

Abstract
Objective. We aimed to investigate demographic and clinical features and predictors of mortality in Korean patients with systemic sclerosis (SSc).
Methods. We performed a retrospective multicenter medical chart review in Korean patients diagnosed with SSc from 1986 to 2016 at 11 university hospitals representing each geographic area of Korea. SSc patients were defined according to the American College of Rheumatology preliminary classification criteria and subtyped as limited cutaneous (lcSSc) or diffuse cutaneous (dcSSc) SSc.
Results. We enrolled 751 patients (female, 86.7%; mean age at diagnosis, 48.9 yrs). The most common organ involvement was interstitial lung disease (52.7%), followed by gastroesophageal reflux disease (32.9%) and pulmonary arterial hypertension (13.6%). Patients with lcSSc were more common than those with dcSSc (64.8 vs 35.2%), whereas anti-Scl-70 and anticentromere antibody positivity were identified in 302 (42.5%) and 175 (25.5%) patients, respectively. In the 46 (6.1%) patients who developed a malignancy, lung cancer (23.9%) was the most common diagnosis, followed by gastric (13%) and breast cancer (13%). During the study period, 57 (7.6%) patients died, and the 5- and 10-year survival rates were 94% and 87%, respectively. Increased age at diagnosis, cardiovascular involvement, and anti-Scl-70 antibody positivity were significant predictors of death.
Conclusion. Clinical manifestations and survival rates in Korean SSc patients are similar to those of other populations. However, the prevalence of anti-Scl-70 antibody is higher in Korean SSc patients compared with whites, while the prevalence of anticentromere antibody is lower.
Systemic sclerosis (SSc) is a connective tissue disease of unknown etiology characterized by obliterative vasculopathy and fibrosis of the skin and internal organs, with a wide spectrum of clinical and laboratory manifestations1. Serious organ involvement, such as pulmonary arterial hypertension (PAH), can develop in patients with SSc, and clinical outcomes in SSc are extremely unpredictable because of its highly variable course. Thus, SSc has a poorer prognosis than other autoimmune diseases2. Cases of SSc are classified as limited cutaneous (lcSSc) or diffuse cutaneous (dcSSc) according to the extent of skin involvement and categorized by disease-specific autoantibodies including those directed against Scl-70 (topoisomerase I), centromere protein, and RNA polymerase III (ARA). Thus, the associations between clinicoserological characteristics, severity, and outcome in patients with SSc can give valuable insight into disease pathobiology.
Considerable ethnic and geographic variation in clinical and laboratory features, severity, and mortality have been observed in previous studies3,4,5, suggesting a link between genetic and environmental factors and the etiology of SSc. Thus, investigating the distinctive manifestations and outcome of SSc in different ethnic and geographic groups is important, not only for a better understanding of the characteristics of SSc but also to improve medical care in specific populations. However, previous assessments of the clinical characteristics in patients with SSc have focused on white populations or Western countries2,6,7,8,9,10 and few studies have been performed in Asian subjects, especially Koreans. To date, 2 studies have reported the clinical features of SSc in Korean patients in the Korean language11,12, while 1 study detailed disease-related mortality13. However, these were small-scale, single-center studies, and a nationwide study is needed to accurately identify the clinical features and mortality in Korean patients. The purpose of this study was to investigate demographic, clinical, and laboratory features of SSc in Korean patients and identify independent predictors of mortality in this population.
MATERIALS AND METHODS
Study design and population
We performed a retrospective multicenter cohort study in Korean patients diagnosed with SSc from 1986 to 2016 at 11 university hospitals representing each geographic area of Korea (Figure 1). Patient lists were compared to remove redundant cases. Patients were diagnosed according to the American College of Rheumatology (ACR) preliminary classification criteria for SSc14. Disease subtype (lcSSc and dcSSc) was categorized according to LeRoy, et al15. All study subjects were ethnically Korean. Patients with sine scleroderma or other autoimmune diseases such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), dermatomyositis, and polymyositis were excluded. The institutional review boards of each hospital approved the study protocol and waived patient informed consent because of the retrospective study design (IRB no. KNUH-2017-03-009 in Kangwon National University Hospital, CNUN-2017-082 in Chonnam National University Hospital, B-1801/447-402 in Seoul National University Bundang Hospital, HYUH 2017-05-023 in Hanyang University Hospital, CNUH 2017-03-023 in Chungnam National University Hospital, KC16OIMI0119 in Catholic Medical Center, 2017-06-018 in Soonchunhyang University Cheonan Hospital, 2017-03-003 in Chungbuk National University Hospital, CR315051-002 in Human Research Yonsei University Wonju Severance Christian Hospital, 1702-072-831 in Seoul National University Hospital, and 1704-013-054 in the Research and ERB of the Pusan National University Hospital).

Geographic distribution of 11 Korean hospitals in the present study.
Assessments
The 11 hospitals used the same predefined protocol to evaluate demographic, clinical, and laboratory features. We recorded the following for each patient: sex, SSc subtype, age at diagnosis, age at onset of Raynaud phenomenon (RP) and SSc, observation period, body mass index (BMI), residence (urban vs rural), modified Rodnan skin score (mRSS) at first visit, organ involvement, pulmonary function test (PFT) results, systolic pulmonary arterial pressure (PAP) on echocardiography; autoantibody status [including antinuclear antibody (ANA), anti-Scl-70 antibody, anticentromere antibody (ACA), and ARA], cancer, and death. Onset of scleroderma was defined as the first non-RP manifestation. The observation period was defined as the duration between diagnosis and the last followup. BMI was determined as weight in kg divided by the square of height in meters (kg/m2), and mRSS was measured by experienced rheumatologists at each hospital. Gastroesophageal reflux disease (GERD) was defined as the presence of symptoms such as heartburn, reflux, and dysphagia, and reflux esophagitis on gastroscopy, esophageal dysmotility on manometry, or esophageal dilatation on chest computed tomography (CT). Interstitial lung disease (ILD) was defined as the presence of bibasilar pulmonary fibrosis on chest radiography or high-resolution CT without evidence of another lung disease16. Cardiovascular involvement was defined as symptomatic congestive heart failure, pericarditis, or a major conduction disturbance17. PAH was defined as a systolic PAP > 40 mmHg on echocardiography or mean PAP > 25 mmHg on right-sided heart catheterization. PAH diagnosed without evidence of ILD was considered isolated PAH18. A renal crisis was defined as rapidly progressive renal insufficiency with malignant hypertension or microangiopathic hemolytic anemia19. PFT results included forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), FEV1-to-FVC ratio (FEV1/FVC), and DLCO. ANA was detected by indirect immunofluorescence on HEp-2 cells, and anti-Scl-70 antibody, ACA, and ARA were determined by Euroline SSc profile line immunoassay. We also recorded cancer occurrence, type, and death during the followup period. Experienced rheumatologists retrieved all data by medical chart review at each hospital.
Statistical analysis
Data were expressed as the mean ± SD or number (%), as appropriate. Group comparisons were performed for continuous variables using Student t test and for categorical variables using the chi-square test or Fisher’s exact test, as appropriate. The 5- and 10-year survival rates were calculated by Kaplan-Meier survival analyses, and comparisons of survival distributions were analyzed using the log-rank test. We first selected the significant prognostic factors by univariate analysis and then calculated independent predictors of mortality using a multivariate Cox proportional hazards model with backward selection. P values < 0.05 were considered statistically significant. All calculation was performed using SPSS Statistics for Windows, Version 23.0 (IBM Corp.) and Stata, Version 11.1 for Windows (StataCorp LLC).
RESULTS
We enrolled 751 Korean patients with SSc. The majority of patients (86.7%) were female, and the female-to-male ratio was 6:1 (Table 1). Two hundred sixty-four patients (35.2%) had dcSSc and 487 patients (64.8%) had lcSSc. The mean (± SD) age at diagnosis was 48.9 (± 13.3) years, and the mean ages of RP and scleroderma onset were 44.5 (± 14.6) and 46 (± 14.2) years, respectively. The peak age at diagnosis was in the 50s whereas peak onset ages of RP and scleroderma were in the 40s (Supplementary Figure 1, available with the online version of this article). The mean BMI and mRSS were 22.3 (± 13.3) kg/m2 and 8.4 (± 7.1), respectively, and 584 patients (77.8%) lived in an urban area. The most common organ involvement was ILD (52.7%) followed by GERD (32.9%), PAH (13.6%), cardiovascular involvement (11.2%), renal crisis (2.5%), and isolated PAH (1.7%). The mean FVC, DLCO, and systolic PAP were 78.4% (± 19.8), 65.5% (± 21.8), and 32.5 (± 16.6) mmHg, respectively. ANA, anti-Scl-70, ACA, and ARA were positive in 715 (96.6%), 302 (42.5%), 175 (25.5%), and 90 (15.8%) patients, respectively. Most patients had a single SSc-specific antibody, but 61 patients with SSc had > 1 SSc-related autoantibody; 29 of 671 (4.3%) with anti-Scl-70 and ACA, 26 of 565 (4.6%) with anti-Scl-70 and ARA, and 7 of 564 (1.2%) with ACA and ARA. One patient with SSc had triple SSc-specific autoantibodies. During the study period, death and cancer occurred in 57 (7.6%) and 46 (6.1%) patients, respectively. The most common malignancy was lung cancer (23.9%), followed by cancer of the stomach (13%), breast (13%), thyroid (10.9%), cervix (8.7%), and lymphoma (6.5%), and others (Supplementary Table 1, available with the online version of this article).
Clinical and laboratory characteristics of patients with systemic sclerosis (SSc) in Korea. Values are n (%) or mean ± SD.
Table 2 shows the comparisons of clinical features in patients with dcSSc and lcSSc. Patients with dcSSc were significantly younger at the time of the diagnosis than those with lcSSc (47.1 ± 13.3 vs 49.9 ± 13.2 yrs, p = 0.006). The dcSSc type was also associated with an earlier onset of RP (42.4 ± 14.5 vs 45.6 ± 14.6 yrs, p = 0.008) and scleroderma (44 ± 14.3 vs 47.2 ± 14.1 yrs, p = 0.006) than the lcSSc type. Patients with dcSSc had a higher mRSS (13.2 ± 7.2 vs 4.3 ± 3.6, p < 0.001) and lower FVC (72.9 ± 20% vs 81.8 ± 19%, p < 0.001), FEV1 (77.8 ± 20.1% vs 86.5 ± 20.7%, p < 0.001), and DLCO (62.1 ± 22.1% vs 67.7 ± 21.3%, p = 0.004) than patients with lcSSc. These were more frequently observed in patients with dcSSc than in those with lcSSc: GERD (42.4% vs 27.7%, p < 0.001), ILD (67.4 vs. 44.8%, p < 0.001), cardiovascular involvement (17% vs. 8%, p < 0.001), renal crisis (4.9% vs 1.2%, p = 0.002), and death (12.1% vs 5.1%, p = 0.001). The frequency of PAH, isolated PAH, and cancer were not significantly different between the 2 groups. As expected, the patients with dcSSc had a significantly higher frequency of anti-Scl-70 antibody and a significantly lower frequency of ACA compared with those with lcSSc. The frequency of ARA positivity was not significantly different between the 2 groups.
Comparison of clinical features between patients with dcSSc and lcSSc. Values are n (%) or mean ± SD.
We also compared disease presentations according to the presence of the anti-Scl-70 antibody (Supplementary Table 2, available with the online version of this article). Patients with the anti-Scl-70 antibody were diagnosed at a younger age (45.3 ± 13.9 vs 51.5 ± 12.2 yrs, p < 0.001) and had an earlier onset of RP (39.8 ± 15 vs 48 ± 13.6 years, p < 0.001) and scleroderma (41.5 ± 14.4 vs 49.2 ± 13.4 years, p < 0.001) than those without this finding. Further, anti-Scl-70-positive patients had a higher mRSS (10.2 ± 7.7 vs 6.6 ± 5.9, p < 0.001), frequency of dcSSc (50.3 vs 20.3%, p < 0.001), ILD (74.1 vs 38.9%, p < 0.001), and incidence of death (11.6 vs 4.7%, p < 0.001) than anti-Scl-70-negative patients; however, the frequency of isolated PAH was lower in anti-Scl-70-positive patients (0.3 vs 2.7%, p = 0.017). Additionally, patients with the anti-Scl-70 antibody had worse pulmonary function than those without this finding.
In our Kaplan-Meier analysis, the cumulative 5- and 10-year survival rates in all patients with SSc were 94% (95% CI 91.4–95.9%) and 87% (95% CI 82.9–90.3%), respectively (Figure 2). In the log-rank analysis, the presence of cardiovascular complications (p < 0.001) and anti-Scl-70 antibody (p = 0.003) were associated with poor survival (Supplementary Figure 2, available with the online version of this article). The Cox proportional hazards models for survival are described in Table 3. In univariate analyses, these factors were associated with decreased survival: age at diagnosis ≥ 50 years, male sex, residence in a rural area, ILD, cardiovascular involvement, PAH, renal crisis, cancer, FVC < 70%, DLCO < 60%, and anti-Scl-70 antibody positivity. The multivariate Cox proportional hazards model adjusting for confounding factors revealed these independent risk factors for death in our patients with SSc: increased age at diagnosis (HR 3.85, 95% CI 1.04–14.21; p = 0.043 for those 50–59 yrs and HR 9.95, 95% CI 2.35–42.25; p = 0.002 for those ≥ 60 yrs), cardiovascular involvement (HR 6.89, 95% CI 3.21–14.78; p < 0.001), and the presence of anti-Scl-70 antibody (HR 2.8, 95% CI 1.24–6.35; p = 0.014).
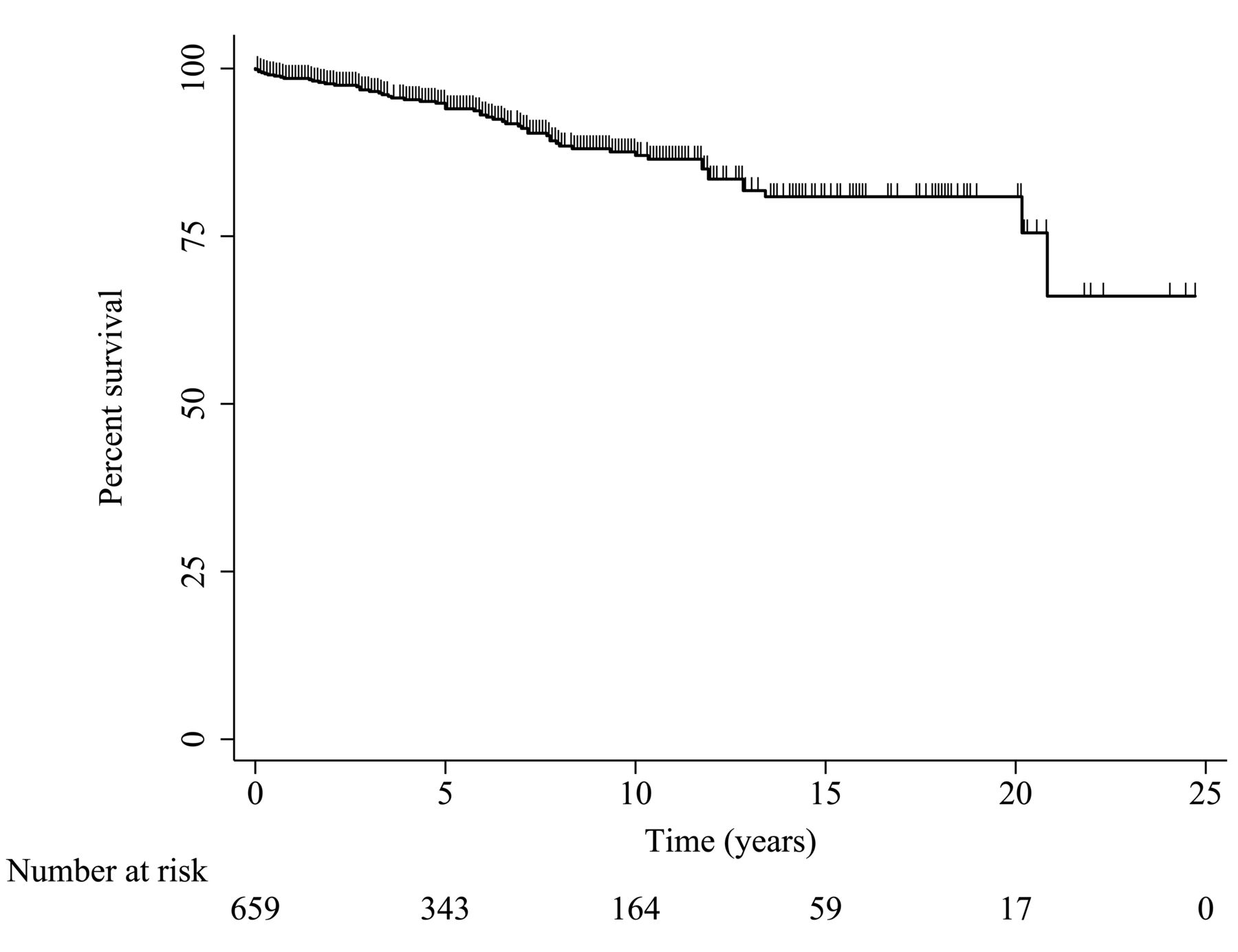
Overall survival curve of Korean patients with systemic sclerosis.
The univariate and multivariate Cox proportional hazards models for death of Korean patients with SSc.
DISCUSSION
We performed a retrospective, multicenter cohort study throughout Korea to evaluate the clinical and laboratory characteristics of patients with SSc and analyze the risk factors for mortality in this population. To our knowledge, this is the largest and most representative study of the clinical features and mortality in Korean patients with SSc to date.
Demographic, clinical, and laboratory characteristics in patients with SSc in other nations are summarized in Table 4. Similar to our results, most SSc patients were female, and the mean age of onset ranged from 42 to 47 years. The female-to-male ratio and the frequency of organ involvement including GERD, ILD, PAH, and renal crisis were largely similar in our Korean patients with SSc and those in other countries. Anti-Scl-70 and ACA tended to be associated with dcSSc and lcSSc, respectively, regardless of study origin. Notably, although the lcSSc-to-dcSSc ratio was comparable in different SSc populations worldwide, considerable geographic variation in the prevalence of SSc-associated autoantibodies was found between studies (Table 4). The frequency of the anti-Scl-70 antibody in patients with SSc in the United States, Japan, and most European countries except for France was < 30%, whereas the same prevalence in China and Korea was 59.9% and 42.5%, respectively. ACA positivity was found in nearly 40% of German, Spanish, Belgian, and Japanese patients with SSc. In contrast, the prevalence of this antibody was about 20% in studies of patients in Korea, France, the United States, and Brazil, and even lower in Chinese and Malaysian populations (13.1% and 9.7%, respectively). Thus, compared to patients with SSc in other nations, those in Korea demonstrated a distinctive distribution of SSc-specific autoantibodies and had a higher frequency of the anti-Scl-70 antibody. Ethnic variations in SSc-related autoantibodies have also been reported in previous studies; for example, African Americans with SSc had a higher rate of anti-Scl-70 antibody and lower frequency of ACA than white patients20,21. The evidence suggests that geographic and ethnic background may have a substantial effect on the occurrence of SSc-associated antibodies22,23, and further research is needed to clarify the clinical relevance of the disparities in SSc-related autoantibody profiles associated with geographic areas. In addition, our study revealed that 61 Korean patients with SSc had > 1 SSc-related autoantibody, a somewhat unexpected finding because coexistence of SSc-specific autoantibodies in the same patients is uncommon24,25. Whether this is a specific characteristic of Korean SSc warrants further investigation.
Comparison of clinical characteristics in patients with SSc in other populations worldwide. Values are n (%) or mean ± SD unless otherwise specified.
As with other autoimmune disorders such as RA and SLE, investigators have suggested that a close association exists between SSc and an increased risk of cancer26,27,28,29,30. Although the underlying pathophysiology has not yet been established, tissue fibrosis, autoantibodies, chronic inflammation, and the use of immunosuppressants may contribute to the development and progression of malignancy in patients with SSc28,31,32. In particular, patients with SSc are known to have a higher risk for lung cancer and hematologic malignancies than the general population26,27. However, a relationship between SSc and other malignancies such as breast, cervical, thyroid, and skin cancer has also been reported, although conflicting data exist27,28. In our study, 46 patients (6.1%) were diagnosed with a malignancy during the followup period, and the most common diagnosis was lung cancer (23.9%), followed by gastric (13%) and breast cancer (13%). Our findings were similar to those of 2 previously published Korean studies by Chang, et al and Kang, et al30,33. In Korea, the most common malignancy is reportedly thyroid cancer, followed by stomach and colon cancer. Because lung cancer is only the fourth most common cancer34, we hypothesize that patients with SSc in Korea may have a higher risk of this disease than the general population, similar to the risk found in other countries.
The overall survival rate in our Korean patients with SSc was 94% at 5 years and 87% at 10 years. The survival rate of patients with SSc has gradually improved over the last decades35. Steen and Medsger demonstrated that the 10-year survival rate had improved from 54% in the 1970s to 66% in the 1990s in their Pittsburgh cohort36. After 2000, the survival rate continued to rise. Hashimoto, et al analyzed 405 Japanese patients with SSc from 1973 to 2008 and found a 10-year survival rate of 88%37. Sampaio-Barros, et al reported 5- and 10-year survival rates of 90% and 84%, respectively, in their 10-year analysis of 947 Brazilian patients ending in 20109. The improved survival is thought to result from earlier diagnosis and referral to specialized centers and therapeutic advances such as angiotensin-converting enzyme inhibitors for the treatment of renal crisis3. The survival rate in our cohort was higher than that in the study by Kang, et al (5-yr survival rate, 88.5%), which used national health insurance data (Health Insurance Review and Assessment Services; HIRA) to evaluate Korean patients with SSc33. However, the diagnostic accuracy in that study is questionable because in the HIRA system, the primary diagnosis is entered for reimbursement purposes and can be provided by any medical doctor, including nonrheumatologists. Thus, their cases require validation by experts to achieve diagnostic certainty38,39. On the other hand, all the patients we enrolled were diagnosed by experienced rheumatologists in tertiary hospitals according to the ACR preliminary classification criteria. Thus, we suggest that the SSc mortality rates we found are more precise than those reported by Kang, et al33.
Our data revealed that increased age at diagnosis, cardiovascular involvement, and anti-Scl-70 antibody positivity were independent risk factors for mortality in Korean patients with SSc, consistent with the findings in previous reports13,40,41. As discussed, the prevalence of the anti-Scl-70 antibody varies according to geographic region and patient ethnicity. Thus, the significant association between the anti-Scl-70 antibody and a higher risk of death suggests the possibility of racial and geographic disparities in SSc-related mortality. Further studies are needed to evaluate this relationship. Additionally, Korean patients with SSc with cardiovascular involvement had about a 7-fold higher risk of death (HR = 6.89) than those without this complication. Thus, careful screening and appropriate management of cardiovascular disease in patients with SSc are crucial to improving clinical outcomes.
This study had several limitations. First, because of the retrospective study design, there might be errors related to data collection such as missing values or misclassifications. To avoid this problem, experienced rheumatologists retrieved and thoroughly reviewed the medical records in our present study. Second, because patients with SSc sine scleroderma were not included, our data may not fully reflect the entire spectrum of SSc. Last, we did not obtain data regarding the causes of death in patients with SSc. These can be classified as SSc-related death or as related to other causes, and cardiopulmonary involvement, infection, and cancer were reported to be the major causes of death in patients with SSc in previous studies9,37,40. Thus, further studies are needed to determine the causes of death in Korean patients with SSc.
Our study presents the clinical and laboratory characteristics of SSc in a large representative Korean cohort. ILD was the most common internal organ comorbid disease, and lung cancer was the most common malignancy in this population. The overall survival rate in Koreans with SSc was similar to that in other populations, but increased age at diagnosis, cardiovascular involvement, and anti-Scl-70 antibody positivity were all associated with a poor prognosis. Notably, the frequency of SSc-specific autoantibody positivity varies according to nationality, and Korean patients with SSc had a higher prevalence of anti-Scl-70 antibody positivity than other populations, suggesting the potential role of ethnic and geographic factors in autoantibody production and the clinical SSc phenotype.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
Supported by a research grant from Handok Inc. pharmaceutical company, Seoul, Korea, for the Digital Ulcer Cohort Study.
- Accepted for publication April 26, 2018.








{kind=link}
{kind=link}