

Abstract
Objective. We investigated the development of giant cell arteritis (GCA) in patients with prior diagnoses of isolated polymyalgia rheumatica and/or peripheral arthritis (PMR/PA), and the potentially relevant characteristics of both illnesses in such patients.
Methods. We retrospectively compared the features of 67 patients at the onset of PMR/PA, and their outcomes, to those of a random group of 65 patients with PMR/PA who did not develop late GCA. We also compared the features and outcomes of patients with late GCA to those of a random sample of patients with more usual GCA (65 with concurrent PMR/PA and 65 without).
Results. Patients with late GCA represented 7.4% of all patients with GCA included in a large hospital-based inception cohort. PMR/PA preceded overt GCA by 27 months on average. Permanent visual loss developed in 10 patients, including 8 of 48 (17%) patients featuring cranial arteritis. A questionable female predominance was the only distinguishing feature of PMR/PA evolving into GCA; late GCA more often featured subclinical aortitis (OR 6.42, 95% CI 2.39–17.23; p < 0.001), headache (OR 0.44, 95% CI 0.19–1.03; p = 0.06), and fever (OR 0.29, 95% CI 0.13–0.64; p = 0.002) less often compared to the more usual form of GCA. Patients with either form of GCA experienced similar outcomes.
Conclusion. A cranial arteritis pattern of late GCA is associated with a significant risk for ischemic blindness. However, compared to the usual form of GCA, late GCA is often less typical, with a higher frequency of silent aortitis. Patients with relapsing/refractory PMR may not be at increased risk for late GCA.
Polymyalgia rheumatica (PMR) is a clinical syndrome of unknown etiology that develops after the age of 50 years and is characterized by pain and stiffness in the neck, shoulders, and pelvic girdle1. Giant cell arteritis (GCA) is a closely related condition2, in which vascular inflammation preferentially affects the medium and large arteries of the head and neck, aorta, and upper branches of the aorta. Both entities respond well to oral corticosteroids and often overlap in the same patient3. Of all patients with GCA, 45–60% experience symptoms of PMR either before, synchronously with, or after vasculitis onset4,5. Conversely, systematic temporal artery biopsies (TAB) have revealed subclinical GCA in 2–26% of patients with apparently isolated PMR3,4,6. Likewise, the reported incidence of GCA in the setting of established PMR varies from 0% to 47%, but is generally ≤ 15%3,7. Finally, 18-fluorodeoxyglucose (FDG)-positron emission tomography (PET) imaging studies have suggested that subclinical inflammation of the large arteries is frequent in patients with PMR, both at baseline and during relapses5,8,9.
The frequency of late GCA following PMR remains controversial; 2 studies have found an overall incidence of 7–10%6,10. In 1 prospective study, the incidence of GCA during the first year after PMR diagnosis was 5%11. Rodriguez-Valverde, et al found that polymyalgia patients < 70 years of age without features of temporal arteritis are at very low risk (< 2%) of eventually developing GCA12. Gonzalez-Gay, et al found that the prevalence of GCA evident in systematic TAB of a subset of patients with prominent systemic symptoms and high erythrocyte sedimentation rates (ESR) was only 9%13. Only 1 study has addressed the risk factors for late-onset GCA in patients with PMR11. These included the female sex, HLA DRB1*0101 or *0401, a high plasma viscosity, and an initial daily prednisolone dose > 15 mg. It remains unknown whether resistant or relapsing PMR is a risk factor for late GCA.
Regarding the features of GCA in treated or recovering PMR, 2 retrospective works on patients who developed GCA against a background of established pure PMR reported a high prevalence of ischemic complications14,15. However, 1 study included only patients with biopsy-proven GCA14, and the other had a small sample size15. Further, neither study included a control group in which GCA developed in the absence of prior PMR.
In our present study, we sought to define risk factors for late GCA development after pure PMR and the principal characteristics of the condition. We created a control group of patients with PMR who did not develop late GCA and 2 control groups of patients with GCA (with and without concurrent PMR).
MATERIALS AND METHODS
Patients and data collection
We analyzed the clinical, laboratory, and pathological features, and the treatments and outcomes of consecutive patients referred to the internal medicine departments of 2 tertiary care teaching hospitals for the treatment of GCA, in a setting of established PMR. As peripheral arthritis (PA) is frequently associated with PMR16 and may occasionally form part of the rheumatic spectrum of GCA17, we also included new GCA patients with such prior diagnoses, either isolated or overlapping with PMR symptoms. PMR was defined by ≥ 2 weeks of moderate to severe pain and morning stiffness lasting > 30 min in ≥ 2 areas (neck, shoulders, and pelvic girdles) without any evident alternative diagnosis. The inclusion criteria were a diagnosis of isolated PMR or PA prior to GCA, an arteritic relapse during or after a course of steroid treatment of PMR/PA, an interval ≥ 2 months between PMR/PA and GCA, and a GCA diagnosis based on the American College of Rheumatology (ACR) criteria18, with a rapid sustained response to corticosteroid treatment. Biopsy-negative cases were included if ≥ 3 of the ACR criteria were fulfilled. We also identified GCA in patients who fulfilled only 2 of the ACR criteria but whose FDG-PET scans were strongly suggestive of occult large-vessel vasculitis19. Noticeably, only 2 out of 32 such patients had isolated PMR with a negative TAB result. All GCA diagnoses were pathologically confirmed using the currently accepted criteria20,21.
All data on GCA stage were retrieved by searching the computerized patient record systems of either institution. Data were extracted and detailed information was collected using a standardized form. In addition, for patients who were recruited at Limoges Hospital, clinical, laboratory, and pathological data were prospectively recorded at the time of first admission using a specifically designed questionnaire to take a detailed history and log data on 176 items. These data were stored in computerized files and regularly updated22. This allowed us to retrieve 33 such patients (7.7% of the entire 1988–2017 inception cohort). Of the 67 patients with late GCA, 5 had received a GCA diagnosis at least 3 months before their first appointment at Limoges Hospital. All the other patients were diagnosed with late GCA in our departments. A comprehensive review of all new patients with GCA seen at Caen University Hospital from 1998 through 2017 retrieved 29 (7.1%) late GCA cases.
Study variables and clinical definitions
Details on rheumatological features, the levels of acute-phase reactants at disease onset, systematic TAB performance, starting prednisone dose, number of relapses during prednisone tapering, lowest prednisone dose associated with permanent disease control, use of steroid-sparing agents, and total duration of treatment were retrieved for each patient. If PMR/PA had been diagnosed elsewhere, both the rheumatologist involved in patient care and the family physician were contacted by mail and asked to provide relevant data. PMR relapses were defined using a combination of patient self-assessment, ESR, C-reactive protein (CRP) level, shoulder pain/limitations on clinical examination, and response to steroid dose adjustments23. Relapsing patients who were unable to reduce their prednisone doses < 20 mg/day at 6 months, 10 mg/day at 12 months, or 7.5 mg/day at 2 years were considered resistant cases.
Retrieved for each patient were demographics, date of GCA diagnosis, clinical features, principal laboratory variables, ACR criteria, and TAB results. Clinical items extracted from chart or computerized files included persistently active PMR or PA, new-onset headache, scalp tenderness, jaw claudication and/or other jaw/mouth/throat problems (e.g., reduction or difficulties in jaw opening, maxillary or tooth pain, lingual discomfort, ischemia, sore throat, carotidynia, dysphagia, hoarseness, and/or dry cough), and visual ischemic manifestations. Only visual events that developed before therapy or within the first 2 weeks after therapy commenced were included in analyses. Ischemic visual symptoms included transient symptoms and permanent visual loss22. Amaurosis fugax, intermittent blurred vision, and transient diplopia were considered transient ischemic visual symptoms. Permanent visual loss included anterior ischemic optic neuropathy, central retinal artery occlusion, and posterior ischemic optic neuropathy. The temporal arteries were considered abnormal on examination if pulses were decreased or absent and/or if nodules, redness, thickening, or tenderness was apparent in ≥ 1 artery. Constitutional syndrome was defined as a temperature ≥ 38°C lasting for ≥ 1 week, severe asthenia, and/or weight loss > 5%. Jaw claudication was considered present if the patient reported recurring pain on chewing that resolved when chewing stopped, or trismus. Upper limb artery involvement was defined on a clinical basis followed by echo Doppler and/or angiographic confirmation. Cranial arteritis was defined by at least a headache of recent onset, irrespective of other presenting features, whereas typical cranial arteritis included ≥ 3 of the following features: new-onset headache of moderate to severe intensity, jaw claudication or trismus, other jaw/mouth/throat problems, scalp tenderness, and an abnormal temporal artery on physical examination. Subclinical aortitis was diagnosed using (since 2005) FDG-PET scan study, computed tomography (CT) scan study, or both. A vascular territory was considered affected on aortic CT angiography when showing a circumferential and homogeneous thickening ≥ 2 mm of the vascular wall. On FDG-PET/CT, all vascular uptakes of equal or superior intensity to that of liver physiologic uptake were considered positive. Circumferential and homogeneous vascular uptakes were suggestive of vasculitis24. Patients with isolated subclinical aortitis qualified for late-onset GCA if they also had otherwise unexplained elevated acute-phase reactants that normalized upon steroid treatment readjustment. Relapse was defined as recurrence of clinical symptoms and/or inflammatory variables, attributable to GCA, which required increased medication. Such events that occurred after cessation of planned treatment were also considered recurrences.
Comparisons among groups
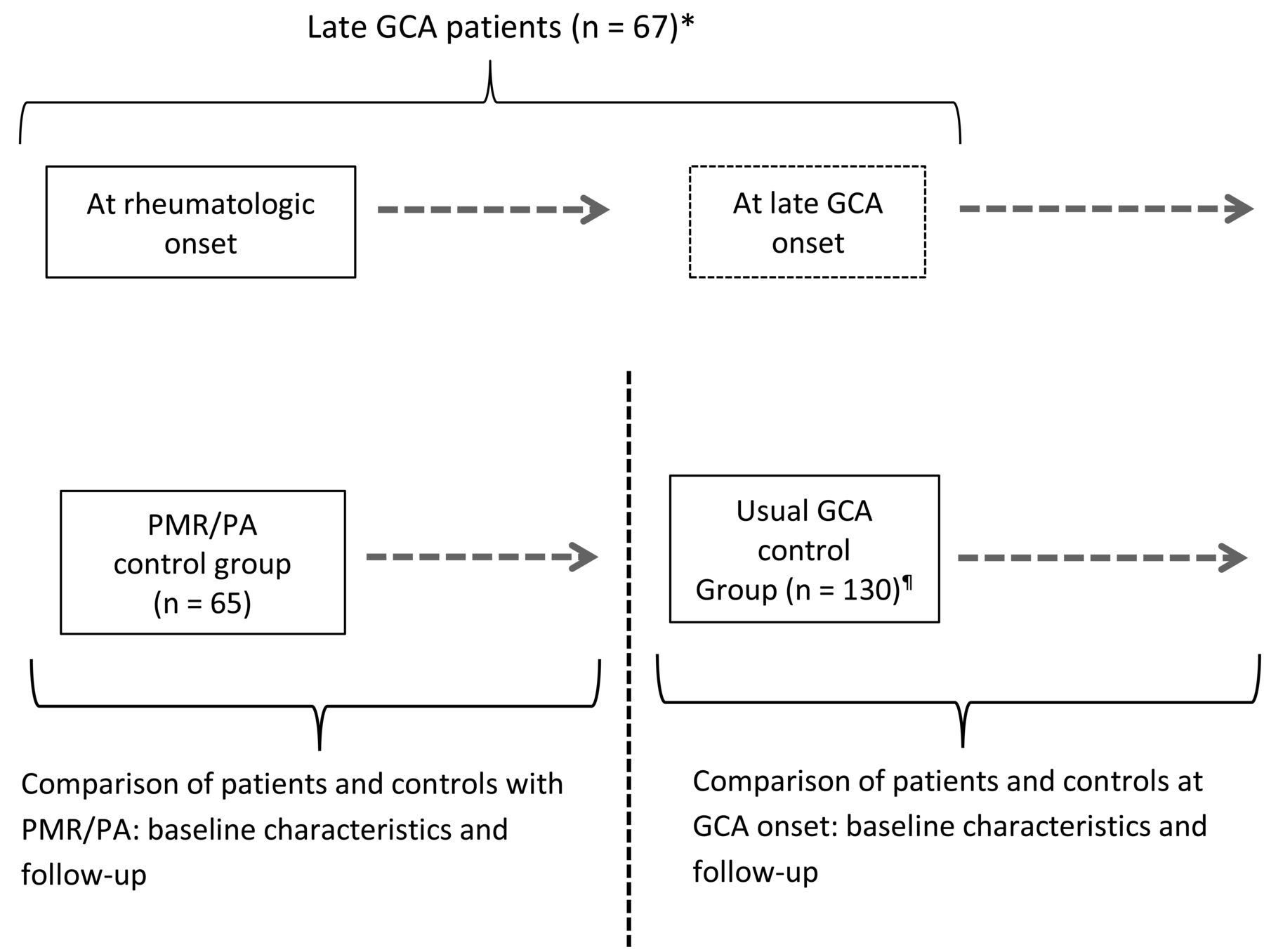
Each PMR/PA patient with late GCA was matched to members of 3 randomly created control groups (Figure 1). A PMR/PA-alone group was created from a retrospective cohort of 91 PMR/PA patients without late GCA diagnosed between 2001 and 2017 and followed up in the Internal Medicine Department of Limoges Hospital. Two control groups with the usual form of GCA were similarly extracted from the Limoges inception cohort and were composed of 65 patients with and 65 without concurrent PMR/PA. Baseline characteristics, treatments, and outcomes were compared between patients with late GCA and the controls.

Study design. *The Limoges recruitment consisted of 33 patients extracted from a GCA inception cohort (1988–2017) and 5 additional patients with late GCA (developing after PMR) referred for second advice. The Caen University Hospital recruitment consisted of 29 patients extracted from a similar inception cohort (1999–2017). †Includes 65 patients with isolated GCA and 65 with synchronous GCA and PMR/PA. Dashed arrows indicate followup times and outcomes. GCA: giant cell arteritis; PMR: polymyalgia rheumatica; PA: peripheral arthritis.
Treatments and outcomes
No preestablished glucocorticoid protocols were used to treat PMR/PA. At both centers, methotrexate (MTX) was the first steroid-sparing treatment option for patients with resistant PMR. Most patients with GCA were treated using standardized protocols. Patients lacking ischemic manifestations received prednisone at 0.6–0.8 mg/kg/day until symptoms disappeared and the CRP level had fallen to < 5 mg/l. The prednisone dose was progressively tapered to 0.35 mg/kg within 4–6 weeks. Patients with permanent ischemic manifestations received initial prednisone at 0.9–1 mg/kg/day, often preceded by pulse methylprednisolone, which was then similarly tapered. Minor relapses were managed by temporarily increasing prednisone to the previously effective dose, whereas severe relapses involved more consistent increases, on an individualized basis. Patients with relapsing/resistant disease or who experienced serious steroid-related side effects often received steroid-sparing drugs, such as MTX, disulone25, cyclophosphamide (CYC)26, or tocilizumab, according to protocols specific to either center.
Statistical analyses
PMR/PA and GCA controls were selected using a random-number method. Continuous variables are expressed as means ± SD and categorical variables as frequencies with percentages. The normalities of the distributions of quantitative variables were checked using the Shapiro-Wilk method. Comparisons of continuous variables were performed with the aid of Student t test. Proportions were compared using chi-square or Fisher exact tests. To identify the specific characteristics of late GCA, multivariate analyses were performed by multiple logistic regressions. We compared GCA patients with and without prior diagnoses of PMR/GCA. To reduce residual confounding, we built crude and age/sex-adjusted models of potentially specific features of late GCA including variables with p values < 0.25. The significance threshold selected for the final model was 0.05. All calculations were performed using the statistical package SAS, version 9.1.3 (SAS Institute).
Ethics board approval
The data concerning all patients with late GCA were retrospectively collected. This study was conducted in compliance with the Good Clinical Practices and Declaration of Helsinki principles. In accordance with French law, a formal approval from an ethics committee is not required for this kind of retrospective study.
RESULTS
Patient characteristics at the onset of PMR/PA and rheumatological outcomes prior to GCA
Of the 67 included patients, 55 had PMR, 5 had PA, and 7 had PMR/PA. The mean patient age was 72.1 ± 8 (range 51–86) years and the female/male ratio was 3:1. Only 6 patients received < 15 mg/day of steroid initially. Of 66 assessable patients, 29 (44%) relapsed at least once and 22 (33%) had chronic/resistant disease, causing rheumatologists to prescribe steroid-sparing treatments for 14 (21%). At the time of GCA diagnosis, 21 patients (31%) had completed their PMR treatment 1–102 months prior (mean 23 mos), after a mean steroid course of 15 months (range 2–49), whereas the other patients were still taking prednisone and continued to do so for a mean of 24 months (range 2–115). The entire cohort of 132 PMR/PA patients (67 late GCA patients and 65 controls) was followed up for 38.5 months on average (range 3–132 mos). Of 5 patients who developed seronegative rheumatoid arthritis or ankylosing spondyloarthritis, 4 had resistant PMR prior to their final diagnoses and 1 was in the late GCA group.
Table 1 shows the results of univariate analyses comparing patients with PMR/PA and controls for diagnosis and late outcomes. At disease onset, patients with late GCA and controls were indistinguishable, except for a higher proportion of females (p < 0.0001) in the former group. The groups were similar in terms of baseline ESR and CRP levels, and proportions of patients experiencing long-lasting remission, relapses, and resistant PMR/PA.
Univariate analyses of patients and controls at the time of PMR (or PA) onset involving age, sex, baseline ESR and CRP levels, and response to treatment. Values are n (%) or mean ± SD unless otherwise specified.
Patient characteristics at GCA onset and responses to treatment
GCA was diagnosed at an average of 27 months after PMR/PA diagnosis (median 17 mos, range 3–125 mos; Figure 2). Of the 20 patients with negative TAB (18 cases) or no TAB (2 cases), 12 had large vessel vasculitis evident in PET or CT scans. Of the 10 patients with previously negative TAB, 8 had positive contralateral TAB data at the time of GCA diagnosis. Of the 46 patients (69%) who were still taking prednisone at this time (mean daily dose 8.7 ± 4.7 mg), 26 (57%) had persistent or recurring concurrent rheumatic disease. Apart from the PMR/PA symptoms, 2 principal clinical patterns were evident at GCA onset. Cranial arteritis was the sole or prominent clinical feature in 48 patients (72%) and was typical in 33 (≥ 3/5 typical cranial symptoms or signs). Of these 48 patients, 8 (17%) developed permanent visual loss (bilateral in 3). Twelve patients exhibited transient, visual ischemic symptoms, heralding the development of permanent vision defects in 4. Thus, 18 patients (27%) developed visual ischemic symptoms and all but 1 exhibited other features of cranial arteritis. Four other patients had extraophthalmic permanent ischemic manifestations. Sixteen patients (24%) had prominent systemic disease mainly diagnosed by FDG-PET; of these 16, only 1 (6%) experienced visual damage. Table 2 summarizes the principal characteristics of the 10 patients with permanent vision loss.

Delay of onset of late GCA in 67 patients with PMR/PA. GCA: giant cell arteritis; PMR: polymyalgia rheumatica; PA: peripheral arthritis.
Principal features of 10 patients with late GCA who presented with permanent visual loss.
Of 58 assessable patients, 19 (33%) underwent PET scanning, which revealed subclinical aortitis in 17. Twelve other patients underwent CT scanning, which revealed a thickened aortal wall in 3 patients. One of 20 patients (5%) with aortitis (i.e., positive FDG and/or CT plus elevated acute-phase reactants) developed permanent vision loss.
After a mean of 61 months (range 2–193) of followup, 38 patients (58%) had experienced relapses or recurrences. Seventeen (26%) had multiple relapses or had developed resistant disease and had been continuously treated for 63 ± 38.6 months. Seventeen (25%) had received steroid-sparing treatments including disulone, MTX, CYC, and/or biologics; 30 (45%) were in long-lasting remission after treatment courses of 32.4 ± 25 months; and 8 (12%) had died. Of the 20 patients diagnosed with subclinical aortitis (defined by positive PET or CT angiography and high ESR/CRP), 8 (40%) had multiple relapses or developed resistant disease, 9 (45%) received steroid-sparing drugs, and 6 (30%) were in long-lasting remission.
Table 3 shows the results of univariate analyses comparing the demographics, disease characteristics, and outcomes of patients in the 2 groups. Logistic regression showed that patients with late GCA had more subclinical aortitis than the GCA controls, and fewer headaches and fevers (Table 4). Neither the chosen therapeutics nor outcomes differed between the 2 groups.
Univariate analyses of 67 patients with late GCA to 130 with usual GCA (i.e., without a prior diagnosis of PMR/PA) involving baseline GCA features, treatments, and outcomes. Values are n (%) or mean ± SD unless otherwise specified.
Baseline late GCA characteristics independently associated with a prior diagnosis of PMR or PA as revealed by backward stepwise logistic regression.
DISCUSSION
Our results confirm that late GCA in a setting of established PMR (or PA) is not rare. Although the study design did not allow us to calculate the incidence of late GCA after PMR/PA, we observed such events in 7.4% of a large, tertiary care–based inception cohort of patients with GCA. Because studies on PMR outcomes have shown comparable rates (7–10% late GCA)6,11, we suggest that the true incidence of late GCA in patients with pure PMR is similar.
We recorded GCA in 5 patients with PA lacking concurrent PMR, unlike what was found in a previous study18. Differences in study design, recruitment bias, and GCA sample sizes may explain this discrepancy, although it is also possible that GCA developing after PMR and/or PA may represent a variant of the usual form of GCA, with specific disease associations. Patients of our present study who had isolated PA experienced remission after steroid treatment, with no late joint damage.
The time that elapsed between PMR diagnosis and the first arteritic relapse ranged from < 3 months to 10 years (median 17 mos). In 2 prior studies, the duration of pure PMR prior to GCA development was shorter (median 7–8 mos); the longest interval was 5 years15,16. We have no satisfactory explanation for these differences, although variations in GCA diagnoses between internists and rheumatologists may be in play. PMR can recur years after discontinuation of steroid therapy27 or may be a late feature of established GCA, but late GCA recurrences are rather uncommon27. It may thus be relevant that 16% of our patients developed GCA ≥ 4 years after PMR/PA. In such patients, the persistence of subclinical GCA throughout the PMR course is rather unlikely, although repeat TAB occasionally reveals active GCA several years after treatment has been completed28. Conversely, GCA developing early in the course of PMR is likely to have been subclinically present since the time of PMR onset, progressing to overt disease during steroid tapering3.
At baseline, PMR/PA patients with developing GCA were indistinguishable from those without GCA, except for a strong female predominance. Although the control PMR group was biased toward males (62%), likely reflecting recruitment bias, our finding is in line with that of Mackie, et al10. However, our findings may not be entirely applicable to PMR populations recruited in rheumatology clinics or followed up by general practitioners.
Late GCA developing after PMR/PA followed 2 major patterns. Cranial arteritis was the most frequent feature, present in most patients who were still taking steroids (63%), even at ≥ 10 mg/day. However, a pattern highly suggestive of temporal arteritis was encountered in two-thirds of patients with cephalic features, whereas about 30% of all patients denied headaches and 24% presented with prominent systemic symptoms or unexplained increases in the levels of acute-phase reactants. These findings are remarkably similar to those of Hernandez-Rodriguez, et al14. Together, these findings indicate that diagnosis of a first arteritic relapse in a patient with established PMR or PA may be challenging, emphasizing that vigilance is required throughout the disease course and beyond.
The frequencies of permanent visual ischemic complications in patients with late GCA were similar in our study and that of Hernandez-Rodriguez, et al14, at 17% and 16%, respectively. Although permanent visual loss developed in only 11% of the patients described by Narvaez, et al15, the frequency of severe vascular events, including stroke and upper limb claudication, was 28%. Hence, GCA is a potentially serious complication of established PMR. Moreover, we observed that patients with overt cranial arteritis were at an even higher risk (≤ 24%) for developing permanent vision loss. This finding is in agreement with those of previous studies on the visual ischemic risk associated with GCA22,29,30. Accordingly, our study and that of Hernandez-Rodriguez, et al14 confirm that patients with late GCA who present with prominent systemic manifestations and/or large artery vasculitis are at low risk for developing permanent visual loss. This is consistent with previous studies of GCA31,32.
We found that late GCA was less clinically typical than early GCA, with fewer cranial symptoms and fevers. This may be attributable to attenuation of the GCA course during or after glucocorticoid treatment of PMR. Conversely, the much higher frequency of aortitis in such patients compared to early GCA controls (30% vs 5%) may indicate pathophysiological and/or clinical overlap between PMR and large-vessel vasculitis5,33,34. Although the proportions of patients with late and early GCA who underwent PET scans during the 2005–2017 study period were slightly unbalanced (33% vs 21%), this can hardly explain such a major difference in the proportions of aortic involvement. Moreover, we avoided inclusion biases by excluding from our study patients with isolated active PMR and subclinical aortitis. Nevertheless, PET and/or CT angiography were only performed in cases of clinical suspicion in patients with PMR. Therefore, the outcome may have been biased, overstating the importance of an association between aortitis and late GCA. Other limitations of our study include the retrospective design, which may have introduced referral bias. We lacked detailed data on the PMR/PA features at GCA onset in a substantial proportion of patients. The sample size was relatively small, which may have hidden potentially relevant variables. In addition, sampling bias was likely in the PMR/PA control group. Conversely, most included patients were part of well-defined inception cohorts, increasing the accuracy of data collection. The main strength of our study is that we compared patients to randomly selected PMR and GCA controls, allowing us to reveal possible sex differences in terms of late GCA risk and to identify variation in the clinical pattern of late GCA.
All patients with PMR should undergo careful routine scrutiny for underlying GCA both at baseline and thereafter, particularly during the first 2 years of PMR; all should be informed about such possible signs of GCA at the time of PMR diagnosis. Patients who develop signs of even mild cranial arteritis should be urgently evaluated for GCA and aggressively treated without delay. Conversely, patients with persistently unexplained high levels of acute-phase reactants should be carefully evaluated for subclinical aortitis. Patients with isolated relapsing/refractory PMR may not be prone to hidden GCA, but this requires confirmation using a prospective study of a large population of unselected patients with PMR.
- Accepted for publication December 7, 2017.








{kind=link}
{kind=link}