

Abstract
Objective. To determine the incidence of arterial thrombotic events (ATE) and venous thromboembolism (VTE) in antineutrophil cytoplasmic antibody–associated vasculitis (AAV).
Methods. This is a retrospective cohort study presenting the incidence of ATE (coronary events or ischemic stroke) and VTE [pulmonary embolism (PE) or deep venous thrombosis (DVT)] in patients diagnosed with AAV between 2005 and 2014.
Results. There were 204 patients with AAV who were identified. Median followup for surviving patients was 5.8 (range 1–10) years, accounting for 1088 person-years (PY). The incidence of ATE was 2.67/100 PY (1.56 for coronary events and 1.10 for ischemic stroke) and for VTE was 1.47/100 PY (0.83 for DVT only and 0.64 for PE with/without DVT). On multivariate analysis, prior ischemic heart disease (IHD) and advancing age were the only independent predictors of ATE. Among patients without prior IHD or stroke, the incidence of ATE remained elevated at 2.32/100 PY (1.26 for coronary events and 1.06 for ischemic stroke). ATE, but not VTE, was an independent predictor of all-cause mortality. Event rates for both ATE and VTE were highest in the first year after diagnosis of AAV but remained above the population incidence during the 10-year followup period. In comparison to reported rates for the UK population, the event rates in our AAV patients were 15-times higher for coronary events, 11-times higher for incident stroke, and 20-times higher for VTE.
Conclusion. Patients with AAV have a high incidence of arterial and venous thrombosis, particularly in the first year after diagnosis.
- ANTINEUTROPHIL CYTOPLASMIC ANTIBODY-ASSOCIATED VASCULITIS
- THROMBOSIS
- CARDIOVASCULAR DISEASE
- MYOCARDIAL INFARCTION
- STROKE
- VENOUS THROMBOEMBOLISM
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a group of small-vessel vasculitides comprising 3 syndromes: granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic GPA (EGPA)1. In addition, there are patients with renal limited vasculitis (RLV), and “double-positive” disease in patients with both ANCA and anti-glomerular basement membrane (anti-GBM) antibodies2.
AAV is not widely regarded as a disease that carries a high risk of arterial thrombotic events (ATE) or venous thromboembolism (VTE), unlike other inflammatory disorders such as systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA), or renal disorders such as nephrotic syndrome. The incidence of ischemic heart disease (IHD) and VTE in AAV has more recently been described3–11. Antiplasminogen antibody has been reported together with proteinase 3-ANCA and myeloperoxidase (MPO)-ANCA, and associated with disease activity in AAV12,13. It may be pathogenic in AAV and contribute to arterial and venous thrombosis, although this is not yet established.
We conducted a single-center retrospective observational study to determine the incidence rate (IR) of both ATE and VTE, and risk factors for ATE and VTE, in a UK population of patients with AAV. To our knowledge, we are the first group to look at both ATE and VTE in a contemporary cohort.
MATERIALS AND METHODS
We identified patients with the diagnosis of AAV, as defined by the Chapel Hill Consensus Conference1, diagnosed between 2005 and 2014 with at least 1 year of followup at our center in West London. We also included patients who died within 1 year of followup. All patients were treated according to a standard protocol14,15.
Case notes, clinical letters, electronic records, laboratory results, and medical imaging were used to obtain data. We obtained patients’ demographics at presentation (age, sex, ethnicity, and pathology results), evolution of the illness [diagnosis (GPA, MPA, EGPA, RLV, double-positive disease, or overlap syndrome), organ involvement, and the number of relapses], traditional risk factors for ATE (prior IHD or stroke, hypertension at presentation, history of smoking, diabetes mellitus, atrial fibrillation/flutter, and requirement for dialysis), risk factors for VTE (whether they were admitted to hospital at the time of presentation, history of smoking, cancer, and prior VTE) and treatment with blood thinners (warfarin, antiplatelet agents, or heparins) in the first year after diagnosis or at the time of thrombotic event. Because this was a retrospective analysis, ethical approval was not required, in accordance with the policy of our institution.
ATE was defined as acute coronary events [myocardial infarction (MI) or need for coronary artery intervention] and ischemic stroke (confirmed on cerebral imaging). Hemorrhagic strokes were excluded because we were specifically interested in thrombotic events. We separately recorded episodes of peripheral vascular disease requiring amputation. We excluded angina and transient ischemic attacks (TIA), because these diagnoses are difficult to confirm objectively in a retrospective analysis. VTE was defined as pulmonary embolus (PE) and/or deep vein thrombosis (DVT), with supportive imaging studies. Disease relapse was defined as clinical diagnosis of relapse leading to an increase in immunosuppression. We recorded events of ATE, VTE, AAV relapse, pulmonary hemorrhage, and death. We then calculated the IR for ATE and VTE in our population of patients with AAV.
Statistics
The IR was calculated per 100 person-years (PY). All statistical analyses were performed using SPSS (IBM, version 22). All data were regarded as nonparametric owing to the relatively small sample sizes. Continuous variables are presented as median (interquartile range; IQR). Continuous data were compared using the Mann-Whitney U test for comparison between 2 groups. Categorical data were analyzed using the chi-square test. Logistic regression was used to perform multivariate analysis to ascertain risk factors for ATE and VTE following AAV diagnosis. Log-rank test was used to ascertain unadjusted survival differences between patients with and without ATE/VTE events and plotted as Kaplan–Meier curves. Cox proportional regression analysis was used to ascertain risk factors associated with mortality. Data were presented as OR (95% CI) and p value. A p value < 0.05 was considered statistically significant.
RESULTS
There were 204 patients identified. Median followup for surviving patients was 5.8 (range 1–10) years with a total of 1088 PY. The baseline characteristics of our patient group are presented in Table 1 and Table 2. The median age was 55 (41–67) years, and 46% of patients were male. There were 71% of patients who had renal involvement (defined as abnormal urinary sediment with or without elevated creatinine, confirmed on biopsy in 84% of cases), and the median creatinine at presentation was 117 (IQR 73–268) µmol/l. All patients had a diagnosis of AAV. The majority of patients had GPA (54%), 19% had MPA, 7% had EGPA, 13% had RLV, 4% had double-positive (anti-GBM and ANCA) disease, and 3% had an overlap syndrome with features of both AAV and another autoimmune disease such as SLE or mixed connective tissue disease. Twenty-five patients died during the followup period.
Baseline and disease characteristics for entire cohort and groups with ATE and no ATE.
Baseline and disease characteristics for entire cohort, and groups with VTE and no VTE.
Arterial thrombosis
There were 29 ATE following AAV diagnosis in 24 (11.8%) patients. This included 15 nonfatal and 2 fatal acute coronary events, and 12 nonfatal ischemic strokes, resulting in an IR of 2.67 per 100 PY (1.56 for coronary events and 1.10 for ischemic stroke; Table 3). The incidence of ATE was highest early in the disease course with 9 events (31%) occurring in the first year, giving an incidence of 4.9 per 100 PY. The IR from years 2 to 10 was 2.22 per 100 PY. There were 2 events of peripheral vascular disease requiring amputation in the same patient. Because of the very low frequency of amputation, we did not calculate an IR for it.
Incidence of arterial thrombotic event (ATE) and venous thromboembolism (VTE) per 100 person-years in our study and other reported studies.
Baseline characteristics of patients with ATE and without ATE were compared (Table 1). On univariate analysis, older age (p = 0.001), VTE events (p = 0.004), renal involvement (p = 0.020), MPO-ANCA type (p = 0.011), lower albumin level (p = 0.004), higher C-reactive protein (CRP) level (p = 0.001), and prior IHD (p < 0.001) at the time of AAV diagnosis were associated with subsequent ATE. AAV diagnosis subgroup, age, prior IHD, and requirement for renal replacement therapy (RRT) at presentation were factors entered into the multivariate analysis for subsequent ATE. Predictors of ATE were prior IHD (10.9, 95% CI 2.3–52.0; p = 0.003) and age (1.044, 95% CI 1.022–1.077; p = 0.007). There was no significant difference in frequency of relapses of AAV (p = 0.197) or use of blood thinners (p = 0.703) between patients with and without ATE.
Sensitivity analysis
Because prior IHD was a strong predictor of ATE, we reanalyzed the data, excluding patients with prior IHD or stroke, and found that the IR of ATE was still elevated at 2.32 per 100 PY (1.26 for coronary events and 1.06 for ischemic stroke).
Venous thrombosis
There were 16 VTE events in 14 (6.9%) patients, with an IR of 1.47 per 100 PY. Of the 16 events, 9 were DVT only, 3 were PE only, and 4 events were simultaneous DVT and PE. The incidence of VTE was highest early in the disease course, with 5 (31%) events within 1 month of the diagnosis of AAV. Almost half, 7 (44%) events, occurred in the first year after diagnosis (IR 3.8 per 100 PY). In years 2–10 after diagnosis, the IR was 1.00 event per 100 PY.
There was no statistically significant difference in baseline characteristics between patients with and without VTE on univariate analysis (Table 2). Eleven (69%) VTE events occurred during active disease (within 3 mos of a flare of disease). Ten (63%) VTE events occurred following a recent hospital admission. Hospitalization may be considered a surrogate marker of disease severity and activity, but not all admissions were related directly to AAV, and hospitalization is a known independent risk factor for VTE16. Further, 2 (13%) events were thought to be line-related thromboses and 1 patient had a newly diagnosed malignancy at the time of the event. There was no difference in relapse rate (p = 0.918) or use of blood thinners (p = 0.985) between patients with and without VTE.
Mortality
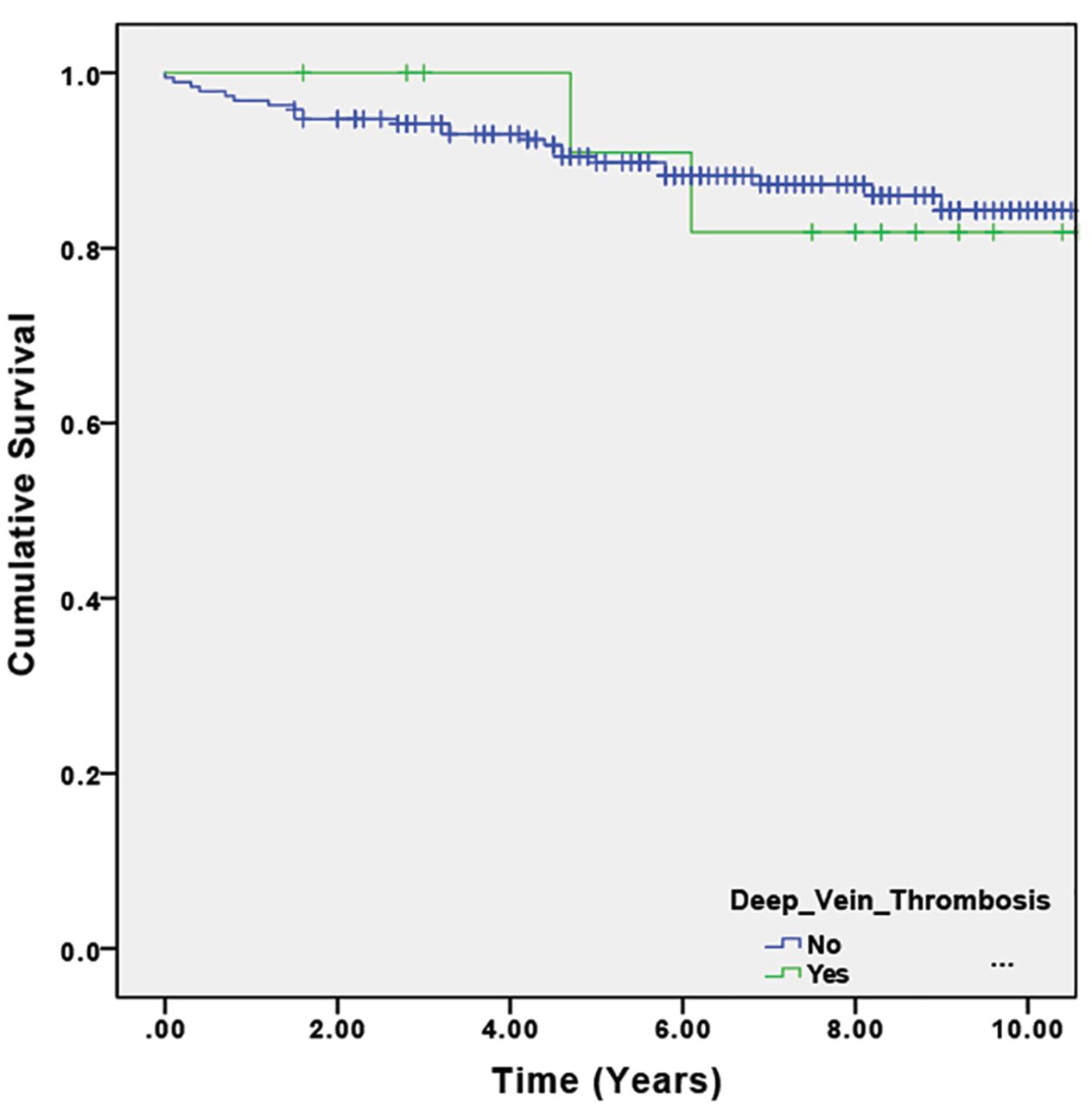
Patients with ATE following AAV diagnosis had a higher mortality rate compared to patients without ATE (p = 0.007; Figure 1). Unadjusted risk factors for mortality on univariate analysis included ATE following diagnosis of AAV (p = 0.007), atrial fibrillation/flutter (p = 0.006), prior IHD (p = 0.026), prior stroke (p = 0.001), AAV subgroup diagnosis (with GPA having a significantly better survival compared to other diagnoses; p = 0.01), advancing age (p < 0.001), and requirement for RRT at presentation (p = 0.007). Age, ATE following diagnosis of AAV, and requirement for RRT at presentation were factors entered into the Cox proportional hazards model for mortality. The only predictor of mortality on multivariate analysis was age [1.076, (1.041–1.112); p < 0.001; Figure 2]. There was no difference in mortality (p = 0.926; Figure 3) between patients with and without VTE.
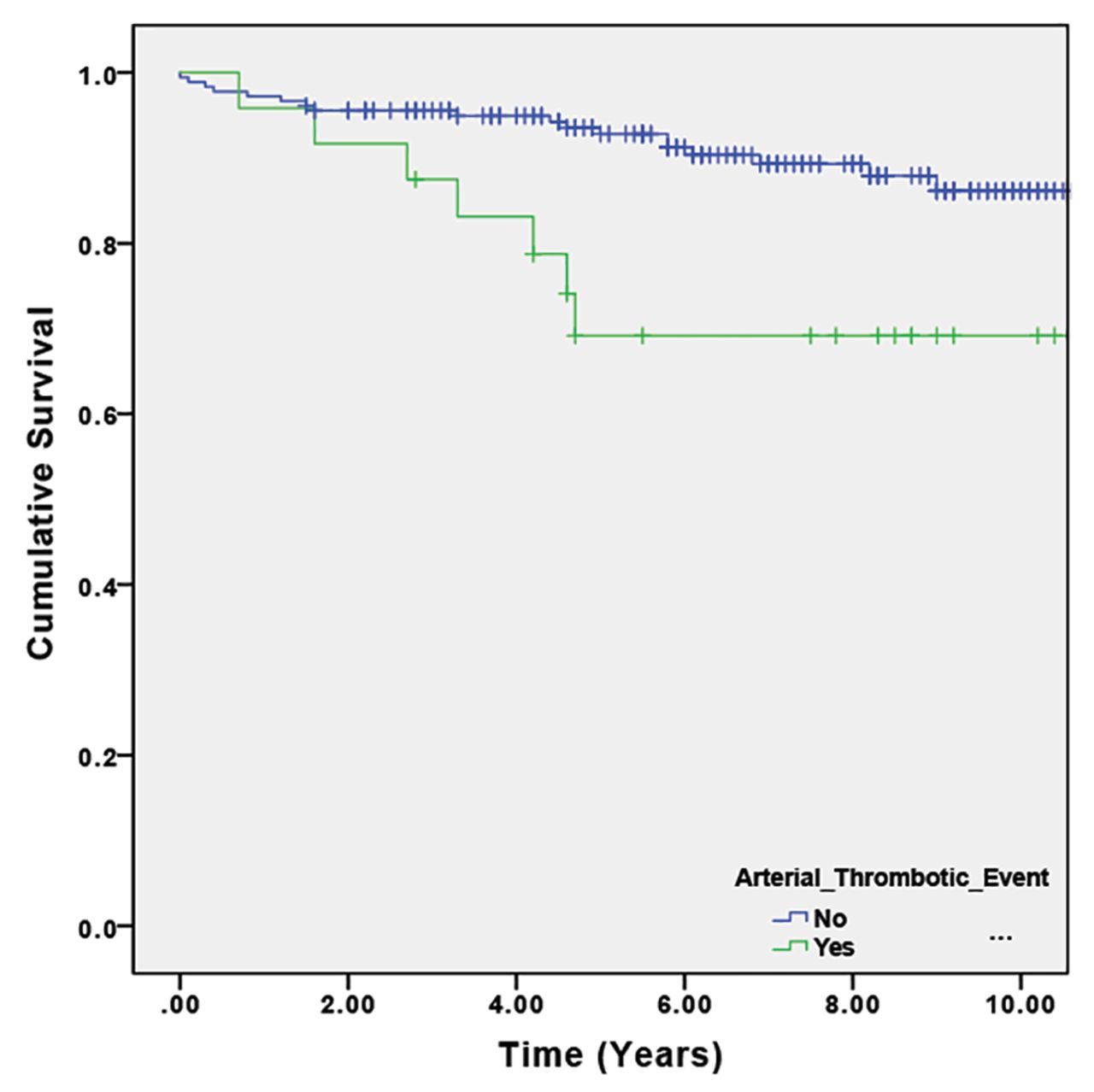
Kaplan-Meier curves for unadjusted patient survival in patients with and without arterial thrombotic events (p = 0.007 on log-rank test).
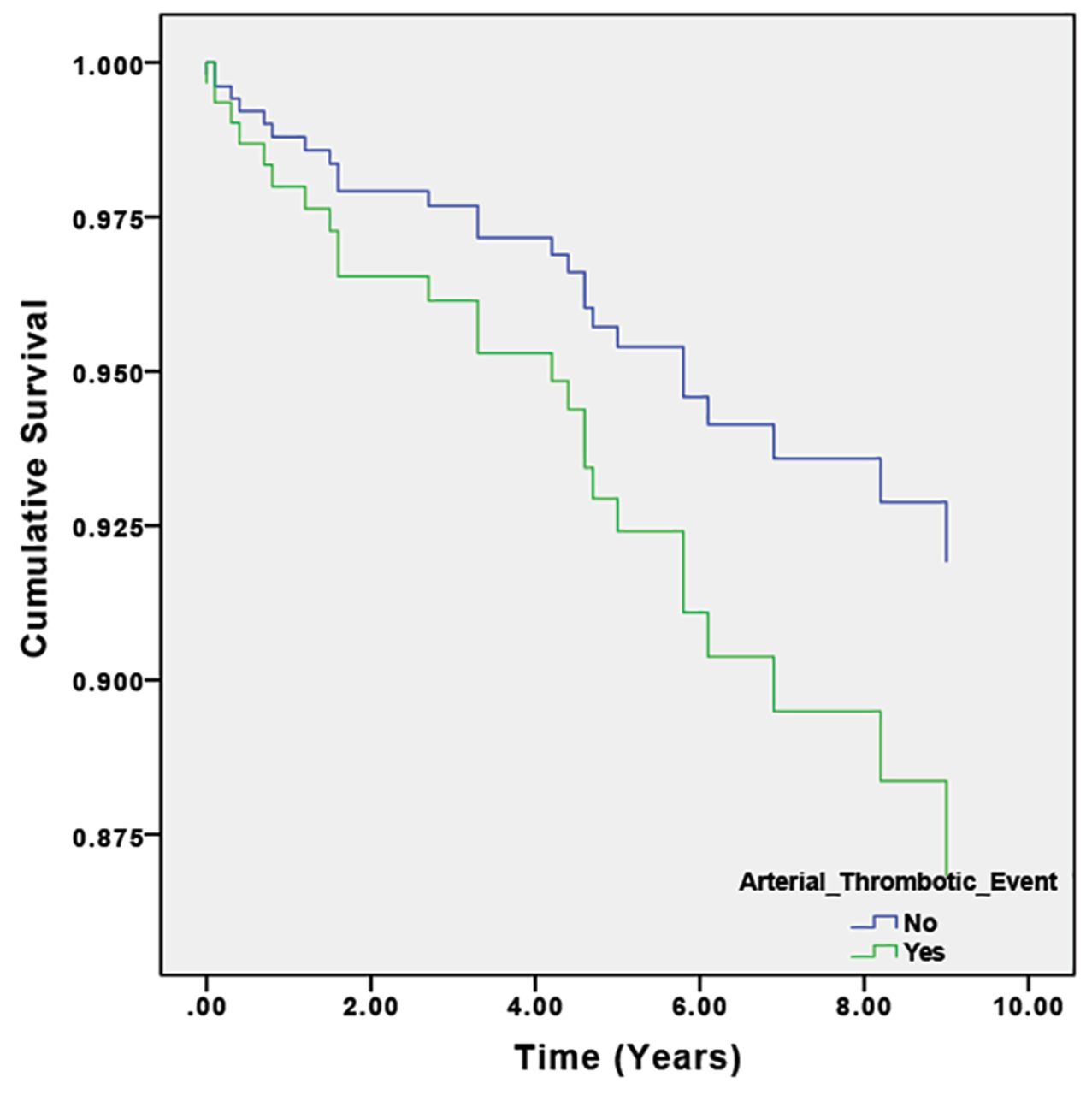
Cox proportional hazards regression curves describing longterm survival in patients with and without ATE, adjusted for age, prior ischemic heart disease, and renal replacement therapy at presentation (p < 0.001 for presence of ATE). ATE: arterial thrombotic events.

Kaplan-Meier curves for unadjusted patient survival in VTE and no VTE groups (p = 0.926 on log-rank test). VTE: venous thromboembolism.
DISCUSSION
Arterial thrombosis
The incidence of ATE in our study group was 2.67/100 PY (1.56 for acute coronary events and 1.10 for ischemic stroke). On multivariate analysis, only prior IHD and age were associated with future ATE. Among patients without prior IHD, the incidence of ATE was still raised compared to the general population at 2.32/100 PY (1.26 for coronary events and 1.06 for ischemic stroke). The median age for our cohort was 55 years.
We compared our rate of ATE in AAV to reported rates of ATE for the UK population (Table 3). Smolina, et al reported the age–standardized IR of acute coronary events as 0.15 per 100 PY for men and 0.07 per 100 PY for women among the general population in England in 201017. The rate of incident stroke (excluding persons with prior cardiovascular disease) was 0.10 per 100 PY in the UK in 200818. Our event rate for coronary events and incident stroke in AAV was 15- and 11-times higher than in the general population, respectively. Among the general population, the incidence of acute coronary events was highest in people with prior MI at 1.85 per 100 PY19. In people without prior MI, the IR of coronary events was 0.69 per 100 PY in people with chronic kidney disease (CKD) and 0.54 per 100 PY in people with diabetes. When we compared our results with this study, our rate of coronary events was similar to that in those with prior MI. In our cohort without prior IHD or stroke, the IR is double that reported by Tonelli, et al19 for people with CKD or diabetes. Therefore, it is unlikely that our event rate could be explained by these other risk factors alone. Power, et al20 reported the IR of stroke in hemodialysis patients at our center over a similar time period, and found an IR for first thrombotic stroke of 1.12 per 100 PY. Our event rate is similar in patients with vasculitis, most of whom did not require RRT [median creatinine 117 (IQR 73–268) µmol/l; 19% required RRT].
A high incidence of arterial thrombosis in inflammatory disorders has been described previously. Hinojosa-Azaola, et al studied the incidence of thrombosis in SLE in Canada and found an incidence of arterial thrombosis (defined as MI, cerebrovascular disease, peripheral vascular disease, and visceral infarction) of 0.7 per 100 PY21. Similarly, del Rincón, et al found an incidence of arterial thrombosis (defined as cardiovascular disease hospitalization including MI, stroke, other arterial occlusive events, or arterial revascularization procedures or death due to cardiovascular disease) of 3.43 per 100 PY in people with RA in the United States22. Allowing for differences in the definition of arterial thrombosis, our event rate in AAV appears similar to that reported in these studies of SLE and RA. Others have previously described an elevated incidence of ATE in patients with AAV9,10,11. Similar to Faurschou, et al (median population age 54.5 yrs)5, we found the incidence of arterial thrombosis was highest early in the disease course but remained elevated for at least 10 years. To our knowledge, we are the first group to describe an elevated IR for stroke; Faurschou, et al did not find a difference in event rates of stroke5. Morgan, et al9 (median population age 63 yrs) found a higher event rate for TIA but a similar event rate for stroke, when compared to CKD matched controls. We are the first, to our knowledge, to report an IR for ATE in AAV. Because these previous studies did not report incidence in PY, we were unable to compare our IR to these studies.
On univariate analysis, these were all independent predictors of ATE: age, prior IHD, VTE, admission at time of diagnosis, renal involvement, lack of ENT or eye involvement, ANCA type (MPO-positive), high CRP, high creatinine, and low albumin. However, on multivariate analysis, only prior IHD and age appeared to predict ATE. The lack of statistical significance of other factors found to be significant on univariate analysis could be due to a small event number and the disproportionate size of the groups.
Venous thrombosis
The incidence of VTE was 1.47 events per 100 PY in the first 10 years after diagnosis. This is about 20 times higher than the rate of VTE in the general population of the UK, reported by Huerta, et al as 0.075 events per 100 PY23. In our cohort, almost half (44%) of the events occurred in the first year after diagnosis (IR 3.8 per 100 PY). In years 2–10, the IR was 1.00 per 100 PY, which is lower than the first year, but still elevated compared to the reported incidence in the general population.
The high incidence of VTE in various inflammatory disorders has been described (Table 3). In SLE, studies have found an incidence of VTE between 0.5 to 3.6 events per 100 PY21,24,25,26. Similarly, the IR of VTE in RA is elevated at about 0.5 per 100 PY27,28. Our event rate in AAV appears similar to event rates in SLE and higher than that in RA. It has previously been reported that people with AAV have an increased risk of VTE. The Wegener’s Granulomatosis Etanercept Trial (WGET)3 was a multicenter randomized controlled trial in GPA performed in the US. Merkel, et al performed a substudy of this trial (WeCLOT) of 180 patients and found an IR of VTE of 7 per 100 PY (median population age 50 yrs)3. Weidner, et al8 performed a retrospective cohort study of 105 patients with AAV in Germany and found an incidence of 4.3 per 100 PY. Stassen, et al conducted a retrospective cohort study of 198 patients with AAV (excluding EGPA) in the Netherlands and found an IR of 1.8 per 100 PY, increasing to 6.7 per 100 PY during active disease4. Allenbach, et al performed a retrospective analysis of 1130 patients with AAV and polyarteritis nodosa (PAN) in France and found a higher incidence of VTE in AAV than PAN (1.84 vs 0.58 per 100 PY, respectively)7. A Danish study of 180 patients with GPA matched to population controls, performed by Faurschou, et al5, found an increased incidence of VTE in the first 2 years after diagnosis and increased incidence of DVT in the following years. There were 70% of events in the GPA cohort that occurred during active vasculitis. The study did not report absolute incidence per PY. The European Vasculitis Society (EUVAS)29 combined 4 randomized controlled trials to report VTE in 9.8% of their population (median population age 60 yrs). The IR was not reported.
When we compare our study to the previous studies, our VTE event rate was less than the WeCLOT3, EUVAS29, and Weidner8 studies, but similar to the Stassen4 and Allenbach7 studies. In the WeCLOT3, EUVAS29, and Stassen4 studies, patients were described as having, or having received treatment for, at least early systemic disease. Disease activity was described as a risk factor for VTE in the studies by Stassen4, Kronbichler29, and Faurschou5. In our study, patients were not selected for disease activity or severity; we included all patients without regard for disease severity and treatment received. Eighteen patients were diagnosed and initially treated at another hospital and then transferred to our unit. As a result, some patients did not have any periods of active disease during the followup period. A difference in disease activity may therefore have contributed to the difference in event rate between our study and the WeCLOT3 and Stassen4 studies. Similar to the study by Faurschou5, we found that the incidence of VTE was highest earlier in the disease course.
We are the first group to specifically look at rates of relapse, rather than periods of disease activity, and did not find a difference in VTE rates when comparing patients who had more frequent episodes of relapse to those that did not relapse.
Some of the previous studies focused on 1 syndrome such as GPA (Faurschou, et al5 and WeCLOT3). However, other studies looked at several subgroups of AAV (Morgan9, EUVAS29, Weidner8, Stassen4, and Allenbach7, et al). We did not find a statistically significant difference in the rate of arterial or venous thrombosis between subgroups of AAV and believe that all subgroups of AAV have an elevated rate of thrombosis. The RLV group appeared to have more ATE events in 7 out of 27 patients, compared with VTE events in 1 out of 27 patients. The RLV subgroup was older (median age 65 yrs compared with overall cohort median age 55 yrs), which may explain the increased frequency of ATE events.
Wattanakit, et al has demonstrated a correlation between stage of chronic kidney disease (CKD) and increased risk of VTE (excluding patients with endstage kidney disease)30, with an IR of 0.15, 0.19, and 0.45 per 100 PY for normal kidney function, mild CKD, and stage III/IV CKD, respectively. However, a large proportion of our cohort had acute kidney injury at presentation, rather than stable CKD, so direct comparison was not possible.
Strengths and limitations
We included all patients with AAV regardless of disease severity and type of treatment received, in a large and contemporary cohort. Our study provides an understanding of the incidence of arterial and venous thrombosis in patients with AAV. To our knowledge, we are the first group to describe the IR of arterial thrombosis in AAV and also the first to demonstrate a higher risk of stroke in AAV.
As with all retrospective cohort studies, we were reliant on prior documentation and cannot exclude the possibility that our event rate may be underreported if events were diagnosed outside of our unit and were not documented in case notes. Some important risk factors for arterial and venous thrombosis were not routinely tested at our clinic, such as lipid profile and body mass index, and therefore could not be included in our analysis. Similarly, the Birmingham Vasculitis Activity Score was not recorded in all patients’ records, so we were not able to relate disease activity scores directly to the risk of ATE and VTE. We were unable to ascertain the relative risk of ATE and VTE in comparison to an age- and estimated glomerular filtration rate–matched cohort without AAV. However, our main objective was to ascertain the risk relative to the general population.
People with AAV have a high rate of arterial and venous thrombosis compared to the reported rates for the general UK population, particularly in the first year after diagnosis. This early incidence may be related to disease activity or to its treatment. The role of antiplasminogen antibodies, reported by others in active disease, requires further investigation. Early thromboprophylaxis is not routinely given to this patient group because of bleeding risk, particularly from pulmonary hemorrhage or at the time of renal biopsy. Future studies should assess the patient benefits and risks of anticoagulation or antiplatelet agents in AAV. Our study highlights the importance of ATE and VTE as complications of AAV and suggests that its treatment should be considered in the care of these patients.
Footnotes
This research is supported by the UK National Institute for Health Research (NIHR) Biomedical Research Centre based at Imperial College Healthcare NHS Trust and Imperial College London. FWKT was supported by the Diamond Fund from Imperial College Healthcare Charity, and the Ken and Mary Minton Chair of Renal Medicine. MA was supported by NIHR and AT by the Wellcome Trust.
- Accepted for publication July 20, 2018.








{kind=link}
{kind=link}
{kind=link}