

Abstract
Objective. Establishing a research agenda on standardizing pain measurement in clinical trials in rheumatic and musculoskeletal diseases (RMD).
Methods. Discussion during a meeting at the Outcome Measures in Rheumatology (OMERACT) 2018, prepared by a systematic review of existing core outcome sets and a patient online survey.
Results. Several key questions were debated: Is pain a symptom or a disease? Are pain core (sub)domains consistent across RMD? How to account for pain mechanistic descriptors (e.g., central sensitization) in pain measurement?
Conclusion. Characterizing and assessing the spectrum of pain experience across RMD in a standardized fashion is the objective of the OMERACT Pain Working Group.
Pain is a prevailing and common symptom across rheumatic and musculoskeletal diseases (RMD)1. Clinically, acute and chronic pain are distinct, are managed differently, and have differences in outcomes. The majority of people who experience acute pain tend to improve spontaneously or under treatment2, but some individuals progress to a chronic pain that can cause considerable physical, emotional, and socioeconomic burdens3. To identify preventive or effectively tailored interventions, standardized pain assessment in clinical trials is essential to making precise estimates on the effectiveness of interventions. However, heterogeneity in outcome assessment has been identified for clinical trials in patients within and between different pain conditions4.
The OMERACT Filter 2.05,6 provides guidance for harmonizing outcome assessment by developing core outcome sets (COS) consisting of domains and measurement instruments. Defining the scope of such a COS is the initial step by identifying the domains that constitute the health condition of interest. For pain conditions, several COS recommendations exist, regarding chronic pain in general7,8, fibromyalgia (FM)9, low back pain (LBP)10, or for specific treatments11. To establish a research agenda for harmonizing pain assessment in clinical trials in RMD, information is needed regarding:
The importance of chronic pain in patients with RMD;
To what extent patients with chronic pain and RMD feel different from patients with chronic pain of other origin;
Whether the pain experience is different across RMD;
The existing pain recommendations in COS for RMD;
To what extent pain measurement differs across RMD;
The relative contribution of different pain mechanisms (e.g., central sensitization, neuropathic pain) to the patient’s experience of pain.
Methods, Results, and Meeting Report
Establishing a research agenda was planned for the OMERACT Meeting in Terrigal, Australia, in May 2018. In preparation, the OMERACT Pain Working Group had multiple teleconferences, and conducted an online survey in patients with RMD and a systematic review of existing pain recommendations in COS for RMD.
Introduction of the OMERACT 2018 Special Interest Group (SIG)
PJM introduced the precursor working group that developed a COS for FM9 and proposed a composite measure of disease activity to assess the COS12. This group described the multidimensional characteristics of this chronic pain disorder by listing the following items in the COS: pain, fatigue, sleep disturbance, patient’s global, multidimensional function, and quality of life. This COS was noted to be closely correlated to the Initiative in Methods, Measurements and Pain Assessment in Clinical Trials (IMMPACT) COS for evaluation of chronic pain conditions in clinical trials7,8,13.
Following this previous work, a working group has met as a SIG at subsequent OMERACT meetings to address the possibility of developing a COS for chronic pain across all RMD. Nevertheless, several inherent problems exist in this standardization process. First, pain may be acute and episodic in some RMD and chronic in others. In the latter situation, pain may become a disease unto itself, including chronic alteration of signaling pathways in the central nervous system rather than an episodic symptom of peripheral pathophysiology of an RMD. It has been demonstrated that chronic central pain can influence RMD outcomes14. Characterizing and assessing the spectrum of pain experience across RMD in a standardized fashion was highlighted as the objective of this working group, consisting of academic pain researchers and patient research partners.
Importance and experience of chronic pain in RMD
An online survey (one round between April and May 2018) was held to investigate the characteristics and relevance of chronic pain in patients with RMD. The questionnaire was developed by 1 SIG member (UK) and revised by others (BH, MG, MdW, MC, EC, LSS, PJM, AC) with SurveyMonkey, and data were analyzed with frequencies of responses and qualitatively. The majority of patients (84%) reported experiencing an RMD and chronic pain, and 86% expressed that chronic pain is relevant for patients with various RMD (Table 1). The majority of the patients (47%) reported that chronic pain is a common, inseparable aspect of RMD.
Characteristics and results of an online survey in patients with RMD.
In a previous survey13, individuals experiencing chronic pain (n > 800) identified 19 (sub)domains to be related to and affected by chronic pain. Similar results were provided by patients with RMD (Table 2, Figure 1)1. The most important domains (i.e., staying asleep, enjoyment of life, and fatigue, mean ≥ 8/10, rating between 0 “not important at all,” 10 “of highest importance”) also scored among the highest in the previous survey. The most substantial distinction between respondents with RMD and chronic pain was found for “weakness” and “difficulties concentrating” (Table 2); such difference may be explained by the fact that only a minority of patients presented with an RMD in the previous survey (i.e., 5% rheumatoid arthritis, 19% osteoarthritis)13. Patients also felt that a specific treatment of chronic pain in RMD would be necessary (median 7/10). The majority of patients (72%) expected treatment of chronic pain to have different aims than other treatments for RMD.
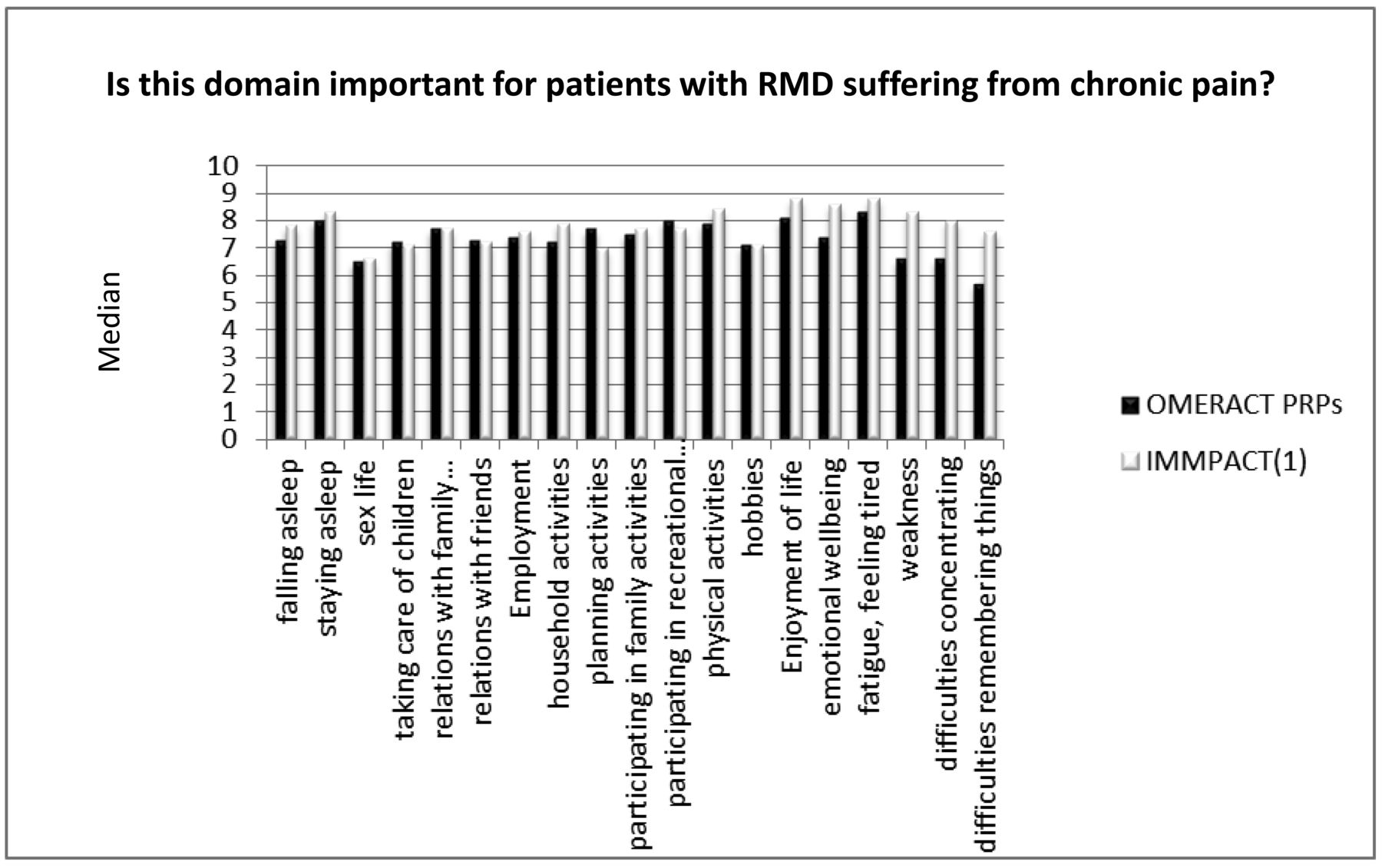
Importance of subdomains regarding the experience of chronic pain in patients with RMD and patients from a previous IMMPAT online survey. RMD: rheumatic and musculoskeletal diseases; IMMPACT: Initiative in Methods, Measurements and Pain Assessment in Clinical Trials; OMERACT: Outcome Measures in Rheumatology; PRP: patient research partners.
Importance (0 not important, 10 of highest importance) of subdomains regarding the experience of chronic pain in patients with RMD and patients from a previous IMMPACT online survey.
COS for RMD
Our aim was to identify any COS for research or practice targeting any RMD. An ad-hoc multifaceted search strategy to retrieve COS in MEDLINE and SCOPUS [developed by the Core Outcome Measures in Effectiveness Trials (COMET) initiative15] was run on March 6, 2018; results were screened to identify eligible COS. Additionally, the COMET database was searched with the keyword “pain.” Two independent reviewers (AC, UK) performed the screening. The methodological quality of a subset of 14 retrieved COS was assessed by 2 reviewers (EG, JK) with the Core Outcome Set-STAndards for Development (COS-STAD) recommendations16. One reviewer (AC) extracted data on the targeted RMD and/or intervention(s), on the frequency of pain recommendation, and on the specific pain (sub)domains recommended.
Fifty-one COS were retrieved, targeting 37 different RMD. Seven (14%) focused on a specific intervention. None of the 14 COS assessed with COS-STAD met all the minimum quality standards (median 6/11, interquartile range 5–8). Thirty-seven COS (73%) proposed pain as a core outcome domain; in 25 COS it was just labeled “pain,” in 10 “pain intensity” was recommended, in 3 “pain frequency/temporal aspects of pain,” and in other 3 “pain interference.”
Pain intensity measurement
AC reported results of an external group, published elsewhere17,18, regarding pain intensity measurement for LBP as an example of issues to consider when deciding about measurement instruments for pain domains. This initiative recommended “pain intensity” as a core outcome domain, consisting of perspectives from clinicians, researchers, and patients10. The 3 most common and frequently recommended measures [i.e., visual analog scale, numeric rating scale (NRS), and pain severity subscale of the Brief Pain Inventory] were assessed in a systematic review18. High-quality evidence was found only for the NRS measurement error, while the evidence on all other measurement properties was lower quality17. In a subsequent Delphi, consensus (75%) was found on endorsing the NRS as a core outcome measure for pain intensity in LBP trials, with the emphasis (96%) on average intensity over the last week18.
Discussion, Conclusion, and Next Steps
Although it is clear that chronic pain is felt by patients as a considerable concern and a separate aspect of RMD, a consensus on whether pain is understood as a symptom or a disease cannot be easily achieved in the rheumatology field19. According to the International Classification of Diseases, 11th ed. classification, chronic pain is considered a separate health condition when meeting specific criteria20. The pain academic community has already acknowledged pain as a symptom, but also chronic pain as a complex condition with multiple components affecting all aspects of functioning. Hence, the experience of chronic pain in RMD seems to be close to those of chronic pain from other origins, but more evidence on patients’ view is still needed.
The existing number of COS recommendations in RMD hampers the original idea of harmonizing chronic pain assessment by OMERACT. It seems to be helpful to consider existing work and support future advancements of existing initiatives. An important field of research is identified in the investigation of the measurement properties of existent pain scales. Two important questions arise from previous discussions about pain measures: (1) the validity of the pain construct and (2) the lacking evidence on measurement properties of commonly applied scales. The validity of the pain construct has been questioned in other fields, regarding aspects such as pain (sub)domains and pain stages (worst, average, etc.). This may explain why measurement properties lack sufficient evidence base.
During preparatory work and the last 2 OMERACT meetings, the pain working group has identified various subjects for research, 3 of which may represent the future work of the group:
Following the surveys’ results, beyond pain domains, are there other items (e.g., fatigue, sleep) to be measured consistently in RMD?
For pain intensity measurement in RMD, the NRS may be a simple measure to assess and standardize across RMD; however, more work on other pain (sub)domains is needed to better identify the construct multidimensionality.
The pain experience may (pathophysiologically) range from peripheral to central mechanisms; therefore, pain assessment must take this variability into account and address these individual patient differences.
Footnotes
AC is supported by a postdoctoral fellowship of the Amsterdam Movement Sciences research institute; he was supported by OMERACT and by a European League Against Rheumatism bursary to attend the OMERACT 2018 conference. UK is funded by a postdoctoral fellowship of the Medical Faculty, Technical University Dresden, and also funded by a federal joint committee of Germany. EC is supported in part by Arthritis Research UK and Health and Care Research Wales through the CREATE Centre. The Parker Institute, Bispebjerg and Frederiksberg Hospital is supported by a core grant from the Oak Foundation (OCAY-13-309). PGC is supported in part by the NIHR Leeds Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of the UK National Health Service, the NIHR, or the Department of Health. DCT is supported by the US National Institutes of Health (NIH) and the US Food and Drug Administration. EC has received research grants and/or served as member of advisory boards and speaker bureaus of AbbVie, Allergan, Amgen, AstraZeneca, Bio-Cancer, Biogen, BMS, Boehringer Ingelheim, Celgene, Chugai Pharma, Daiichi Sankyo, Eli Lilly, Ferring Pharmaceutical, GSK, Hospira, ISIS, Jazz Pharmaceuticals, Janssen, MedImmune, Merrimack Pharmaceutical, MSD, Napp, Novimmune, Novartis, ObsEva, Pfizer, Regeneron, Roche, R-Pharm, Sanofi, SynAct Pharma, Synovate, Tonix, and UCB. JAS has received consultant fees from Crealta/Horizon, Fidia, UBM LLC, Medscape, WebMD, the NIH, and the American College of Rheumatology. JAS is a member of the Veterans Affairs Rheumatology Field Advisory Committee. JAS is the editor and the Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis. JAS served as a member of the American College of Rheumatology’s (ACR) Annual Meeting Planning Committee and Quality of Care Committees, the Chair of the ACR Meet-the-Professor, Workshop and Study Group Subcommittee and the co-chair of the ACR Criteria and Response Criteria subcommittee. JAS is a member of the executive of OMERACT, an organization that develops outcome measures in rheumatology and receives arms-length funding from 36 companies. DCT is the editor-in-chief of The Clinical Journal of Pain and serves as an industry advisor or consultant to AcelRx, GSK/Novartis, and Pfizer.
- Accepted for publication March 8, 2019.








{kind=link}