

Abstract
Objective. Evaluate enthesitis, physical function, and health-related quality of life (HRQOL) among patients with psoriatic arthritis (PsA) who are naive to anti–tumor necrosis factor agents.
Methods. In PSUMMIT 1 and 2, patients with PsA were randomized to placebo or ustekinumab 45 mg or 90 mg. Enthesitis was assessed at weeks 0 and 24 (Maastricht Ankylosing Spondylitis Enthesitis Score). Assessments included Health Assessment Questionnaire–Disability Index (HAQ-DI), Medical Outcomes Study Short Form-36 (SF-36) physical component summary/mental component summary (PCS/MCS), and American College of Rheumatology 20 (ACR20).
Results. At Week 24, 21 had worsened enthesitis, 158 had improved enthesitis, and 412 had unchanged enthesitis. Improved enthesitis was associated with improvements in HAQ-DI and SF-36 MCS. Results were similar for ACR20 responders and nonresponders.
Conclusion. Improvement in enthesitis at Week 24 was associated with improvements in physical function/HRQOL regardless of ACR20 response.
Enthesitis, inflammation at the insertion of tendons, ligaments and joint capsules, is a common manifestation of psoriatic arthritis (PsA)1. Pain arising from enthesitis has been associated with increased pain scores overall and a worsened quality of life compared with patients who do not have enthesitis2. In the phase III PSUMMIT 13 and PSUMMIT 24 trials, patients with PsA who received ustekinumab had significantly greater improvement in the signs and symptoms of PsA, including enthesitis, than did patients who received placebo. Moreover, ustekinumab-treated patients had greater improvement in physical function and health-related quality of life (HRQOL). To further examine the relationship between enthesitis and physical function and HRQOL, we performed a posthoc analysis using combined data from the PSUMMIT trials.
MATERIALS AND METHODS
Patients and study design
The patient inclusion criteria and study designs for the PSUMMIT 13 and PSUMMIT 24 trials have been previously described. Briefly, in both studies, adults were eligible if they had active PsA for ≥ 6 months despite ≥ 3 months of therapy with disease-modifying antirheumatic drugs or ≥ 4 weeks of therapy with nonsteroidal antiinflammatory drugs, or intolerance to these therapies. PSUMMIT 1 included only biologic-naive patients; in PSUMMIT 2, prior therapy with an anti–tumor necrosis factor (TNF) agent for ≥ 8 weeks (etanercept, adalimumab, golimumab, or certolizumab pegol) or ≥ 12 weeks (infliximab) was permitted. In both trials, eligible patients were randomized to receive subcutaneous injections of placebo, ustekinumab 45 mg, or ustekinumab 90 mg at weeks 0 and 4 and every 12 weeks thereafter. Patients in the placebo group crossed over to ustekinumab 45 mg at Week 24. At Week 16, patients with < 5% improvement from baseline in both tender and swollen joint counts entered double-blind early escape, such that patients in the placebo group received ustekinumab 45 mg, and patients in the ustekinumab 45 mg group received ustekinumab 90 mg; patients in the ustekinumab 90 mg group did not have any adjustments in study treatment regardless of early escape status.
Both PSUMMIT 1 (NCT01009086) and PSUMMIT 2 (NCT01077362) were conducted in accordance with Good Clinical Practices and the Declaration of Helsinki. The protocol was approved by the ethics committee or institutional review board (IRB) at each site. Patients were required to give written informed consent before study-related procedures were performed. Centralized IRB approval was managed primarily by Copernicus Group IRB in the United States (approval numbers: PSUMMIT 1, CEN1-09-416; PSUMMIT 2, CEN-09-487) and Research Review Board in Canada (approval numbers: PSUMMIT 1, 2009.275; PSUMMIT 2, 2009.288).
Assessments
In the PSUMMIT studies, enthesitis was assessed using the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES) index5. Enthesitis at each site recorded in the MASES instrument was scored only as either present or absent in each site. Physical function was evaluated using the Health Assessment Questionnaire–Disability Index (HAQ-DI), and general HRQOL was assessed using the Medical Outcomes Study Short Form-36 (SF-36) physical and mental component summary (PCS and MCS, respectively) scores. The proportion of patients with ≥ 20% improvement in the American College of Rheumatology criteria (ACR20)6 was determined at Week 24 to assess overall clinical response.
Statistical analysis
In this posthoc analysis, to have adequate sample size, patients from both studies were included. The population was limited to patients who were biologic-naive (all 615 patients in PSUMMIT 1 and 132 of 312 patients in PSUMMIT 2). This analysis excluded patients who met the early escape criteria and those who did not have enthesitis data available at either baseline or Week 24. Thus, data from 591 patients (PSUMMIT 1, n = 493; PSUMMIT 2, n = 98) were analyzed. The number of body sites with enthesitis was assessed at baseline and Week 24, and categorized as worsened (greater number of sites with enthesitis present at Week 24), improved (fewer sites with enthesitis present at Week 24), or unchanged (same number of sites with enthesitis present at both baseline and Week 24 or no enthesopathy present at both baseline and Week 24). Patients with missing data at either Week 0 (placebo, n = 1; combined ustekinumab, n = 1) or Week 24 (placebo, n = 21; combined ustekinumab, n = 19) were included in the unchanged category.
RESULTS
A total of 591 patients (PSUMMIT 1, n = 493; PSUMMIT 2, n = 98) were included in this analysis (Table 1). The proportion of patients with enthesitis at baseline was similar between the placebo group (72.3%) and the combined ustekinumab group (72.2%). At Week 24, 21 patients (placebo, n = 10; ustekinumab, n = 11) had a worsened enthesitis status relative to baseline, and 158 patients (placebo, n = 33; ustekinumab, n = 125) had an improved enthesitis status (Table 2). A total of 412 patients (placebo, n = 134; ustekinumab, n = 278) were classified as unchanged; 131 patients (placebo, n = 34; ustekinumab, n = 97) did not have enthesitis at both baseline and Week 24; 239 (placebo, n = 78; ustekinumab, n = 161) had enthesitis at both baseline and Week 24, and 42 patients had missing data either at baseline (n = 2) or Week 24 (n = 40). Among all patients, 44.8% were female, and the mean age was 47 years. Baseline demographic and disease characteristics were generally similar among the 3 enthesitis status groups (Table 1). Among patients with worsened or unchanged enthesitis, distal interphalangeal joint arthritis was more common when compared with patients who had improved enthesitis (Table 1).
Baseline demographic and disease characteristics of biologic-naive patients from PSUMMIT 1 and PSUMMIT 2.
Changes in HAQ-DI, SF-36 PCS, and SF-36 MCS at Week 24 among patients with improved, worsened, or unchanged enthesitis.
The mean percent improvement in HAQ-DI score at Week 24 was greater among patients with improved enthesitis (42.0%) compared with patients whose enthesitis was worsened (19.3%; p = 0.030) or unchanged (19.6%; p < 0.001). The mean change in SF-36 PCS score at Week 24 for patients with improved enthesitis (7.0) was greater than that in the unchanged group (4.6; p < 0.001) and numerically greater than that in the worsened group (5.2; p = 0.425); however, this difference did not meet statistical significance. The mean change in SF-36 MCS score was greater for patients with improved enthesitis (4.8) compared with patients in the worsened group (−1.1; p = 0.010); the mean change in SF-36 MCS score in the unchanged enthesitis group was numerically lower, but did not reach statistical significance (4.1; p = 0.155; Table 2).
At Week 24, the mean percent improvement in HAQ-DI and mean improvement in SF-36 PCS score were greater in patients who achieved an ACR20 response compared with ACR20 nonresponders in all 3 enthesitis subgroups (Figure 1). Mean changes in SF-36 MCS score were similar between ACR20 responders and nonresponders for patients with worsened or improved enthesitis. For patients with unchanged enthesitis, ACR20 responders had a greater mean improvement in SF-36 MCS score than did ACR20 non-responders. Among ACR20 responders, improvements in HAQ-DI and SF-36 PCS scores were numerically greater for patients with improved enthesitis compared with those with worsened or unchanged enthesitis (Figure 1). A similar trend was observed for improvements in HAQ-DI and SF-36 MCS among ACR20 nonresponders; however, mean changes in SF-36 PCS scores were similar among the 3 enthesitis subgroups for ACR20 nonresponders (Figure 1).
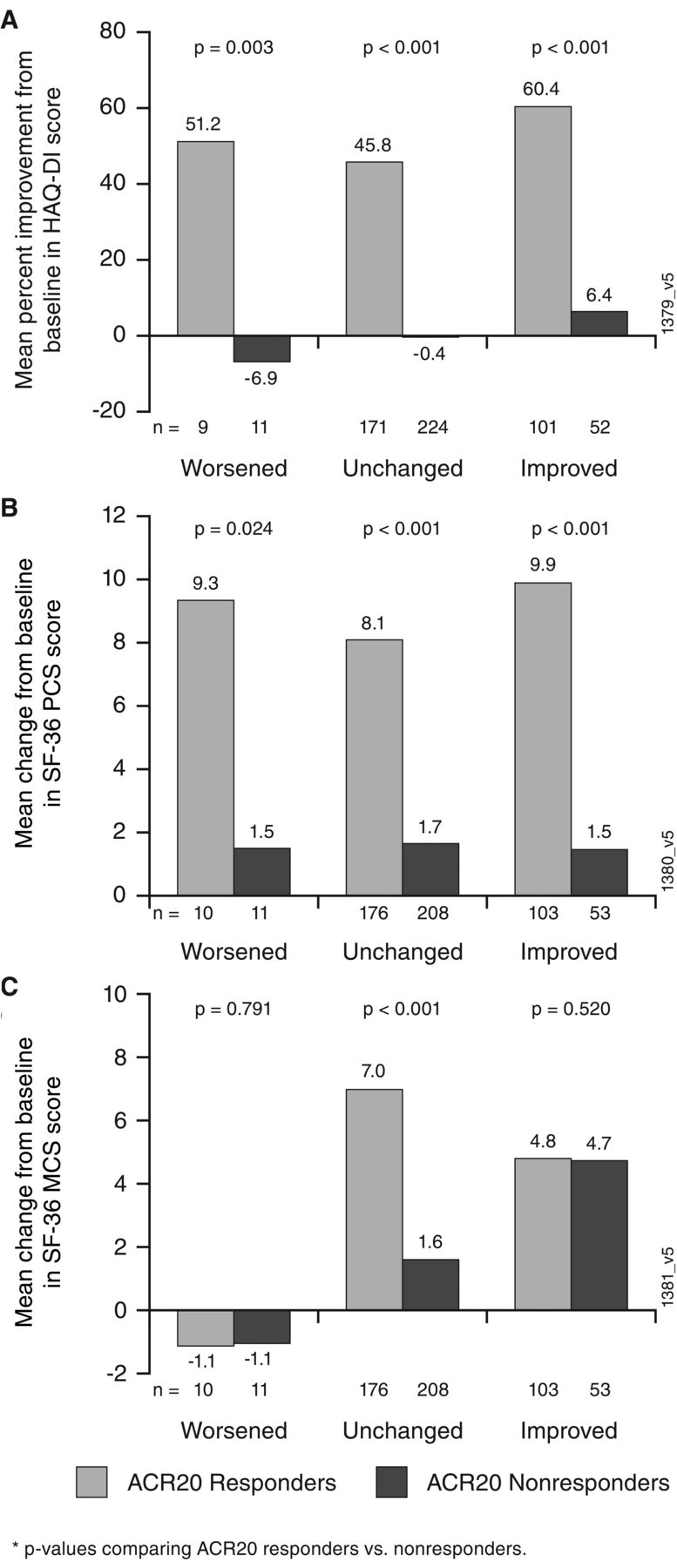
Percent change from baseline in HAQ-DI (A), mean change from baseline in SF-36 PCS score (B), and mean change from baseline in SF-36 MCS score (C) for ACR20 responders and ACR20 nonresponders with an enthesitis status of worsened, unchanged, or improved at Week 24. ACR20: ≥ 20% improvement in the American College of Rheumatology criteria; HAQ-DI: Health Assessment Questionnaire–Disability Index; SF-36 PCS/MCS: Medical Outcomes Study Short Form-36 Health Survey physical/mental component summary.
DISCUSSION
It has been estimated that over one-third of patients with PsA experience enthesitis1. Enthesitis has been associated with greater peripheral joint damage and axial damage7 and has also been associated with increased HAQ-DI scores, pain, and fatigue as well as greater work impairment2. In this exploratory analysis of anti–TNF-naive patients with PsA from the PSUMMIT 1 and PSUMMIT 2 trials, improvement in enthesitis was associated with improvements in physical function and HRQOL at Week 24. Patients who achieved an ACR20 response generally had greater improvements in physical function and HRQOL than did ACR20 nonresponders. However, patients with improvement in enthesitis had numerically greater improvements in HAQ-DI scores compared with those who had unchanged or worsened enthesitis, regardless of ACR20 response. Thus, some patients may still receive clinical benefit from treatment despite not reaching an ACR20 response. This emphasizes the need to consider the distinct tissue compartments that characterize the clinical phenotypes prevalent in a PsA clinic8.
These results are limited by the exploratory nature of the analysis and the relatively small numbers of patients in some groups; the PSUMMIT 1 and 2 trials were not powered for these comparisons. Additionally, the assessment of enthesitis in this analysis was limited to the presence or absence of enthesitis and did not reflect absolute changes in score. However, these results provide insight into the role of enthesitis in HRQOL and physical function in PsA, which is important for patients and their clinicians.
Acknowledgment
The authors thank Kezhen L. Tang, PhD (Janssen Research & Development LLC), for statistical support, and Rebecca E. Clemente, PhD (Janssen Scientific Affairs LLC), for writing support.
Footnotes
This study was funded by Janssen Research & Development LLC. Janssen Biotech Inc. manufactures ustekinumab.
IBM has received consulting fees from AbbVie, Janssen, Novartis, Pfizer, and UCB. LP has received consulting fees or speaker fees or served as an investigator or advisory board member for AbbVie, Almirall, Amgen, Baxalta, Biogen, Boehringer-Ingelheim, Celgene, Gebro, Janssen, Leo-Pharma, Lilly, Merck-Serono, MSD, Novartis, Pfizer, Regeneron, Roche, Sandoz, and SUN Pharmaceutical Industries. ABG has received consulting fees and served as an advisory board member for AbbVie, Janssen, Lilly, Novartis, and UCB, and has received research/educational grants from Janssen, Novartis, and UCB. CTR has received research grants, consulting fees, or speaker honoraria from AbbVie, Amgen, Janssen, Novartis, and UCB. AK has received consulting fees and research support from AbbVie, Amgen, Janssen, Lilly, Novartis, Pfizer, and UCB. PR has received consulting fees from Abbott, AbbVie, Amgen, BMS, Celgene, Janssen, Lilly, Novartis, Pfizer, and Roche. SK and GJM are or were employees of Janssen Scientific Affairs LLC when this work was performed and own stock in Johnson & Johnson, of which Janssen Research & Development LLC is a wholly-owned subsidiary. MS and YY are employees of Janssen Research & Development LLC, and own stock in Johnson & Johnson.
- Accepted for publication March 19, 2019.








{kind=link}