets of the Declaration of Helsinki.
BioTRAC registry
BioTRAC is an ongoing, Canada-wide, multicenter, observational, prospective study of patients initiating treatment with infliximab (IFX) or golimumab (GOL) for RA, ankylosing spondylitis (AS), or psoriatic arthritis (PsA); or with ustekinumab for PsA. The goal of the registry is to collect real-world clinical, laboratory, patient-centric, and safety data on PsA, AS, and RA patients treated in routine care24. Patients ≥ 18 years old, who are biologic-naive, or who have been previously treated with 1 biologic agent, are considered for inclusion in the registry. Patients are followed from initiation of IFX, GOL, or ustekinumab to treatment discontinuation. At the time of analysis, BioTRAC had collected data from over 80 rheumatology practices, with over 3000 RA, AS, and PsA patients enrolled. In our study, only the patients with RA were included.
OBRI registry details
OBRI, founded in 2005, is a prospective registry of patients with RA followed long term in routine care in Ontario, Canada25,26. All patients ≥ 18 years of age, diagnosed with RA after the age of 16 years, and presenting with active disease (defined as at least 1 swollen joint) are eligible for inclusion26. Registry goals include reporting on the safety, effectiveness, and sustainability of available RA therapies, identifying clinical practice patterns for the improvement of patient outcomes, as well as using clinical and economic outcome data to inform healthcare policy26. Over 2500 patients were enrolled from over 60 rheumatology practices at the time of analysis25,27.
Selection criteria
Biologic-naive patients with RA initiating their first anti-TNF agent, with available information on 28-joint count Disease Activity Score based on erythrocyte sedimentation rate (DAS28-ESR) at baseline, and at least 1 post-baseline visit, were initially selected from both registries. Those discontinuing treatments because of nonresponse as per the treating physician’s judgment were included in all analyses. Baseline was considered as the date of initiation of the first anti-TNF therapy. For OBRI, a window of < 30 days prior to enrollment in the registry was allowed for anti-TNF initiation, and baseline DAS were assessed within 60 days before and 30 days after anti-TNF initiation.
Treatment response
The BioTRAC and OBRI registries evaluate response to anti-TNF therapy based on the judgment of the treating physician. OBRI registry patients not responding to treatment per the judgment of the treating physician are categorized by the treating physician as 1ry nonresponse (failure to achieve initial response), or as loss of response (failure to maintain response after a recommended period of ≥ 3 months). BioTRAC patients discontinuing anti-TNF treatment for effectiveness reasons are classified by the treating physician as experiencing either a lack of response (1ry non -response) or loss of response (2ry nonresponse).
Posthoc reclassifications of physician-reported nonresponse to the first anti-TNF agent were performed by the authors for both registry analyses. One reclassification was based on whether a patient clinically responded to treatment — that is, whether (1) a DAS of ≤ 3.2 [low disease activity (LDA)]; (2) good/moderate European League Against Rheumatism (EULAR) response; or (3) a Clinical Disease Activity Index (CDAI) score of ≤ 10 (LDA), was achieved28. A second reclassification was based on actual time of physician-reported nonresponse, categorized as ≤ 6, > 6 to ≤ 12 months.
Statistical analysis
Descriptive statistics were produced for all baseline patient, disease, and treatment characteristics, including the mean and SD for continuous variables, and proportions for categorical variables.
The agreement between physician-reported nonresponse and reclassification categories was assessed descriptively with the concordant pairs. Time to discontinuation of the first anti-TNF treatment regimen was also assessed with the Kaplan-Meier estimate of the survival function.
Statistical analyses were carried out using SPSS 24.0 (SPSS Inc.) and SAS 9.2 (SAS Institute).
RESULTS
Patient disposition and baseline characteristics
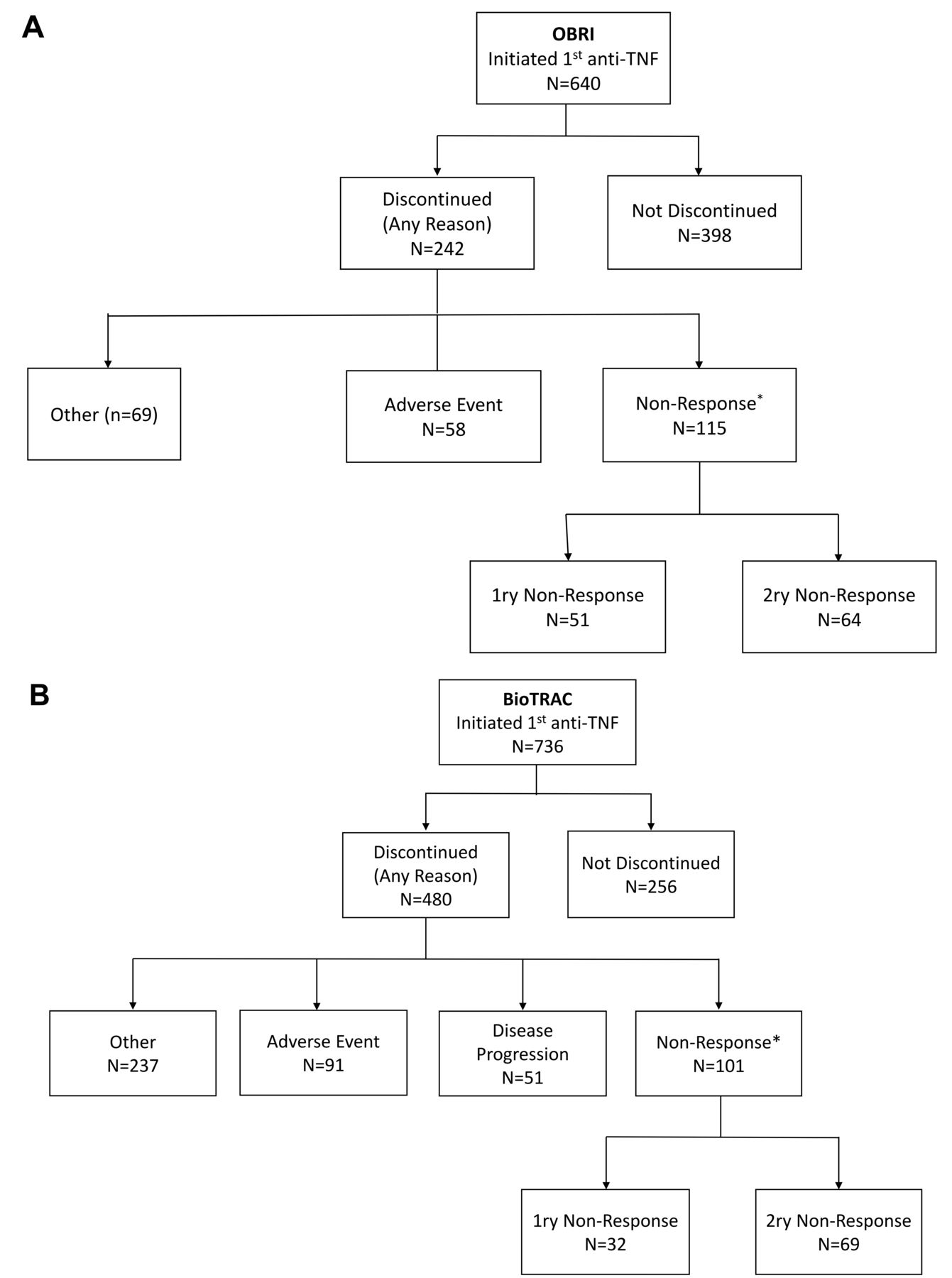
Overall, 736 BioTRAC and 640 OBRI patients met the selection criteria (Figure 1), of which 480 (65.2%) and 242 (37.8%), respectively, discontinued their first anti-TNF treatment due to any reason after 2632 and 1114 person-years of followup, respectively. Median (95% CI) Kaplan-Meier–based time to discontinuation was 3.4 (2.9–4.0) years and 3.6 (3.0–4.8) years in BioTRAC and OBRI, respectively; 1-year and 5-year survival probabilities were 85.5% and 42% in BioTRAC, and 74.2% and 43% in OBRI, respectively. Discontinuation because of physician-reported anti-TNF nonresponse was reported for 101 (13.7%) and 115 (18%) of patients in BioTRAC and OBRI, respectively, which comprised the analysis populations. Within anti-TNF nonresponders as per the physicians’ judgment, the rate of 1ry nonresponse was 31.7% (n = 32) in BioTRAC and 44.3% (n = 51) in OBRI, the remaining 68.3% (n = 69) and 55.7% (n = 64), respectively, judged as 2ry nonresponders.
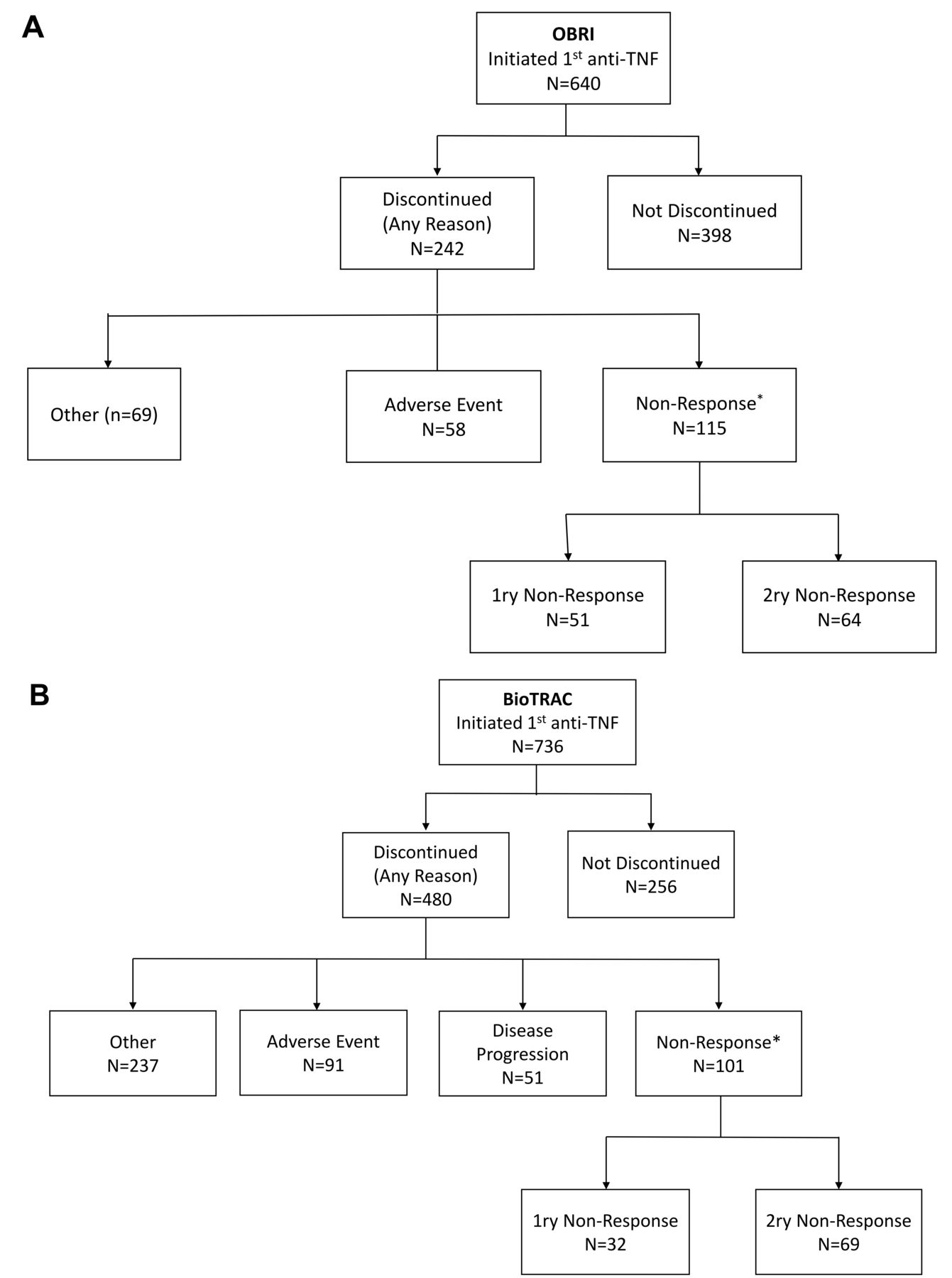
Patient disposition. A. Ontario Best Practices Research Initiative (OBRI). B. Biologic Treatment Registry Across Canada (BioTRAC). Anti-TNF: anti–tumor necrosis factor; 1ry nonresponse: initial nonresponse; 2ry nonresponse: loss of initial responsiveness.
Table 1 provides a summary of the baseline patient and disease characteristics for the 2 analysis populations of RA. In addition, the characteristics of the overall registries of patients with RA are provided for assessment of the comparability of each analysis population with the total population within the respective registry. At anti-TNF initiation, patients in the BioTRAC registry were more likely to be anticitrullinated protein antibody–positive (41.2% vs 34.2%) and had higher disease activity as indicated by the higher DAS28-ESR score (5.6 vs 5.2), swollen (9.5 vs. 7.2) and tender (11.2 vs 8.4) joint counts, and patient’s global assessment (6.3 vs 5.7). Both analysis populations were generally comparable to their respective total cohorts except for disease duration at baseline and followup duration, which were shorter in the analysis populations.
Baseline demographic and disease characteristics of patients with RA, by registry.
Reclassification of physician-reported nonresponse to first anti-TNF based on disease activity
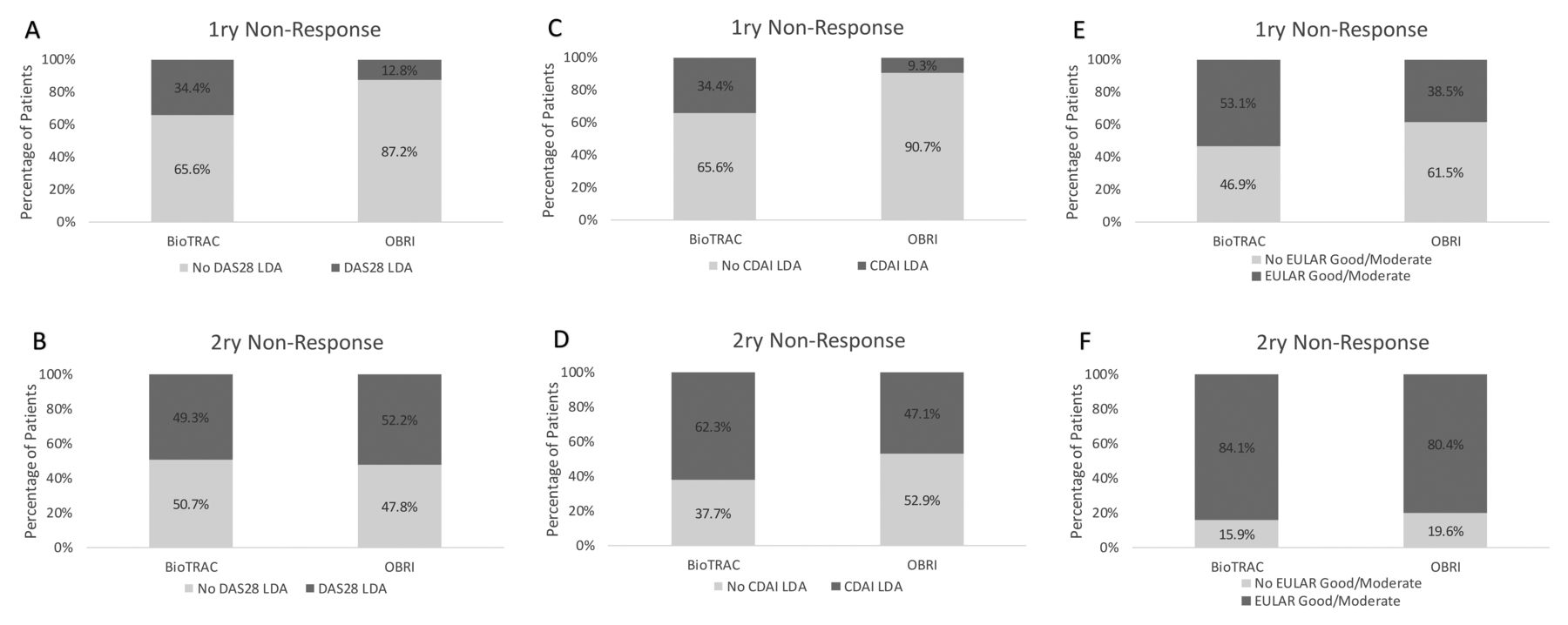
Physician-reported patient’s nonresponse (1ry or 2ry) was contrasted to reclassification based on response criteria, specifically the achievement of DAS28 LDA, CDAI LDA, and good/moderate EULAR response prior to treatment discontinuation. Importantly, 65.6% of BioTRAC and 87.2% of OBRI physician-reported 1ry nonresponders did not achieve DAS28-ESR LDA (Figure 2A); 65.6% and 90.7%, respectively, did not achieve CDAI LDA (Figure 2C); and 46.9% and 61.5%, respectively, did not achieve good/moderate EULAR response (Figure 2E).
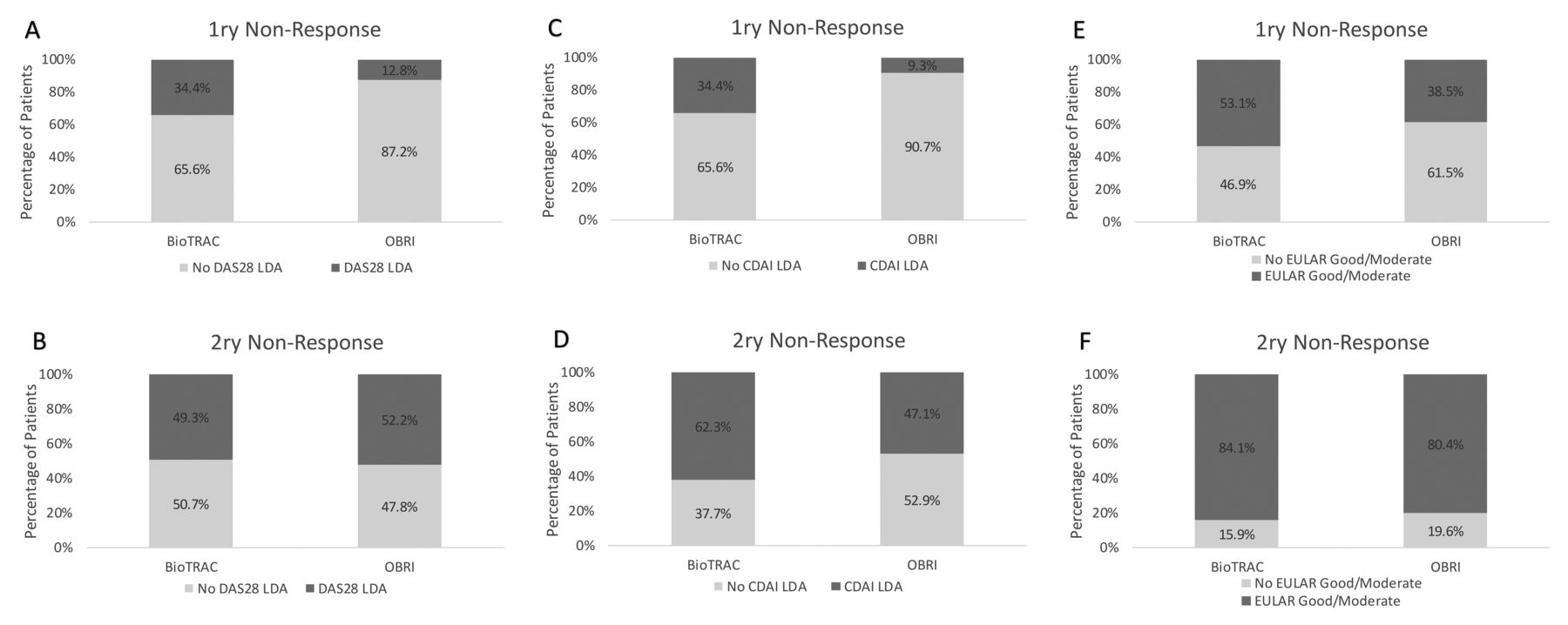
Proportions of patients achieving DAS28-ESR LDA (A, B), CDAI LDA (C, D), and good/moderate EULAR response (E, F) by type of physician-reported nonresponse. 1ry nonresponse: initial nonresponse; 2ry nonresponse: loss of initial responsiveness; DAS28-ESR: 28-joint count Disease Activity Score based on erythrocyte sedimentation rate; LDA: low disease activity; CDAI: Clinical Disease Activity Index; EULAR: European League Against Rheumatism.
Among physician-reported 2ry nonresponders in both registries, almost half of patients did not achieve LDA prior to treatment discontinuation (50.7% BioTRAC and 47.8% in OBRI; Figure 2B); 37.7% and 52.9%, respectively, did not achieve CDAI LDA (Figure 2D); and 15.9% and 19.6%, respectively, did not achieve good/moderate EULAR response (Figure 2F).
Reclassification based on time of physician-reported nonresponse
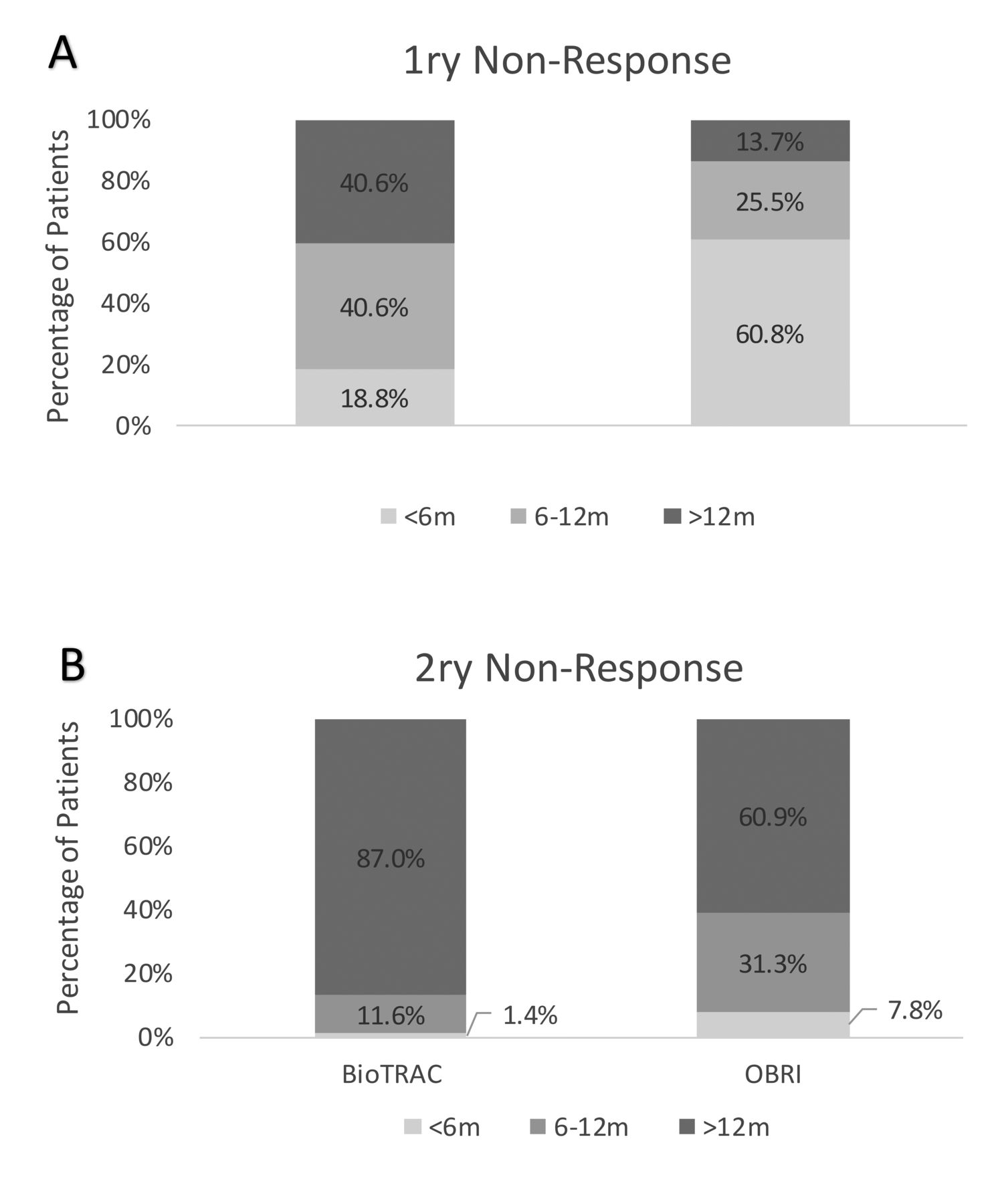
Regarding actual time to physician-reported nonresponse in the BioTRAC cohort, 18.8% of 1ry nonresponders discontinued their first anti-TNF treatment prior to Month 6, 40.6% discontinued between 6 to 12 months, and 40.6% > 12 months post–anti-TNF initiation. In the OBRI cohort, 60.8% of 1ry nonresponders discontinued treatment before 6 months, 25.5% discontinued between 6 to 12 months, and 13.7% after 12 months (Figure 3A).
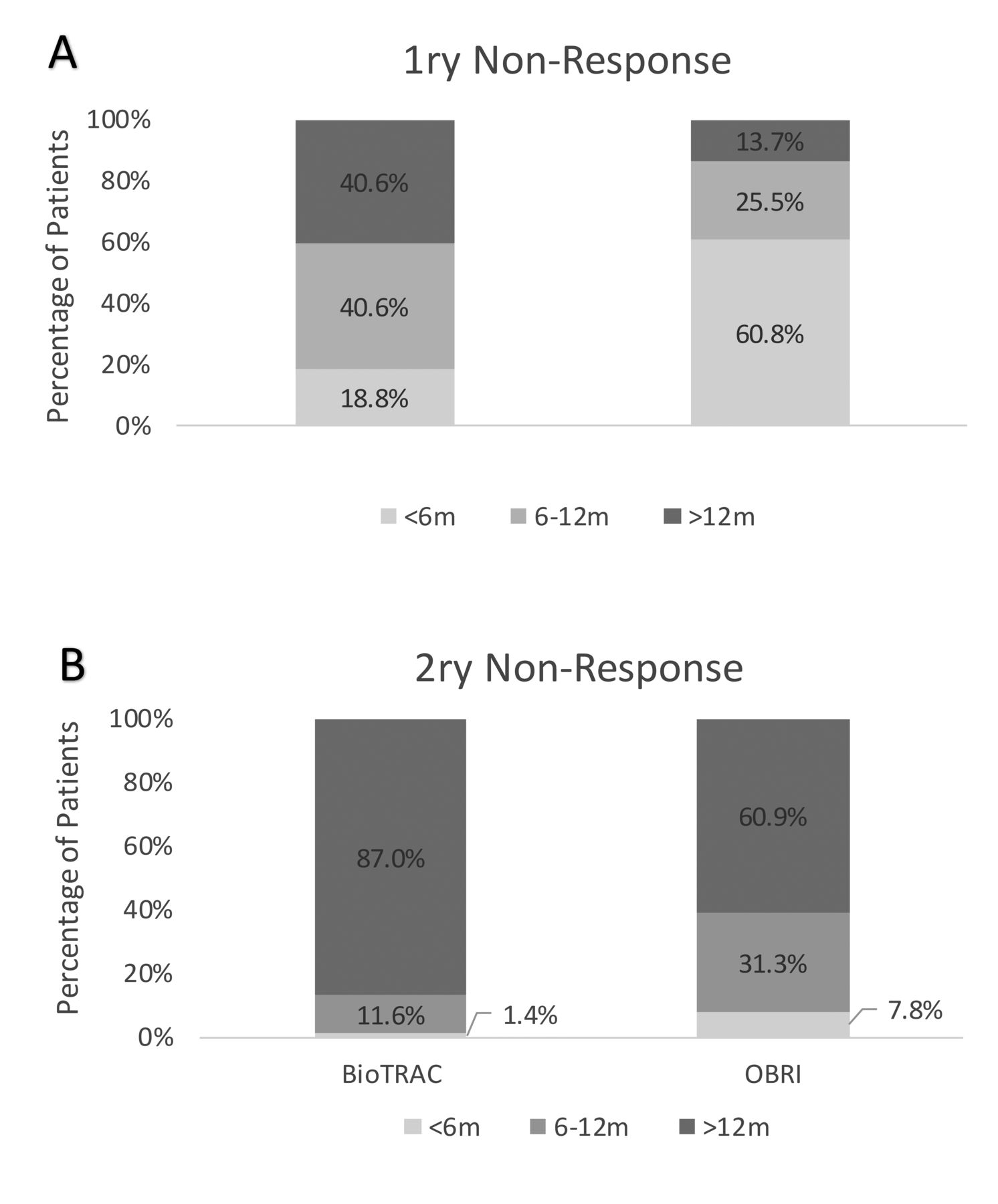
Actual time of physician-reported nonresponse by type of physician-reported nonresponse. 1ry nonresponse: initial nonresponse; 2ry nonresponse: loss of initial responsiveness.
Among patients judged by their treating physician as 2ry nonresponders, in the BioTRAC cohort, 1.4% discontinued treatment before 6 months, 11.6% between 6 to 12 months, and 87.0% after 12 months of anti-TNF initiation. In the OBRI cohort, 7.8% discontinued treatment before 6 months, 31.3% between 6 to 12 months, and 60.9% after 12 months of anti-TNF initiation (Figure 3B).
DISCUSSION
In this joint registry analysis, discontinuation of a first anti-TNF regimen, for any reason, was reported by 65.2% and 37.8% of BioTRAC and OBRI patients, respectively. The difference most likely reflects the longer overall followup of BioTRAC patients as well as differences in clinical practice between Ontario and other provinces (only covered in BioTRAC). Overall, these results are in agreement with a previous metaanalysis29, reporting a rate of anti-TNF discontinuation for any reason at years 2, 3, and 4 of 37%, 44%, and 52%, respectively, as well as with other studies30,31,32,33,34. However, discontinuations specifically for physician-reported nonresponse in both registries were lower compared to the studies by Bartelds, et al (25%)34 and Hyrich, et al (55%)2.
Overall, physician-reported 1ry nonresponse was more correlated to non-achievement of DAS28-ESR LDA and non-achievement of CDAI LDA, rather than good/moderate EULAR response. Physician-reported 2ry nonresponse was more correlated with posthoc reclassification based on actual time of discontinuation, rather than prior achievement of DAS28-ESR LDA, CDAI LDA, or good/moderate EULAR response. These results may reflect the heterogeneity of clinical variables used to gauge response, in addition to patient and physician preferences that may drive retention of treatment, or conversely, cessation of treatment, regardless of treatment outcome35,36.
These results also suggest regional-specific patterns of RA management and could be taken as indication of the lack of consensus among physicians, not only on the definition of treatment nonresponse but also on when a patient should be considered a 1ry nonresponse. Because intensive, treat-to-target management of RA is advocated by Canadian and international treatment guidelines4,5,6,37, the observed delay regarding 1ry nonresponse assessment also suggests that routine care may not completely align with current treatment models. However, both registries included patients from before and after the treat-to-target guidelines era, which could also contribute to the heterogeneity in the definition of 1ry nonresponse.
It is important to emphasize to community physicians which criteria they should consider for definition of 1ry and 2ry nonresponse to the first anti-TNF; it might be possible to extrapolate these criteria to predict response to the second anti-TNF. The findings of our study suggest that the 1ry nonresponse definition should be based on non-achievement of DAS28-ESR LDA or CDAI LDA, whereas actual time of discontinuation should be used for defining 2ry nonresponse.
The main limitation of our study is that the exact reasons for the physicians classifying a patient as a 1ry or a 2ry nonresponder were not available in either registry; these reasons would have led to a more complete picture of clinical practice patterns and decision making. An important strength of our study is the attainment of similar results in both registries, supporting the reliability of the findings.
The results of this joint registry analysis highlight that physician-reported 1ry nonresponse was more correlated to non-achievement of DAS28-ESR LDA or CDAI LDA, whereas physician-reported 2ry nonresponse was more correlated with posthoc reclassification based on actual time of discontinuation. Further work is needed to confirm the importance of 1ry and 2ry nonresponse as well as the type of clinical response to the initial anti-TNF in identifying patients who are most likely to benefit from a second biologic agent treatment.
Acknowledgment
The authors acknowledge the BioTRAC-RA and OBRI-RA investigators. The authors also acknowledge JSS Medical Research for medical writing and editorial services.
Footnotes
This work was partially supported (medical writing services) by Janssen Inc., which manufactures infliximab, golimumab, and ustekinumab. Ontario Best Practices Research Initiative (OBRI) was funded by peer-reviewed grants from the Canadian Institute for Health Research (CIHR), the Ontario Ministry of Health and Long-Term Care (MOHLTC), the Canadian Arthritis Network (CAN), and unrestricted grants from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Hospital Janssen, Pfizer, Roche, Sanofi, and UCB.
ECK has received funding for research from Abbott Laboratories, Amgen Inc., Bristol-Myers Squibb, F. Hoffmann-La Roche Inc., Gilead, Janssen Inc., Lilly Pharmaceuticals, Pfizer Pharmaceuticals, and Sanofi-Aventis; has a consulting agreement/is a member of an advisory board for Abbott Laboratories, AstraZeneca Pharma, Biotest, Bristol-Myers Squibb, Celltrion, Crescendo Bioscience, F. Hoffmann-La Roche Inc., Genentech Inc., Gilead, Janssen Inc., Lilly Pharmaceuticals, Merck, Pfizer Pharmaceuticals, UCB, and Sandoz; and has speaker honoraria agreements with Amgen, Abbott Laboratories, Bristol-Myers Squibb Canada, F. Hoffmann-La Roche Inc., Janssen Inc., Merck, Pfizer Pharmaceuticals, and Sanofi Genzyme UCB. AC, MM, and CB are employees at OBRI, which was funded by peer-reviewed grants from CIHR, MOHLTC, CAN, and unrestricted grants from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Hospital Janssen, Pfizer, Roche, Sanofi, and UCB. ER, MS, and JSS are employees at JSS Medical Research, the contract research organization mandated to manage BioTRAC. FN is an employee at Janssen. KM is a former employee of Janssen.
- Accepted for publication June 20, 2019.








{kind=link}
{kind=link}
{kind=link}