

Abstract
Objective. Markers for treatment response in rheumatoid arthritis (RA) are lacking. The aim of the study was to assess the performance of the RA magnetic resonance imaging (MRI) scoring system (RAMRIS) in combination with serum biomarkers to predict response to methotrexate (MTX) treatment in therapy-naive patients with early RA by using high-field MRI.
Methods. Twenty-eight patients with RA were prospectively assessed with baseline 3-T MRI of the clinical dominant hand, 3 and 6 months after MTX. The patients met the 2010 American College of Rheumatology/European League Against Rheumatism (EULAR) criteria [average age 56.8 yrs (range 39–74); positive for rheumatoid factor and/or anticyclic citrullinated peptide antibodies; disease duration < 6 mos (range 2–23 weeks)]. RAMRIS and serum biomarkers consisting of various experimental proteins including receptor activator of nuclear factor-κB ligand (RANKL) were obtained. Remission or treatment response was defined according to EULAR. To adjust for intrapersonal correlation, generalized linear mixed models were used.
Results. Treatment response at 3 months was associated to low RAMRIS erosion subscores and low total RAMRIS scores (p = 0.019 and 0.03, respectively). Remission at 6 months was associated to low RANKL levels (p = 0.033). In multivariate analyses, response at 3 and 6 months was predicted more accurately with the inclusion of total RAMRIS score, RAMRIS synovitis subscore at the second metacarpophalangeal (MCP) joint, or a combination of the two (p value likelihood ratio test = 0.035, 0.035, and 0.041, respectively). Remission was more accurately predicted with inclusion of RANKL, with no significant predictive effect of MRI.
Conclusion. Baseline total RAMRIS can predict EULAR response. RAMRIS synovitis subscore at the second MCP joint and RANKL are associated with response and remission, respectively.
Reaching remission in rheumatoid arthritis (RA) unambiguously is the goal of any antirheumatic therapy1,2. Treatment guidelines and recommendations published by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) state that all patients diagnosed with RA should initially be treated with conventional synthetic disease-modifying antirheumatic drugs (csDMARD) from the point of diagnosis with the ultimate aim of achieving this goal3,4. By using modern treat-to-target strategies, remission or at least low disease activity can be reached in up to 82% of patients5,6.
Currently, the absence of rheumatoid factors (RF) and/or anticyclic citrullinated peptides antibodies (anti-CCP), the absence of bone erosions in conventional radiographs, the presence of low disease activity, and early intervention with csDMARD are considered good prognostic markers5. The sometimes poor performance of these markers might lead to under- or overtreatment of patients with early RA7. Owing to the more sensitive classification criteria introduced by EULAR/ACR in 2010, patients are now diagnosed and treated earlier in the course of the disease8. Moreover, the prognostic markers mentioned above are mostly based on randomized controlled trials including a homogeneous and preselected patient population, with generally higher prevalence of poor markers and high disease activity, so that generalizability to daily practice may be hampered. There is a lack of valid prognostic markers to help physicians to assess clinical response or remission at the onset of the disease in patients with early RA.
In clinical practice, radiographs are routinely used in most parts of the world, although their use in early RA is limited. Therefore, they are no longer part of the updated classification criteria for RA8. In contrast, magnetic resonance imaging (MRI) is a well-evaluated imaging technique and is used more frequently in daily practice and clinical trials for diagnosis and therapy control in patients with RA9,10,11. It was previously shown that MRI can depict typical pathological signs for RA such as inflammation (e.g., synovitis or tenovaginitis12) and bony changes early in the disease course, and with sensitivity13,14. These signs correlate to histological changes within the synovium15. In addition, MRI can reveal bone marrow edema (BME), which is known to be of high prognostic value in RA16. So far, the predictive role of MRI prior to initiation of csDMARD has not been systematically assessed, especially in a routine setting in patients with early RA.
Further, serological biomarkers play an increasingly important role in diagnosis, therapy control, and prognosis of early RA. Research focused especially on bone and cartilage in the last decade, with receptor activator of nuclear factor-κB ligand (RANKL) and osteoprotegerin (OPG) examined and evaluated even in RA17,18,19. However, no data for early arthritis and the prognostic value for reaching remission or at least clinical response have been published to date20.
In our study, we prospectively investigated the validity of the Outcome Measures in Rheumatology (OMERACT) RA-MRI scoring system (RAMRIS) and serological biomarkers as possible prognostic markers for remission or clinical response after 3 and 6 months of methotrexate (MTX) therapy in patients with therapy-naive, seropositive (RF and/or anti-CCP antibodies) early RA with severe disease activity [28-joint count Disease Activity Score (DAS28) baseline about 4.7; C-reactive protein (CRP) about 9.6 mg/l; Table 1]. The cohort was part of the German ArthroMark initiative, which aims to assess prognostic markers for RA [supported by the German Federal Ministry of Education and Research; ArthroMark (01EC1009)].
Patient characteristics at the beginning of the study.
MATERIALS AND METHODS
ArthroMark was a multicenter consortium [Berlin (Charité, Deutsches Rheumaforschungszentrum), Frankfurt, Munich, and Düsseldorf], while the Düsseldorf location was responsible for the MRI substudy for defining predictive MRI and serological biomarkers for patients with early RA. ArthroMark Düsseldorf was a prospective MRI study of patients with seropositive early RA before initiating a therapy with MTX.
Study design
This was a prospective cohort study (ArthroMark) using high-field MRI (3-Tesla) of the clinically dominant hand at beginning of the study (V0) before initiating MTX therapy in patients with early RA, after 3 months (V3), and after 6 months (V6). Prednisone was allowed at the description of the treating physician, up to 10 mg per day. The study was conducted in accordance with the principles of the Declaration of Helsinki and the International Conference on Harmonisation Guidance for Good Clinical Practice and approved by ethics committees at each site (Charite Berlin EA1/193/10 and local ethic committee of Heinrich-Heine-University Düsseldorf 3483).
Patient cohort
Twenty-eight patients with early seropositive RA were consecutively examined [age 56.8 yrs (range 39–74 yrs); positive for RF and/or anti-CCP antibody; disease duration < 6 mos (average 16.3 weeks, range 2–23 weeks)] fulfilling the 2010 ACR/EULAR criteria for RA8. Patient characteristics are listed in Table 1.
Clinical assessment
The following EULAR core set of variables was recorded: patient’s global assessment of overall disease activity, number of tender and swollen joints, erythrocyte sedimentation rate, and CRP (< 5 mg/l). The DAS28 was used to assess disease activity21. Remission was defined according to the EULAR remission criteria22, and clinical response according to Fransen, et al23.
Biomarker assessment
Blood serum samples were collected at every visit (0, 3, and 6 mos) on the same day as the clinical examination, and the MRI were performed and stored for posthoc analyses after the study. The following assays were carried out: human Dickkopf-1 (DKK-1; Quantikine ELISA, R&D Systems); OPG (Biomedica); free soluble RANKL high sensitivity (Biomedica); matrix metalloproteinase 3 (MMP-3; Quantikine ELISA, R&D Systems); human chitinase 3–like 1 (Quantikine ELISA, R&D Systems); neuropeptide-Y (NPY; ELISA, RAB0387 Sigma).
Magnetic resonance imaging
All MRI data were acquired on the same whole-body 3-Tesla MRI scanner (Magnetom Trio A Tim System; Siemens Healthcare). Images were made using a 4-channel flex coil. Before contrast media application, a coronal short-tau inversion recovery (STIR) and T1-weighted turbo spin echo sequence as well as a T1-weighted 3-D fast low angle shot sequence for T1 mapping using a dual flip-angle approach were acquired. Afterward, perfusion imaging was acquired with a dynamic 2-dimensional T1-weighted turbo flash sequence. Twenty seconds after the beginning of the sequence, the contrast agent Magnevist was injected with a dose of 0.4 ml/kg body weight.
Protocol for delayed gadolinium-enhanced MRI of cartilage (dGEMRIC)
After a 40-min delay, the dGEMRIC imaging sequence was applied, using a dual flip-angle approach for T1 estimation. The sequence variables were as follows: repetition time, 15 ms; echo time, 3.34 ms; flip angles, 5° and 26°; field of view, 90 mm × 53 mm; and slice thickness, 2 mm. The dGEMRIC analysis was performed by 1 radiologist with 6 years of experience in musculoskeletal imaging. The reader was blinded to RAMRIS analysis.
RAMRIS scoring
MRI scans were analyzed using RAMRIS23. According to OMERACT guidelines, RAMRIS was scored in consensus (1 radiologist with 6 years of experience in musculoskeletal imaging and 1 rheumatologist with 5 years of experience in musculoskeletal imaging). RAMRIS subscores including single joint scores were included posthoc. All scorings were performed by the same readers.
Ethical approval and consent to participate
Ethical approval for the study was received from the ethics committee of the Heinrich-Heine-University of Düsseldorf (reference no.: 3483) and the Charite Berlin (EA1/193/10). All patients provided written informed consent.
Statistical testing
The effect of biomarkers (DKK, OPG, RANKL, MMP, NPY) and MRI variables (RAMRIS and perfusion) on the outcomes EULAR response and remission at V6 have been studied in univariate analyses with the Mann-Whitney U statistical test and in multivariate analyses with logistic regression models adjusted for DAS28 at V0. Box plots are used to depict the distributions of markers in the outcome groups.
To adjust for intrapersonal correlation, we calculated generalized linear mixed models (GLMM) for the outcomes EULAR response at V6 or EULAR remission at V6. GLMM are set up with time as the independent variable and a random intercept for each study subject. Models incorporating the respective independent variables (biomarkers and MRI variables as above) were systematically assessed by likelihood ratio (LR) tests comparing with the null model (M0) that has time as the only independent variable. MRI scans (RAMRIS scoring) were blinded to the rheumatologist until the end of the study. All statistical tests are 2-sided, with a significance level of 0.05. P values are not adjusted for multiple testing.
RESULTS
To select potential markers for further assessment, univariate logistic regression analyses were performed in the ArthroMark cohort MRI substudy, to investigate the association between these markers and clinical remission or response (according to EULAR criteria) after 3 (V3) or 6 months (V6). The RAMRIS subscore for erosions (p = 0.019) and total RAMRIS (p = 0.03) score were significantly associated with response at V3 (Figure 1). No further significant results were found for the other imaging markers assessed for response prediction at either V3 or V6 (Supplementary Material, Table 1, available from the authors on request). Of note, BME was detectable in only 4 patients of our cohort. Hence, BME was not further considered in subsequent analyses.

Comparison of DAS28 responders versus nonresponders (according to EULAR) at 3 months (V3, left side) and 6 months (V6, right side) depicted by box plots. Erosion subscore (upper half) and total RAMRIS (lower half) were significantly different between groups at 3 months. At 6 months no significant differences were found. DAS28: 28-joint count Disease Activity Score; EULAR: European League Against Rheumatism; RAMRIS: rheumatoid arthritis magnetic resonance imaging scoring system.
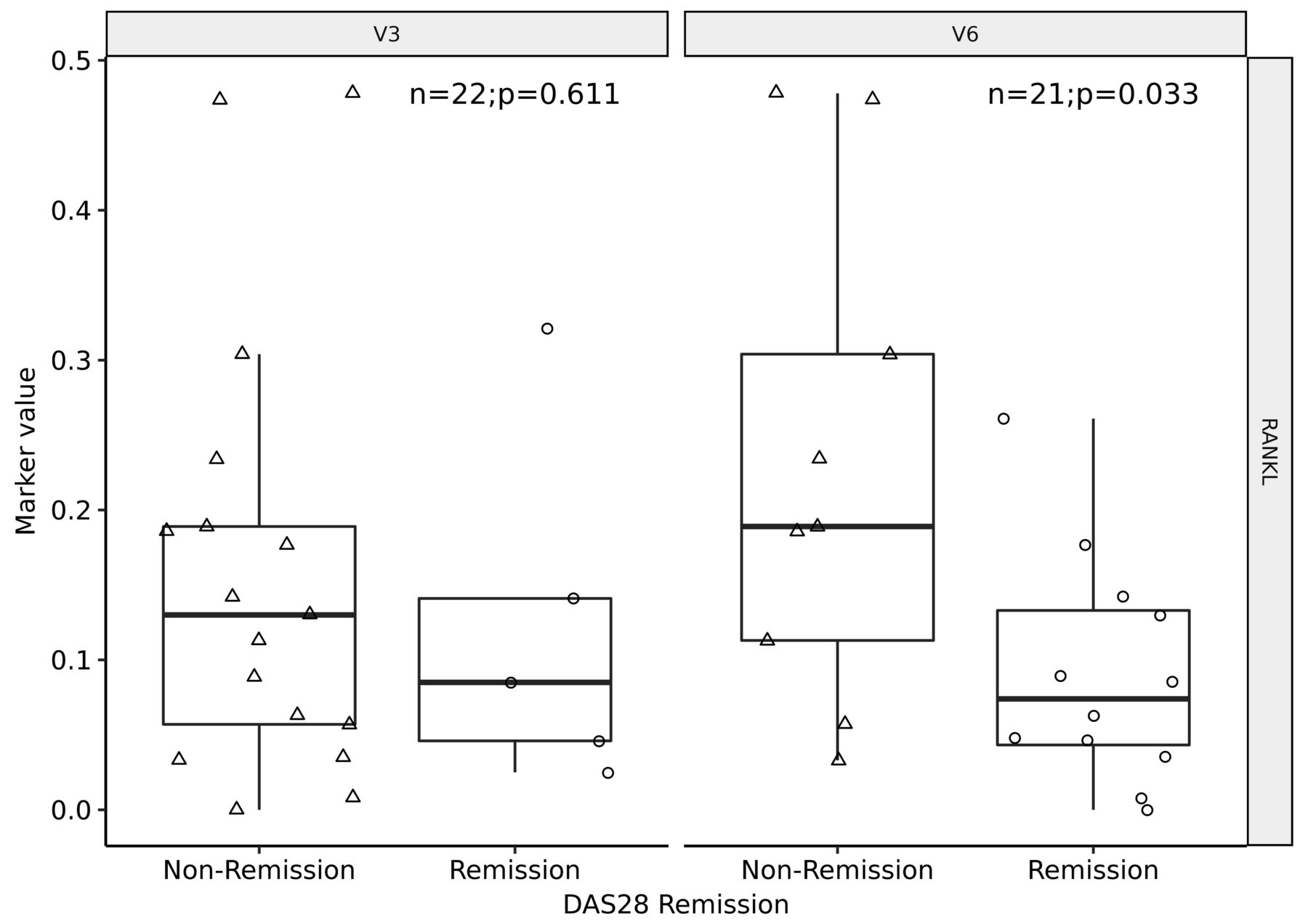
Concerning remission, low values of RANKL at baseline were significantly associated with EULAR remission at V6 (p = 0.033; Figure 2). Other markers including DKK1, OPG, MMP-3, NPY, RAMRIS and RAMRIS subscores (BME, erosions, and synovitis) did not show significant results at either V3 or V6 (Supplementary Material, Table 2, available from the authors on request).

Comparison of DAS28 responders versus nonresponders (according to EULAR) at 3 months (V3, left side) and 6 months (V6, right side) depicted by box plots. RANKL was significantly different between groups at 6 months. DAS28: 28-joint count Disease Activity Score; EULAR: European League Against Rheumatism; RANKL: receptor activator of nuclear factor-κB ligand.
Next, we performed multivariate analyses with the inclusion of candidate markers identified by univariate analyses, i.e., RAMRIS, RAMRIS erosion and synovitis subscore, and RANKL. Models incorporating the respective variables were systematically tested for EULAR response at V6 or EULAR remission at V6, respectively. As can be seen in Table 2, response was predicted more accurately with the inclusion of either RAMRIS (p value of LR test 0.035), RAMRIS synovitis subscore at the second MCP joint (p value of LR test 0.035), or a combination of the two (p value of LR test 0.041). Conventional potential predictors of response such as baseline DAS28 (Table 2), TJC, SJC, and CPR were assessed as well, but did not improve prediction (data not shown).
Specifying the marker models for the outcome response.
As can be seen in Table 3, remission was more accurately predicted when RANKL was considered, with increasing RANKL values worsening the chance of remission (p value of LR test 0.004). In contrast to response prediction, adding MRI markers (RAMRIS total or subscores) did not significantly improve model fit for remission.
Specifying the marker models for the outcome remission.
Finally, interreader reliability of MRI scoring at T0 was assessed to estimate the generalizability of scoring. Smallest detectable differences were as follows: RAMRIS total score 4.53, RAMRIS synovitis subscore for second MCP joint 3.53, and RAMRIS erosion subscore total 4.07.
DISCUSSION
Because treat-to-target strategies are increasingly implemented in the therapeutic algorithm and highly effective antiinflammatory therapies are available, low disease activity or even remission can be achieved in the majority of patients with RA5,24,25. Despite these improvements, there is a lack of valid data for prediction of therapy response or remission using clinical, serological, or radiographic variables before starting an antirheumatic therapy. ACR and EULAR recommend starting a csDMARD therapy immediately after the diagnosis of RA. Further, it is recommended that patients with a very high risk for rapid progression be treated initially with biologicals (for example, antitumor necrosis factor therapy)3. Accurate tools to select patients who likely profit from immediate biologic initiation rather than prior csDMARD therapy are needed. Indeed, ACR and EULAR stressed the importance of research to accomplish stratification and personalization of RA therapy in the future4.
MRI is used increasingly in clinical trials and in daily practice26. It was shown that MRI is able to sensitively depict even subclinical joint inflammation27. To date, there are no data for the prediction of clinical outcome for high-field MRI scans of the hand before initiating an antirheumatic therapy in therapy-naive patients with early RA. RAMRIS is a validated tool that was investigated and evaluated in many studies, but was not hitherto evaluated in response or remission prediction before initiating an antirheumatoid therapy in patients with early RA28.
In our study, high RAMRIS scores were highly associated with negative therapy response to MTX after 3 months, while low RAMRIS scores were associated with good or at least moderate therapy response (as assessed by DAS28 according to EULAR). This may indicate that RAMRIS is a potential predictive imaging marker for response. Similarly, high initial levels of the RAMRIS synovitis subscore of the second MCP joint showed association with a higher risk for poor response after 6 months, while there was no association between MRI value and remission overall. It could be demonstrated that there is sustaining inflammation in MRI despite clinical response or even remission as a sign of silent progression10,26. In support of this, we found that low RAMRIS or synovitis subscores of the second MCP joint were not associated with remission. Reasons for this lack of predictability may be the short therapy duration of only 6 months and the homogeneous treatment with “only” MTX. We cannot exclude that a longer followup of patients may have resulted in therapy response or remission even in those patients with a high baseline RAMRIS. However, current treatment guidelines recommend treat-to-target strategies and advise against tolerating active disease or low disease activity in biological-naive patients without contraindication1.
We found a surprisingly low amount of BME in our study. BME is known to be highly predictive for the development of erosive disease16. In accordance with this observation, there was only 1 patient with erosions on conventional radiographs of the hands at baseline within the current cohort. We maintain that the low burden of BME or erosive disease is a consequence of the short disease duration of only 16.3 weeks and subsequent immediate treatment. Of note, patients with BME did not appear to display higher scores in the other RAMRIS domains, potentially due to the low number of cases (n = 4).
Further and longer studies are needed to prove that RAMRIS is predictive for remission after a longer treatment period or an escalated treatment.
In contrast, baseline serum level of RANKL was significantly associated with remission in a longitudinal analysis. RANKL is known to correlate with cartilage and bony changes in degenerative or inflammatory joint diseases17 and is considered to contribute to bone destruction in RA29.
Our data suggest moreover that besides implemented clinical and serological markers for negative response, a high RAMRIS and a high synovitis subscore of the second MCP joint are highly predictive for poor therapy response in patients with early RA. The data also suggest that patients presenting high RAMRIS and/or synovitis subscores at a baseline MRI scan of the hand before initiating antiinflammatory therapy have a high risk of responding insufficiently to a csDMARD therapy, so that a primary biological therapy or at least a very tight therapy control could be of high value. The same applies for RANKL as a serum biomarker. Patients with high titers showed a high risk of not reaching remission after 6 months of continuous MTX therapy and may thus potentially be candidates for very tight control or immediate biological therapy.
To our knowledge, this is the first longitudinal study using GLMM showing the potential predictive value of the RAMRIS (in total and synovitis subscore of the second MCP joint) and RANKL, considering intrapersonal differences. There is a need to perform further studies to validate these findings and to define a clinically useful prediction model. Because of the number of patients, we were not able to define a cutoff value for response or remission (RAMRIS and RANKL), so that further studies are needed to gain sufficient data to justify clinical implementation.
At baseline, low RAMRIS scores were significantly associated with therapy response in our longitudinal analysis using GLMM. RAMRIS synovitis subscores at the second MCP joint and RANKL were significantly associated to response or remission, respectively. Our data suggest that MRI and biomarkers may aid response prediction and facilitate patient selection for intensified therapy in the future.
Acknowledgment
We thank Erika Rädisch for assistance in gathering the MRI scans.
Footnotes
Supported by a grant from the German Bundesministerium für Bildung und Forschung, ArthroMark (01EC1009).
- Accepted for publication January 16, 2018.








{kind=link}
{kind=link}