

Abstract
Objective. Cauda equina syndrome (CES) is a rare neurologic complication of longstanding ankylosing spondylitis (AS). It is unclear what causes CES, and no proven or effective therapy has been reported to date. We have encountered 6 patients with longstanding AS diagnosed with CES. We set about to study their features, review the literature, and generate hypotheses regarding pathophysiology, as well as to speculate on the possibilities of early recognition and prevention.
Methods. We obtained permission from 6 patients with longstanding AS and CES to access their medical records and imaging studies for research purposes related to this paper. We collected and reviewed each patient’s medical history, imaging studies, disease duration, past therapies especially those that relate to AS, laboratory data, as well as any treatment they received for CES and followup results of each case to the present time.
Results. The 6 cases of CES with AS have remarkable similarity to each other in that several decades of the disease had passed before neurologic symptoms and later signs appeared. All cases have fused spines and facet joints without spinal fractures, spinal stenosis, or disc herniation.
Conclusion. CES is a rare yet debilitating neurologic complication of longstanding AS. The pathophysiology and treatments are far from clear. We postulate that chronic enthesitis of the vertebral column initiates the process that results in dural stiffening and formation of ectasias, causing downstream nerve root damage.
Ankylosing spondylitis (AS) is characterized radiologically and pathologically in its late stages by fusion of the sacroiliac joints and ossification of tendons and ligaments at their sites of attachment to bones1,2,3. Nonmusculoskeletal manifestations include uveitis, pulmonary fibrosis, aortic valvular disease, and amyloidosis2,4. Neurologic complications of AS are reported to occur in 2.1% of patients and include atlanto-axial subluxation with spinal cord compression or pathologic fractures of the rigid spine causing neurologic deficits2,4.
Cauda equina syndrome (CES) is a rare neurologic complication of longstanding AS; its earliest descriptions appear to have been done by Bowie, Glasgow, and Hauge in 19615,6. Dural ectasia with or without nerve root adhesion to the enlarged dural sac is the typical finding seen on magnetic resonance imaging (MRI) and the main diagnostic feature associated with this condition7,8,9. It is unclear what causes CES, and no proven or effective therapy has been reported to date. It is assumed that dural ectasia with subsequent fibrosis of the dura mater is the result of chronic inflammation, which at one point becomes unrecoverable10,11,12,13,14. However, it is possible that unique features related to spinal and dural anatomy and the distribution of mechanical forces in the thoraco-lumbar spine taking place over time in patients with AS may have an as-yet-unrecognized contribution to the etiopathogenesis of CES.
Challenges related to the management of CES are almost overwhelming; case reports of patients treated with tumor necrosis factor inhibitors (TNFi), and lumboperitoneal shunting (LPS), have shown some effect, while other reports have revealed no improvement15,16,17,18,19,20. CES, a rare but nevertheless well-defined neurologic complication of longstanding AS, has an extremely important effect on physical function and patients’ quality of life. We have encountered 6 patients diagnosed with CES, all of whom have had longstanding AS. We set about to study their features in detail, review the literature, and generate hypotheses regarding why this event occurs, as well as speculate on the possibilities of early recognition and prevention.
MATERIALS AND METHODS
We obtained permission from 6 patients with longstanding AS and CES to access their medical records and imaging studies for research purposes related to this case series and review. One of the 6 patients had died, and her husband gave permission. All patients gave permission to discuss their cases with them to fill gaps where necessary. The process by which the investigators achieved access to personal health information from these subjects was approved by the Cedars-Sinai Institutional Review Board (IRB). No IRB or ethics approval was required.
We collected and reviewed each patient’s previous medical history, imaging studies, disease duration, past therapies (especially those that relate to AS), laboratory data, as well as any treatment they received for CES, and followup results of each case to the present time.
RESULTS
Patient demographics and characteristics are shown in Table 1 and Table 2. Patient 1 is a 70-year-old female with almost 40 years of AS who reported a very slow progression (over 14 yrs) of “pins and needles” sensations in the right foot. Symptoms progressed to involve the right leg along with increasing numbness. Eight years after symptom onset, she started experiencing a change in her bowel habits with more frequency and urgency, and then constipation. After 6 more years, she noticed slight weakness of the right quadriceps. She stopped playing competitive table tennis when the “pins and needles” sensation intensified, and numbness began to involve the buttock and perineum, and urinary urgency developed. She had been taking nonsteroidal antiinflammatory drugs (NSAID) and etanercept for her AS almost the entire time she had experienced the above neurologic symptoms. MRI of the lumbar spine showed diffuse bony fusion, and L1–L2 dural ectasia involving the right posterior elements with a posterolateral dural diverticulum. There was associated displacement of the distal conus, filum, and nerves of the upper cauda equina to the right, suggestive of associated tethering (Figure 1). She received 4 doses of infliximab (IFX) but stopped after shingles developed. Laminectomy with untethering was performed. Dural patch placement was performed; however, the patch dehisced weeks after the procedure. She did not experience relief in her symptoms with medical or surgical treatments. She now has chronic constipation and urinary retention that is being treated with medications. Physical activity, including prolonged sitting, is difficult for her at the present time.

A. T2-weighted sagittal scan of the lumbar spine demonstrating the conus terminating at the L1 level. B. T1-weighted noncontrast sagittal scan of the lumbar spine showing a widely patent spinal canal.
Demographic summary of 6 patients with cauda equina syndrome (CES).
Summary of duration of disease at diagnosis, clinical features, treatments, and responses in 6 patients with cauda equina syndrome (CES).
Patient 2 is a 69-year-old male with a 20-year diagnosis of AS who reported 2 years of numbness and tingling in bilateral lower extremities that progressed to involve the saddle region. Pain became dominant as well as numbness. Urinary and bowel incontinence began to develop, and he learned to self-catheterize for relief. He could ride his bicycle up to 50 miles on occasion prior to the diagnosis of CES. He used only NSAID for the treatment of his AS. Inflammatory markers were always normal. MRI of the spine disclosed multilevel remodeling and dehiscence of the posterior elements; there were multiple L1-S1 thecal sac sacculations with scalloping of the lamina, and disposition of the cauda equina into those sacculations. He continued to take NSAID without improvement of his symptoms and now requires a cane for ambulation.
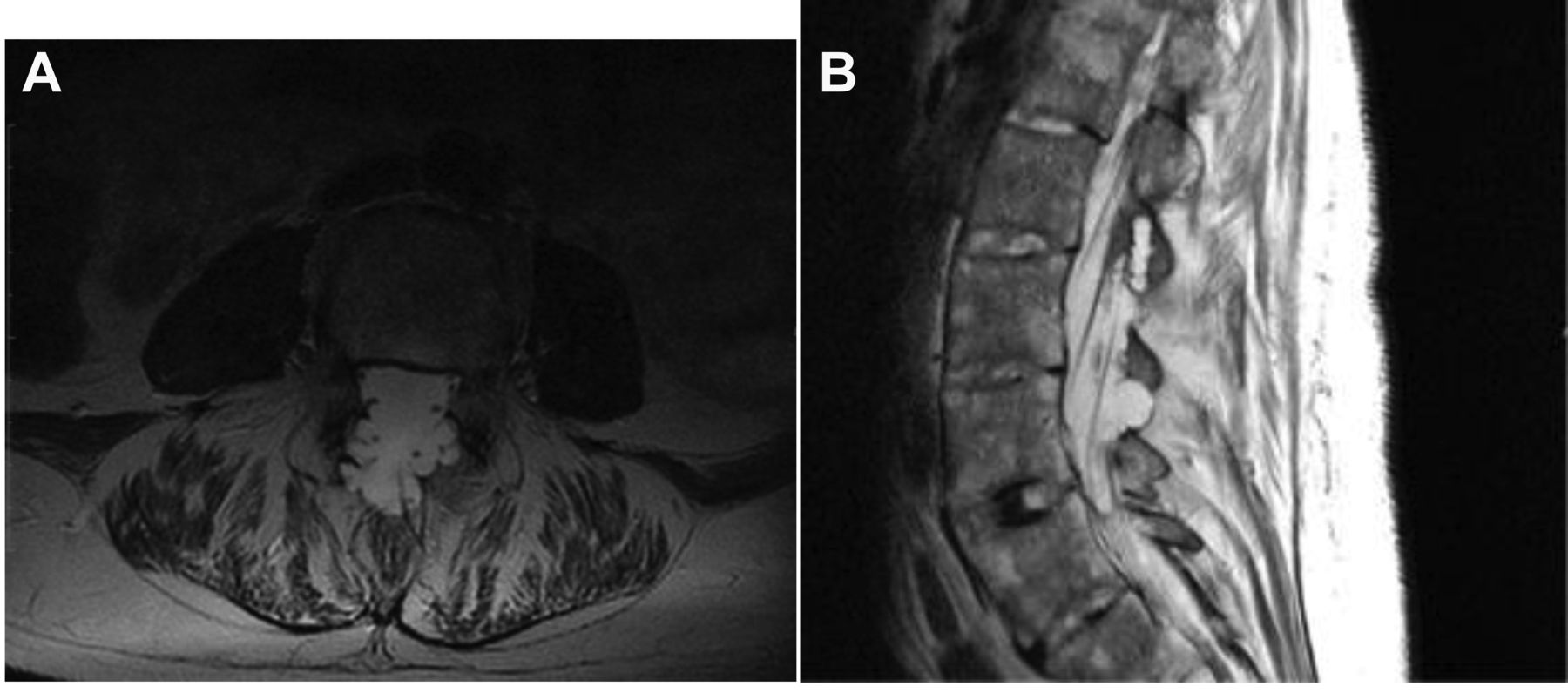
Patient 3 is a 69-year-old female (now dead) with over 30 years of AS, who presented with 2 years of numbness and pain in the right buttock radiating to the right lower extremity, as well as numbness of the left foot. She had associated weakness of the lower extremities and loss of sensation with urination and bowel movements. These symptoms caused her to use a cane and stop driving. Physical examination showed atrophy of the calf muscles, absent ankle jerk reflexes, and abnormal sensation testing. MRI revealed dural ectasia L2–L4 with adhesive arachnoiditis (Figure 2). She received a short 6-week course of adalimumab (ADA) without improvement. Laminectomy and epidural steroid injections did not help. Subsequently she was diagnosed with metastatic pancreatic cancer and died shortly thereafter.
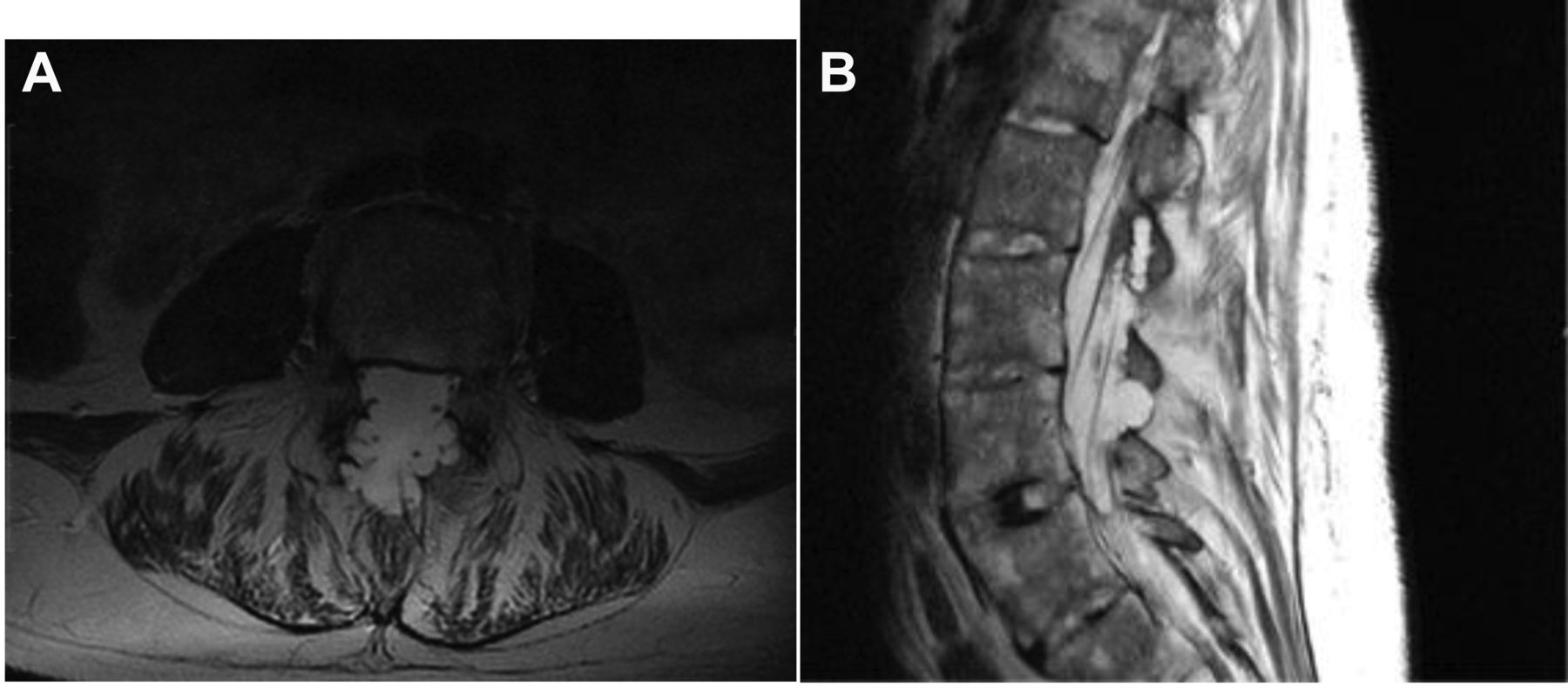
A. T2-weighted axial scan at the L4 level in the lumbar spine demonstrating posterior dural ectasia. B. T2-weighted sagittal scan of the lumbar spine showing the posterior location of the abnormalities with the normal contour of the anterior spinal canal.
Patient 4 is a 65-year-old male with almost 40 years of AS who presented with left foot drop associated with pain, numbness, weakness, and muscle atrophy over 4 years in duration. His symptoms extended proximally and began to involve the right side as well. Physical examination disclosed significant muscle atrophy, weakness, and abnormal sensation from the feet to the buttock. MRI revealed left-sided L1–L3 dural ectasia containing several descending nerve roots as well as compressing the L5-S1 nerve roots. He had a bone spur surgical removal due to concern about nerve impingement but without benefit. He received ADA with unexpected worsening of symptoms, and this treatment was stopped.
Patient 5 is a 70-year-old male with 40 years of AS who presented with 6 years of numbness and pain in the left foot that gradually ascended to involve the entire leg and groin. He also developed bladder, bowel, and sexual dysfunction. Because of the severity of his urinary issues, he had frequent urinary tract infections and nephrolithiasis. He now performs urinary self-catheterization. Physical examination reveals abnormal sensation in the left leg and absent ankle reflexes. MRI disclosed multilevel dural ectasias without tethering of the conus medullaris. He started ADA with subjective improvement in pain. Strength and sensation returned partially to the perineum at the time of his last assessment.
Patient 6 is a 69-year-old male with almost 30 years of AS who presented with numbness of the right foot that extended caudally, followed by weakness of the calf, as well as involvement of the left lower extremity and saddle areas. Prior to the diagnosis of CES, he travelled extensively to many national parks and participated in swimming and biking exercise activities. MRI demonstrated extensive L2–L5 dural ectasias. He underwent LPS with significant reduction in neuropathic pain; however, symptoms returned to previous levels 2 to 3 years following surgery. He now uses a cane to ambulate.
DISCUSSION
CES remains today a rare but devastating neurologic complication of longstanding AS21. Damage to the nerve roots appears to take place at the distal end of the spinal cord, resulting in sensory and/or motor deficits of the pelvis and lower limbs, including bladder and bowel dysfunction. Symptoms could develop rapidly, but most CES cases associated with AS take years to develop, resulting in delay in diagnosis.
There are no specific clinical or imaging criteria for the diagnosis of CES. The diagnosis is supported by symptoms and radiographic findings. MRI is the preferred modality21. A list of red flag symptoms used to diagnose CES includes low back pain, weakness, sensory loss or pain, saddle anesthesia, urinary or bowel dysfunction, sexual dysfunction, and reduced reflexes13.
In patients with CES but without AS, the process is most commonly caused by lumbar disc herniation22 with a pathogenesis understood to be underlying spinal canal narrowing with ligamentum flavum infolding22. Further injury to the nerves could be perpetuated by reactive inflammation from any process, subsequently leading to nerve root compression22,23,24. However, CES in patients with AS occurs without obvious spinal canal or foraminal narrowing, or disc herniation presenting the challenge to understand why it takes place.
The 6 cases of CES with AS described herein have remarkable similarity to each other in that several decades of the disease had passed before neurologic symptoms and later signs appeared. All cases have fused spines and facet joints without spinal fractures, spinal stenosis, or disc herniation. The diagnosis of AS was established in the patients’ early 30s but symptoms of back pain likely occurred much earlier. In addition, none of the cases displayed other extraspinal manifestations. Three of the 6 patients participated in very active recreational exercises. One case of CES developed while the patient was taking a TNFi; attempts at treatment of established signs and symptoms of CES with anti-TNF agents in the other cases did not reveal a pattern of success.
The pathogenesis of CES in AS is unknown. One proposed theory is that the meninges expand in response to cerebrospinal fluid (CSF) pulse pressure, allowing increased absorption of the CSF and subsequent dampening of the transmitted pressure variations12. Other suggested mechanisms include small-vessel angiitis of the vasa vasorum of the nerve roots, increased arterial pulsatile forces, or prior radiation treatments12. Koboyashi, et al25 studied cauda equina circulation of patients with neurogenic intermittent claudication in lumbar spinal canal stenosis using dynamic contrast-enhanced MRI; he and others found abnormal contrast extravasation, delayed arterial uptake, and venous pooling of contrast that suggest disruption of the blood-brain barrier, findings that often occur with chronic inflammation of any cause. It is possible, according to Koboyashi, that edema from vascular compromise occurs secondary to chronic enthesitis in various tissues of the spinal canal in AS subjects, which in turn causes irreversible damage to the spinal nerve roots over time25.
Recent attempts from clinical and imaging studies and animal model investigations to increase our understanding of the biomechanical basis for enthesitis do provide a unifying concept for enthesitis as a potential mechanism for development of CES in AS subjects3,26. The enthesis, a site of a ligament, tendon, or joint capsule attachment to bone, may be the pathway by which the loading forces of the spine can produce inflammation, setting in motion the cascade of events leading to nerve damage in patients with CES. Based on these newly evolving concepts of AS pathogenesis, we propose that enthesitis in tissues of the spine is the inciting event that leads to the multiple downstream sequelae resulting in CES in patients with AS. Primary AS inflammatory processes may extend to the dura mater from adjacent entheses, causing inflammatory changes to the blood-nerve barrier and adhesion of the dura mater to the surrounding structures, thereby resulting in reduction of compliance of the dural sac25,27. Stiffening of the dural sac would cause it to weaken over time, encouraging the development of ectasias28. The combination of mechanical distribution of the forces in the thoraco-lumbo-sacral spine, increased pressure in the lower vertebral column from a fused spine, associated edema, and reduced dural compliance, all of which could cause the formation of dural ectasias29. Because more ligaments are found in the lateral-posterior portions of the spinal canal, it is possible that more enthesitis occurs in these regions and weakening of these structures results in the common finding of posterior sacculations on imaging. Displacement, tethering, and vascular damage to the nerve roots over time could result in CES.
For patients who have been taking biologic therapy with quiescent disease for years and then develop CES, one can argue that inflammation may not be the primary initiating event. However, it is likely that weakening of the dural sac would have already occurred prior to initiation of biologic therapy, because in almost all cases CES develops in AS patients with complete fusion of the spine. This suggests a prolonged latency period from clinically active disease to development of CES following decades of apparent clinical remission.
A review of the anatomy of the spine segments involved in AS does provide us with a critical view of where and when CES may take place. There are 3 major ligaments in the spine: the anterior longitudinal ligament that runs along the front of the vertebral bodies, the posterior longitudinal ligament behind the vertebral bodies, and the ligamentum flavum that covers the dura mater and connects under the facet joints13. These critical ligaments connect bones or cartilage elements together, providing stability to a joint during rest and movement.
The posterior longitudinal ligament is intimately adherent to the fibrocartilages and contiguous margins of the vertebrae and is connected to the most superficial layer of the meninges, the dura mater13. The dura has 2 layers: the superficial layer, which serves as the skull’s inner periosteum, and a deep meningeal layer13. When the dura covers the spinal cord, it is known as the dural or thecal sac. The dura also becomes the epineurium at the level of the dorsal root ganglion. The next layer of meninges is the arachnoid mater, which lines the dural sac13. The third and deepest layer of the meninges is the pia mater, which closely covers the brain, spinal cord, and the nerve roots, and eventually forms the filum terminale, which arises from the conus medullaris and anchors the spinal cord to the coccyx. The cauda equina consists of nerve roots distal to the conus and containing afferent dorsal sensory fibers and efferent ventral motor fibers. These nerve roots enter the spinal cord through both sides of the vertebral bodies, with every added cephalad nerve root displacing subsequent distal nerve roots posteriorly, maintaining the orientation of motor fibers being anteromedial, and sensory fibers posterolateral13.
From an appreciation of the complex mechanical anatomy of the spine, we observe that the ligaments of the vertebral column are closely associated with the meninges; therefore, enthesitis of the vertebral column would necessarily affect the nerve roots. Weakening of the ligaments and underlying meninges could occur both from inflammation and erosion as well as from mechanical tension on the spinal connective tissue from rigidity created by ankylosis. Zarzur28 observed that the posterior lumbar dura mater was easily distensible only in the transverse direction. Therefore, fusion of the spine may limit the ability of the dura to redistribute pressure; this observation, in part, may explain the specific mechanical contributions to the formation of posterior dural sacculations. We could not examine whether ossification or calcification of the posterior longitudinal ligaments occurred in our patient cohort because of insufficient computed tomography imaging data.
The work of Tan, et al30,31,32 suggests that syndesmophytes (SM) are nonrandomly distributed around the disc margins, and they occurred most often at the posterolateral rim. We would expect random distribution of SM if they were formed solely in response to inflammation. Further, orthopedists and biomechanical engineers cite this area as the middle column of the spine where mechanical stress is concentrated at the base of the pedicles. Therefore, these observations suggest that mechanical forces in this area of the spine may be important for SM’s initiation as well as in spinal enthesitis.
There has been no demonstrated effective medical or surgical treatment for CES once it occurs in AS20. Ahn, et al20 performed a metaanalysis for treatment effects of CES in AS and found that steroids had not been effective. While NSAID appeared to improve symptoms, they did not alter neurologic deficits20. Others reported improvement after treatment with IFX, but this is not consistent across reports17. Surgical intervention such as LPS, untethering, and laminectomy also have achieved inconsistent results15,16. Some experts have suggested early medical treatment is crucial for making as full a recovery as possible for typical CES, especially in those who have evidence of active inflammation33. Unfortunately, early diagnosis is difficult, and treatments succeed inconsistently. The degree of recovery is limited even in those who have a partial response.
This information raises the question of when CES should be suspected in patients with AS. The following questions need to be addressed if we are going to understand how to diagnose and manage this condition. How and when do we screen, predict progression, and differentiate CES from other causes of pain and neuropathy? Is it too late to intervene when patients display the initial symptoms of neuropathy — when chronic inflammation presumably has already taken place? Are physical mechanical forces on the spine a major cause of CES in AS? Future attempts to identify at-risk patients early may help us understand more about CES pathogenesis and treatment options.
CES is a rare yet debilitating neurologic complication of longstanding AS and the pathophysiology and treatments are far from clear. Herein we reported 6 patients with CES and AS, and reviewed current understanding of the pathogenesis of CES in AS. We postulate that chronic enthesitis of the vertebral column initiates the process that results in dural stiffening and formation of ectasias, causing downstream nerve root damage. Mechanical force transduction in the spine may play a pivotal etiologic role.
- Accepted for publication March 19, 2019.








{kind=link}
{kind=link}