

Abstract
Objective. The optimal treatment strategy for anti-aminoacyl-tRNA synthetase antibody–positive polymyositis/dermatomyositis-associated interstitial lung disease (anti-ARS-PM/DM-ILD) is yet to be established. We aimed to evaluate the efficacy of glucocorticoids and calcineurin inhibitors (CNI) in patients with ARS-PM/DM-ILD.
Methods. Progression-free survival (PFS) and overall survival rates were retrospectively evaluated in 32 consecutive patients with ARS-PM/DM-ILD. Disease progression was defined as deterioration in PM/DM-ILD (including recurrence). Predictive factors associated with PFS were analyzed by Cox hazards analysis. The efficacy of first-line prednisolone (PSL) plus CNI therapy was compared with that of PSL monotherapy using propensity score–matched analysis.
Results. Overall, 20 (62.5%) and 12 (37.5%) patients received first-line therapy with PSL + CNI and PSL, respectively. The 2-year PFS and 5-year survival rates in the overall cohort were 68.8% and 96.9%, respectively. On multivariate analysis, arterial oxygen pressure (HR 0.86) and PSL monotherapy (vs PSL + CNI; HR 7.29) showed an independent association with PFS. Baseline characteristics of propensity score-matched PSL + CNI and PSL groups were similar. The 2-year PFS rate was significantly higher in the matched PSL + CNI group than in the matched PSL group. All patients who experienced disease progression during first-line therapy were subsequently treated with second-line therapies. The 5-year survival rates of both the matched PSL + CNI and PSL groups were favorable.
Conclusion. Propensity score–matched analysis demonstrated that first-line PSL + CNI therapy for patients with ARS-PM/DM-ILD significantly improved the PFS compared with PSL monotherapy, although there was no significant difference regarding longterm survival.
- DERMATOMYOSITIS
- POLYMYOSITIS
- INTERSTITIAL LUNG DISEASE
- ANTI-AMINOACYL TRNA-SYNTHETASE ANTIBODY
- CALCINEURIN INHIBITOR
Polymyositis (PM) and dermatomyositis (DM) are systemic autoimmune disorders that affect skeletal muscle, skin and/or other organs1,2,3. Interstitial lung disease (ILD) is a frequent occurrence in patients with PM/DM; it worsens the associated morbidity and mortality4,5,6,7,8,9. Currently, glucocorticoids (GC) with/without immunosuppressants are the empirical first-line therapy for PM/DM-associated ILD (PM/DM-ILD). Calcineurin is a calcium/calmodulin-activated serine/threonine phosphatase that upregulates the transcription of interleukin 2 and other T lymphocyte cytokines. Calcineurin inhibitors (CNI), including tacrolimus (TAC) and cyclosporine (CSA), are often used for treatment of PM/DM-ILD in Japan10,11. However, the optimal treatment strategy for PM/DM-ILD is yet to be established because of the rarity of the disorders, their variable clinical phenotypes, and the lack of data from randomized controlled clinical trials (RCT).
Myositis-specific autoantibodies (MSA) are mutually exclusive diagnostic serum PM/DM biomarkers, which relate to distinct PM/DM subsets12,13,14. Anti-aminoacyl tRNA-synthetase enzyme (ARS) and anti-melanoma differentiation-associated gene 5 (MDA-5) antibodies are 2 major MSA in patients with PM/DM-ILD13,14. Of note, the therapeutic response and prognoses of anti-ARS antibody–positive and anti-MDA5 antibody–positive patients are quite different14,15,16,17,18,19. Therefore, the distinction between anti-ARS antibody-positive and anti-MDA5 antibody-positive cases is considered essential in clinical practice12,13,14,20. We previously suggested that the therapeutic strategy for PM/DM-ILD should be established according to MSA status14.
Studies have shown that about 30%–50% of patients with PM/DM-ILD have anti-ARS antibodies, including anti-Jo1, PL7, PL12, EJ, OJ, and KS13,21,22. Although each type of anti-ARS antibody is associated with some unique clinicopathological features23,24, these subsets commonly present with similar manifestations, such as ILD, myositis, arthritis, Raynaud phenomenon, and mechanic’s hands. Patients with anti-ARS antibody-positive PM/DM-ILD (ARS-PM/DM-ILD), an MSA subgroup of PM/DM-ILD, often respond well to GC therapy, including prednisolone (PSL), and have a relatively favorable prognosis17,19,21,22. Moreover, the presence of these antibodies was shown to be associated with recurrence of myositis and/or ILD22. The typical clinical course of ARS-PM/DM-ILD is not well characterized. In addition, the specific indications for the addition of immunosuppressants (including CNI) as a first-line therapy for ARS-PM/DM-ILD are still being discussed. To address these issues, we aimed to characterize the clinical course after first-line therapy initiation, including the survival outcomes such as progression-free survival (PFS) and overall survival. The objective of our study was to clarify the factors associated with PFS of patients with ARS-PM/DM-ILD and to compare the efficacy of first-line PSL plus CNI (PSL + CNI) therapy with that of PSL monotherapy using propensity score-matched analysis, a statistical matching technique that helps minimize the influence of confounding variables25.
MATERIALS AND METHODS
Subjects
We retrospectively reviewed 73 consecutive patients with PM/DM-ILD who were treated with systemic immunosuppressive therapy between 2000 and 2018 at the Hamamatsu University Hospital (Hamamatsu, Japan). The flowchart for our study is presented in Supplementary Figure 1, available with the online version of this article. Of the 73 patients, 34 were seropositive for any anti-ARS antibodies, and of these 34, thirty-two who had been followed up for more than 2 years since the initiation of first-line therapy or had died within the 2 years were included in our study.
The diagnosis of PM/DM was based on the Bohan and Peter criteria1,2. In our study, patients with definite or probable PM/DM were included. The diagnosis of clinically amyopathic DM (CADM) was based on the Sontheimer criteria with a slight modification – the presence of a typical rash with little or no clinical evidence of myopathy during the study period3,7,8,9,14,21. The diagnosis of ILD was based on clinical findings and high-resolution computed tomography (HRCT), with or without lung biopsy findings26,27,28. Consequently, PM/DM-ILD was diagnosed by consensus among rheumatologists and pulmonologists. ILD onset was classified as acute (aggravation < 1 month from the onset of respiratory symptoms or the initial visit), sub-acute (aggravation within 1–3 mos), or chronic (slowly progressive > 3 mos), according to the clinical presentation.
This single-center study was conducted according to the Declaration of Helsinki and involved a retrospective review of clinical records. The institutional review board of Hamamatsu University School of Medicine approved this study (approval no. 18-084). The requirement for written informed consent of the patient was waived owing to the retrospective nature of the study.
Detection of anti-ARS antibodies
Baseline serum samples collected at the time of diagnosis were available for all the patients with PM/DM−ILD. The samples were stored at −20°C or −80°C until further processing. The presence of anti-ARS antibodies (e.g., anti-PL-7, anti-Jo1, anti-PL-12, anti-KS, anti-EJ, and anti-OJ) was retrospectively measured using RNA and protein immunoprecipitation assays, a gold standard method to detect MSA, including anti-ARS antibodies15,23,29.
Endpoints and assessment protocol
The primary endpoint to evaluate the efficacy of first-line therapy was PFS rate. PFS was defined as the time from the date of initiation of first-line therapy until the date of first disease progression of PM/DM-ILD, death, or the most recent visit. The secondary endpoints were overall survival rate and safety of treatment. Overall survival was defined as the time from the date of initiation of first-line therapy until the date of death or the most recent visit.
The efficacy of first-line therapies was retrospectively assessed according to the assessment protocol for PM/DM-ILD. As a result of the reassessment, we confirmed that all patients had been evaluated according to this protocol. In this cohort, all patients were followed up at least every month for more than 2 years or until death. Disease progression was defined as deterioration of PM/DM-ILD. Recurrence was defined as when a patient who had fulfilled the criteria for improvement with first-line therapy fulfilled the criteria of deterioration later. Improvement, deterioration, and stable/unchanged status of PM/DM-ILD were defined on the basis of the International Consensus Statement of idiopathic pulmonary fibrosis with modification for PM/DM-ILD28. Briefly, improvement of PM/DM-ILD was defined by 2 or more of the following: (1) improvement in dyspnea and PM/DM-related extrapulmonary symptoms including muscle weakness/myalgia and rash; (2) decrease in ILD-related parenchymal abnormality on chest HRCT or radiograph, and/or (3) ≥ 10% increase in percent predicted forced vital capacity (%FVC), ≥ 15% increase in percent predicted DLCO, ≥ 10 Torr increase in arterial oxygen pressure (PaO2), or ≥ 4% increase in peripheral capillary oxygen saturation (SpO2). Deterioration of PM/DM-ILD was defined by 2 or more of the following: (1) deterioration in dyspnea or PM/DM-related extrapulmonary symptoms; (2) increase in ILD-related parenchymal abnormality on chest HRCT or radiograph; (3) ≥ 10% decrease in %FVC, ≥ 15% decrease in %DLCO, ≥ 10 Torr decrease in PaO2, or a ≥ 4% decrease in SpO2; and/or (4) new development of PM/DM-related extrapulmonary manifestations. Stable/unchanged of PM/DM-ILD was defined when a patient did not meet the criteria for improvement or deterioration of PM/DM-ILD. Disagreements, if any, were resolved by consensus among pulmonologists and rheumatologists.
Adverse events during first-line therapy were retrospectively evaluated on the basis of Common Terminology Criteria for Adverse Events (CTCAE) v5.0 (ctep.cancer.gov/protocolDevelopment/adverse_effects.htm). In our study, only grades of ≥ 3 were recorded.
First-line therapies
All patients were treated with initial doses of PSL (0.5–1.0 mg/kg body weight per day). PSL was tapered by 10–20% dose every 2–4 weeks until progression of PM/DM-ILD or attainment of a maintenance PSL dose of 0.1–0.2 mg/kg body weight per day. CNI such as CSA and TAC were selected at the discretion of the attending physician. CSA was initiated orally at a dose of 2–3 mg/kg body weight per day, followed by adjustment to trough levels of 100–150 ng/ml and levels of 600–800 ng/ml at 2 h after administration. TAC was initiated orally at a dose of 0.06–0.1 mg/kg bodyweight per day and followed by adjustment to trough levels of 5–10 ng/ml.
Statistical analysis
All values are expressed as median (range) or frequency (%). Fisher’s exact test was used for comparison of proportions among groups, whereas the Mann–Whitney U test was used for comparison of medians. The overall survival and PFS were evaluated using the Kaplan–Meier method and the between-group differences assessed using the log-rank test. Patients were censored if they remained alive until April 31, 2018. Cox hazards analysis was used to identify variables associated with PFS; all variables identified as significant in the univariate analysis were included in the multivariate analysis. A propensity score (the predicted probability of a patient being assigned to PSL monotherapy or PSL + CNI therapy) was estimated by a logistic regression model that was adjusted for patient characteristics. Propensity score matching was performed using the following algorithm: 1:1 optimal match with a ± 0.03 caliper and no replacement. In all analyses, p < 0.05 was considered statistically significant. All data were analyzed using commercially available software (JMP version 13.2.1, SAS Institute Inc.) and R software version 2.15.1 (The R Foundation for Statistical Computing, Austria).
RESULTS
Baseline characteristics and clinical course of all patients with ARS-PM/DM-ILD
Baseline characteristics of all 32 patients with ARS-PM/DM-ILD are summarized in Table 1. Regarding first-line therapy, 12 patients (37.5%) were treated with PSL alone (PSL group) and 20 (62.5%) were treated with PSL + CNI [CSA (n = 16), TAC (n = 4), PSL + CNI group). The median initial PSL dose was 0.75 mg/kg body weight once daily. None of the patients discontinued the first-line therapy because of treatment-related adverse events.
Characteristics of all patients with ARS-PM/DM-ILD.
Of the 32 patients, 15 (46.9%) showed disease progression, including recurrence, at least once during the study period. The first disease progression in the 15 patients consisted of deterioration within 30 days of initiation of first-line therapy (n = 4), ILD recurrence (n = 9), and myositis recurrence (n = 2). In all these patients, the first-line therapy was changed to second-line therapy with PSL + IS. The second-line therapies included addition of an immunosuppressant [CSA (n = 6), TAC (n = 2), cyclophosphamide (CYC; n = 1)] in the PSL group or change to another immunosuppressant [TAC (n = 4), CYC (n = 1), azathioprine (AZA; n = 1)] in the PSL + CNI group.
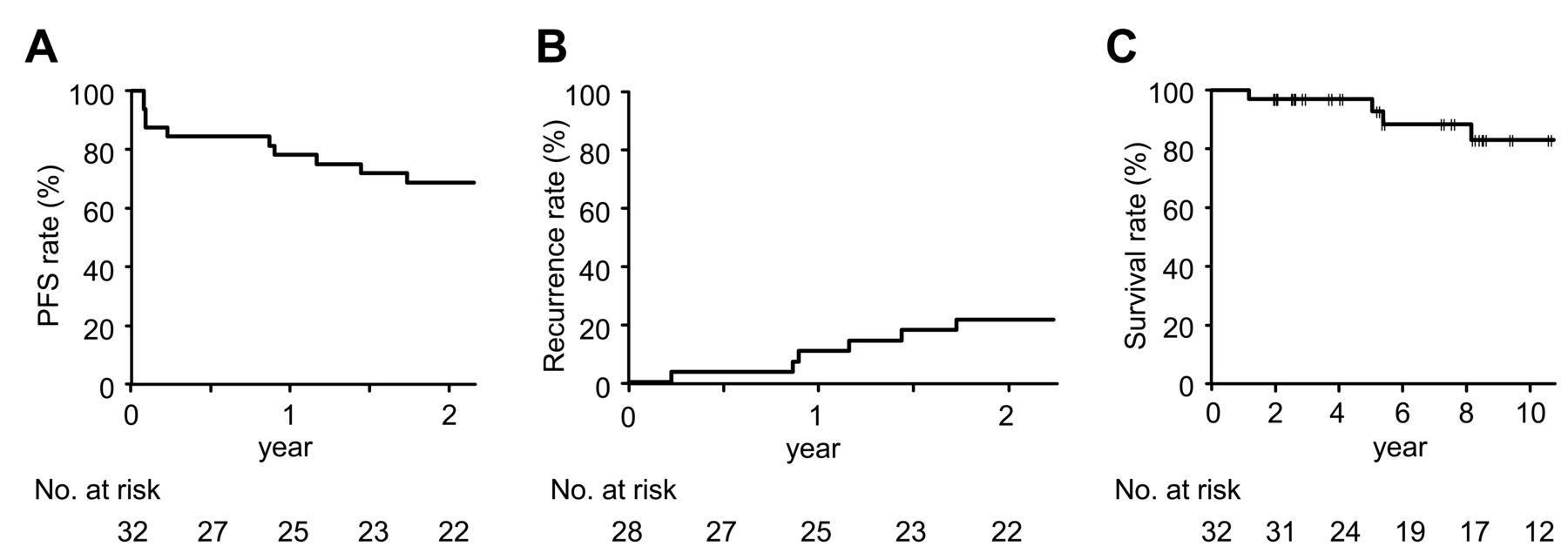
The 2-year PFS rate was 68.8% (95% CI 49.7–81.8%; Figure 1A). In the remaining 28 patients (except for 4 who showed deterioration within 30 days of initiation of first-line therapy), the 2-year recurrence rate was 21.4% (95% CI 10.2–41.6%; Figure 1B).

Kaplan–Meier survival curves for all patients with ARS-PM/DM-ILD. A. The 1- and 2-year PFS rates were 78.1% and 68.8%, respectively. B. In the remaining 28 patients, except for 4 who showed deterioration within 30 days of first-line therapy initiation, the 1- and 2-year recurrence rates were 10.7% and 21.4%, respectively. C. The 5- and 10-year survival rates were 96.9% and 83.1%. ARS-PM/DM-ILD: aminoacyl-tRNA synthetase antibody–positive polymyositis/dermatomyositis-associated interstitial lung disease; PFS: progression-free survival.
Overall, 5 (15.6%) of the 32 patients with ARS-PM/DM-ILD died during the study period. Two deaths were due to ARS-PM/DM-ILD. The other 3 deaths were attributed to a cancer of unknown primary origin that developed after PM/DM-ILD diagnosis (n = 1), heart failure (n = 1), or pneumonia (n = 1). The cumulative 5-year survival rate was 96.9% (95% CI 79.8–99.6%; Figure 1C).
Predictive factors for PFS
The predictive factors associated with PFS were analyzed using Cox hazards model (Table 2). In univariate analysis, PaO2 (HR 0.92, p = 0.01) and first-line therapy with PSL (vs PSL + CNI; HR 2.88, p = 0.04) were associated with PFS. On multivariate analysis, lower PaO2 levels (HR 0.86, p < 0.001) and first-line therapy with PSL (vs PSL + CNI; HR 7.29, p = 0.001) were found to be independent predictors of poor PFS. Although acute/subacute onset of ILD tended to be associated with poor PFS, the association was not statistically significant (vs chronic onset; HR 2.75, p = 0.05).
Results of Cox proportional hazards regression analysis for first disease progression or death.
Efficacy of first-line PSL monotherapy and PSL + CNI therapy
To analyze the efficacy of first-line therapies with PSL and PSL + CNI for ARS-PM/DM-ILD, we compared the patients who received PSL monotherapy (unmatched PSL group) with those who received PSL + CNI therapy (unmatched PSL + CNI group). No significant differences were observed between the unmatched PSL and PSL + CNI groups with respect to baseline characteristics and initial PSL dose (Supplementary Table 1, available with the online version of this article). However, the 2-year PFS rate in the unmatched PSL + CNI group was significantly higher than that in the unmatched PSL group (85% vs 41.2%, respectively; p = 0.02, Supplementary Figure 2A). However, the cumulative 5-year survival rates were comparable in the 2 groups (91.7% and 100%, respectively; p = 0.92, Supplementary Figure 2B).
To reduce the effect of treatment-selection bias and potential confounding, we performed adjustment for the baseline characteristics between PSL and PSL + CNI groups using the propensity score–matching method. The propensity scores were calculated using a logistic regression model that was adjusted for sex, age, and severity-related variables including ILD onset, %FVC, and PaO2. The distribution of logit conversion scores is presented in Supplementary Figure 3, available with the online version of this article. On the basis of the propensity scores, 12 propensity score-matched pairs were made that included 12 patients treated with PSL monotherapy (matched PSL group) and 12 with PSL + CNI therapy (matched PSL + CNI group).
Baseline characteristics of the matched PSL and PSL + CNI groups are summarized in Table 3. There were no significant differences between the 2 groups regarding the characteristics and the initial PSL dose. The doses of PSL administered from the initiation of first-line therapy until 24 months are presented in Supplementary Figure 4, available with the online version of this article. No significant difference in PSL doses was observed between the matched PSL and PSL + CNI groups in any of the months during the 24-month period.
Characteristics of propensity score–matched patients.
The 2-year PFS rate in the matched PSL + CNI group was significantly higher than that in the matched PSL group (91.7% and 41.7%, respectively; p = 0.03, Figure 2A). The efficacy and adverse events of PSL and PSL + CNI therapies in the propensity score-matched patients are presented in Table 4. Recurrence rate during the first 2 years after initiation of first-line therapy in the matched PSL + CNI group was significantly lower than that in the matched PSL group (8.3% and 33.3%, respectively; p = 0.04). However, no significant between-group difference was observed regarding the incidence of adverse events (≥ CTCAE vs 5.0 grade 3; = 0.67).

Kaplan–Meier survival curves for the matched PSL and PSL + CNI groups. A. The 2-year PFS rate was 91.7% in the matched PSL + CNI group and 41.7% in the matched PSL group (p = 0.03). B. The cumulative 5-year survival rate was 100% in the matched PSL + CNI group and 91.7% in the matched PSL group (p = 0.75). PSL: prednisolone; CNI: calcineurin inhibitor; PFS: progression-free survival.
Efficacy and adverse events of PSL and PSL + CNI therapies in propensity score–matched patients.
Despite significantly different PFS rates in the 2 groups, no significant between-group difference was observed regarding the cumulative survival rate (Figure 2B). Both groups showed favorable longterm survival.
DISCUSSION
In our study, patients with ARS-PM/DM-ILD had received first-line therapy either with PSL or PSL + CNI. The 2-year PFS and 5-year survival rate in the entire study cohort after the initiation of first-line therapy was 68.8% and 96.9%, respectively. On multivariate analysis, lower baseline PaO2 levels and first-line therapy with PSL (vs PSL + CNI) were independent predictors of poor PFS. Propensity score-matched analysis demonstrated that first-line therapy with PSL + CNI significantly improved the PFS and recurrence rates, compared with PSL monotherapy. However, the difference in first-line therapy did not eventually affect longterm survival. To our knowledge, this is the first study to have compared the efficacy of PSL and PSL + CNI therapies for patients with ARS-PM/DM-ILD using propensity score-matched analysis25.
Despite the lack of RCT on PM/DM-ILD, GC with/without immunosuppressants are the mainstay therapy. The choice of immunosuppressants typically depends on the individual preference or experience of the treating physician. Current evidence on the efficacy of immunosuppressants (including CSA, TAC, AZA, and mycophenolate mofetil) for PM/DM-ILD is largely based on retrospective case series, expert opinion, or from noncomparative studies10,30,31,32,33,34. Several retrospective case–control studies suggested the clinical utility of CNI, including CSA and TAC, for PM/DM-ILD. Takada, et al reported in 2005 that patients with DM-ILD who were initially treated with the combination therapy of GC and CSA showed significantly higher survival rates than those patients treated with GC alone10. Kurita, et al reported in 2015 that addition of TAC improved the prognosis of patients with PM/DM-ILD when compared with patients treated with conventional therapy11. On the basis of these reports, we have mainly used CSA as the first-line therapy for PM/DM-ILD over the study period; however, we have also started to use TAC in recent years. However, these studies did not take into account the MSA status. A strength of our study is that the propensity score–matched analysis demonstrated the efficacy of first-line therapy with PSL + CNI for patients with ARS-PM/DM-ILD, as confirmed by the gold standard method to detect MSA (immunoprecipitation assay).
The first major finding in our study is that the first-line therapy with PSL + CNI was associated with significantly higher PFS, compared with PSL monotherapy. Moreover, there was no significant difference in the incidence of adverse events between the 2 therapies. These findings suggest that this combination therapy may help achieve longterm control of ARS-PM/DM-ILD without a concomitant increase in adverse events. Importantly, multivariate Cox hazards analysis revealed that lower PaO2 levels and first-line PSL monotherapy were independent predictors of poor PFS. Therefore, first-line PSL monotherapy may have to be avoided in patients with severe ILD.
The second major finding is that, despite significantly better PFS rates in the PSL + CNI group (vs the PSL group), there was no significant between-group difference regarding the survival rates. All patients who developed disease progression during first-line therapy were subsequently treated with second-line therapy. Although the efficacy of second-line therapy for ARS-PM/DM-ILD was not evaluated in the current study, it is likely that second-line therapy may have helped achieve parity in overall survival rates. A similar phenomenon pertaining to treatment outcomes is often observed in the field of oncology, especially in the context of lung cancer35. Our present study suggests that the attending physician can select the first-line therapy either with PSL + CNI or PSL for patients with ARS-PM/DM-ILD, depending on their severity and potential contraindications to CNI. A further study may be needed to elucidate the efficacy of second-line therapy for ARS-PM/DM-ILD.
In previous studies (including ours), patients with ARS-PM/DM-ILD exhibited better prognoses but more frequently relapsed when compared with other MSA subgroups19,21,22. Consistent with these studies, patients with ARS-PM/DM-ILD in our present study eventually showed more favorable longterm prognoses, regardless of the difference in first-line therapy. In our present study, the 2-year recurrence rate in patients with ARS-PM/DM-ILD was about 20%. Recurrence of disease is clinically important because it tends to impair the quality of life (QOL), increases treatment-related costs, and affects survival. In our study, we could not assess QOL score owing to the retrospective design. Because most of the patients with ARS-PM/DM-ILD achieved longterm survival, evaluation of QOL score should be incorporated as an endpoint in future prospective studies on ARS-PM/DM-ILD.
It is suggested that the clinical features and prognosis may differ depending on the specific types of anti-ARS antibodies23,24. Although we analyzed the association of each type of anti-ARS antibody with PFS, no statistical significance was observed (data not shown), possibly because of the relatively smaller sample size. A larger study should be performed to resolve this issue.
This study had several limitations. First, given the retrospective study design and inclusion of patients with ILD who visited a pulmonary division, our results are subject to several potential biases. For instance, we could not evaluate clinical improvement or deterioration on the basis of the myositis response criteria36. Additionally, although propensity score–matched analysis was used to minimize bias and confounding, more patients with CADM and those with lower forced expiratory volume in 1 s/FVC tended to be included in the matched PSL group compared with the matched PSL + CNI group. It is possible that these tendencies and other unknown confounding factors have affected the result. Second, adverse events during first-line therapy were retrospectively evaluated from the clinical records. It is possible that minor adverse events may have been underestimated. Third, GC therapy is adjustable according to each patient’s condition. Further, in our study population, the CNI used included CSA and TAC. The difference in the speed of tapering GC or difference between these CNI may have affected the results. Finally, we could not analyze prognostic factors associated with survival because only 5 patients with ARS-PM/DM-ILD died during the study period.
We found that the PFS rate of patients with ARS-PM/DM-ILD who were treated with first-line PSL + CNI therapy was significantly higher than that of patients who were treated with PSL monotherapy. However, the first-line therapies did not significantly affect long-term survival. Although some of the patients with ARS-PM/DM-ILD showed disease progression, including recurrence, during first-line therapy, they eventually had favorable longterm prognoses. Possibly, second-line therapy may have helped improve the overall survival. A prospective RCT is required to validate these results. We believe that our results may inform the design of future studies to establish optimal therapeutic strategies for patients with ARS-PM/DM-ILD.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors thank S. Ibuki and S. Mori from the Department of Rheumatology and Clinical Immunology, Graduate School of Medicine, Kyoto University, Kyoto, Japan, for technical support with immunoprecipitation measurements.
- Accepted for publication October 10, 2018.








{kind=link}
{kind=link}