

To the Editor:
Polymyositis (PM) and dermatomyositis (DM) are chronic autoimmune diseases characterized by skeletal muscle inflammation in which interstitial lung disease (ILD) is found in up to 78% of cases1. Clinically amyopathic DM, a subset of DM without objective muscle weakness, and positivity for antimelanoma differentiation-associated gene 5 autoantibodies (anti-MDA5) are known risk factors for rapidly progressive ILD (RPILD)2,3,4. We present a patient with DM, anti-MDA5 antibodies, and RPILD who successfully underwent a bilateral lung transplantation. This report was approved by the Regional Ethical Committee of Stockholm (2005/792-31/4 and 2011/1374-32).
A 38-year-old white man presented with a 4-month history of uncharacteristic skin rash, mild muscle weakness, arthralgia, and exertional dyspnea. His physical examination revealed heliotrope rash, Gottron papules, periungual erythema, mechanic’s hands, small buccal mucosa erosions, fingertip ulcers, and muscle weakness. Cardiopulmonary auscultation was unremarkable. His complete blood count and muscle enzymes were normal. Erythrocyte sedimentation rate was > 90 mm/h, and C-reactive protein was 37 mg/l. He was positive for anti-Ro52 by Immunoblot, but the following were negative: anti-Mi2, anti-SRP, anti-Jo1, anti-PL7, anti-PL12, anti-dsDNA, anti-Sm, anti-Scl-70, anti-Scl-100, anti-SS/B, anti-RNP, rheumatoid factor, antinuclear antibody, and antineutrophil cytoplasmic antibodies. Muscle histopathology showed fiber size variation. A chest computer tomography (CT) showed unspecific basal reticular infiltrates. The patient was started on prednisone 1 mg/kg/day and colchicine.
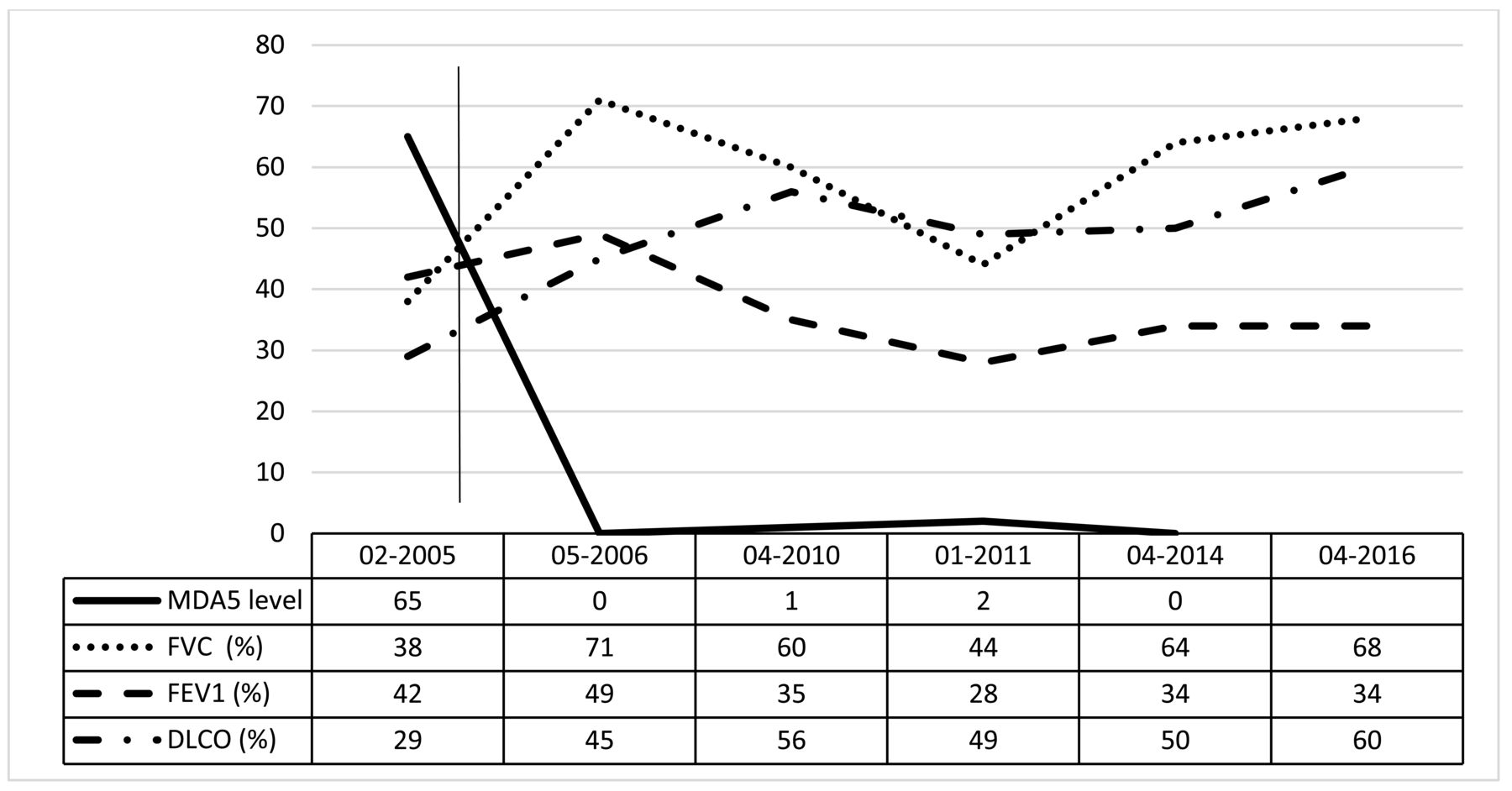
Three weeks later, his pulmonary status worsened and severe bilateral pulmonary interstitial infiltrates with ground-glass opacifications appeared on high-resolution CT (HRCT). Pulmonary function test results are shown in Figure 1. Bronchoscopy, transbronchial biopsy, and bronchoalveolar lavage fluid were normal including negative microbiological cultures. Electromyography and muscle magnetic resonance imaging (Figure 2) suggested an inflammatory process. A repeated muscle biopsy showed MHC class I expression in perifascicular fibers. Based on these findings, a diagnosis of DM with RPILD was made and treatment was initiated with intravenous (IV) methylprednisolone pulses combined with a single IV cyclophosphamide (CYC) pulse, followed by oral administration (2 mg/kg/day). Given the lack of clinical improvement, the patient was referred for lung transplantation.

Evolution of pulmonary function and serum levels of anti-MDA5 before and after lung transplantation. Longitudinal anti-MDA5 titers were assessed by a line blot assay (Euroline myositis panel 4 by Euroimmun A.G.) that detects human immunoglobulin G with a cutoff of ≤ 10, meaning that values of 11 and higher are considered positive. MDA5: melanoma differentiation-associated gene 5; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s.
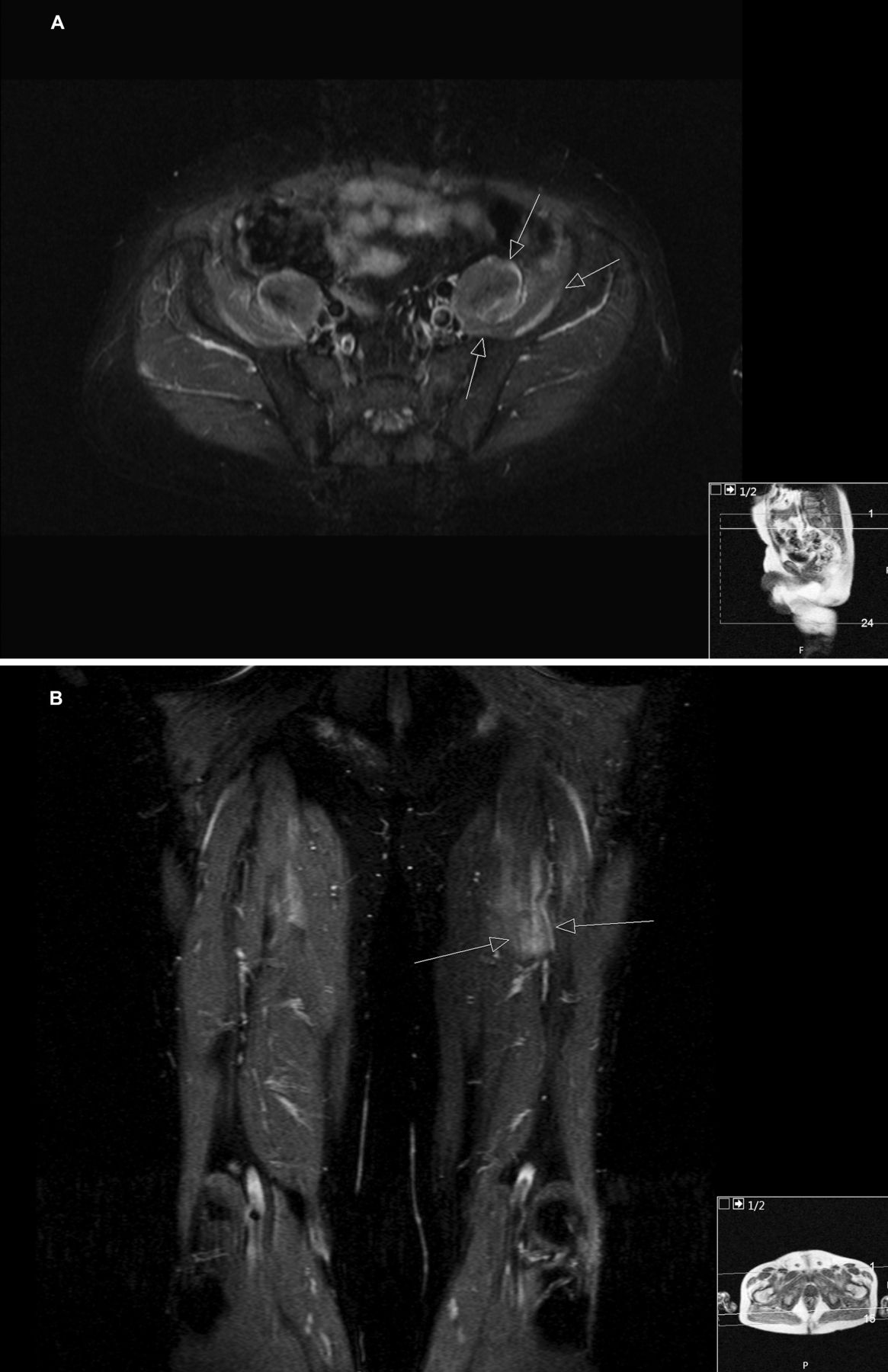
Magnetic resonance imaging of pelvis (A) and dorsal thigh (B). (A) Axial slice of the pelvis showing muscle edema in the left psoas muscle and left iliac muscle (arrows) using a short-tau inversion recovery (STIR) sequence. (B) Coronal slice of the dorsal thigh showing muscle edema (arrows) in the left major adductor muscle using a STIR sequence. Of note, similar but less intensive muscle edema can be seen in the same muscles contralateral. Intramuscular edema of proximal muscle groups is a frequent finding in polymyositis/dermatomyositis, irrespective of autoantibody status.
One week later, his pulmonary status deteriorated. Broad spectrum antibiotics, IV methylprednisolone, and IV immunoglobulin (Ig) were added. Repeated chest HRCT showed extensive lung consolidation, a small pneumomediastinum, and a pericardial effusion. This sudden deterioration prompted approval for lung transplantation. After prolonged venovenous extracorporeal membrane oxygenation (ECMO), a bilateral lung transplantation was performed5. Endstage interstitial lung fibrosis, without signs of granulomas, vasculitis, or malignancy, was shown on histopathologic examination. After a 4-month hospitalization, the patient transferred to a rehabilitation unit before returning home. When assays for anti-MDA5 became available, his serum was screened6. High titers of anti-MDA5 were found pretransplantation, with subsequent disappearance of the autoantibody (Figure 1). Twelve years later, he remains in remission without signs of rejection, taking low-dose prednisolone, azathioprine 100 mg/day, and tacrolimus 2.5 mg/day. He resumed his previous work part-time, and exercises several times per week.
The severity of ILD associated with PM/DM varies from asymptomatic to devastating, and when muscle involvement is absent or subtle, diagnosis is often delayed. The anti-MDA5 subset is characterized by RPILD, cutaneous ulcers, and poor survival3,4. These patients are frequently resistant to conventional immunosuppressive therapies including high doses of glucocorticoids combined with CYC, cyclosporine, or IVIG. Lung transplantation thus represents a rescue therapy, and in a large retrospective study on connective tissue–associated ILD (CTD-ILD), this approach showed similar survival to idiopathic pulmonary fibrosis and a low rate of CTD flare posttransplantation7. Their PM/DM subgroup (n = 34) had a 1-year survival of 67.5% and a 3-year survival of 46.7%, but clinical phenotypes and antibody status were not specified. A successful lung transplantation in an anti-MDA5 subject with a short followup period posttransplantation (7 mos) was previously reported, but to our knowledge, this is the first report with a survival period of > 10 years8. The favorable outcome and low rate of CTD flare posttransplantation could result from the intensive immunosuppressive treatment during and after lung transplantation, aimed at preventing acute rejection.
Some PM/DM pathogenesis hypotheses suggest an initial immune reaction occurring in the lung after exposure to environmental factors such as viral infection or smoking, inducing a break in self-tolerance and an autoimmune response3. If so, after lung transplantation, the autoantigen source would be removed, explaining the disappearance of the anti-MDA5 antibody and the absence of relapse of ILD or DM symptomatology in our patient. Subjects with higher baseline anti-MDA5 titers had a worse prognosis in case series of patients with RPILD, while anti-MDA5 levels seemed to correlate with disease activity, suggesting a possible pathogenic role for this autoantibody9,10.
This report shows the benefit of lung transplantation as a rescue therapy for therapy-resistant RPILD associated with anti-MDA5 antibody. Collective international data on lung transplantation outcomes in PM/DM patients with ILD are warranted to orient the future use of this procedure.
Acknowledgment
We thank Dr. Livia Casciola Rosen, Johns Hopkins School of Medicine, USA, for testing the first serum sample of this patient for anti-MDA5 antibodies, and Dr. Marius Wick for providing the annotated muscle magnetic resonance images.
Footnotes
Grant support for Dr. Leclair is from the Visithan-Khy Award from l’Association des Médecins Rhumatologues du Québec, Canada, and the Jewish General Hospital Department of Medicine Foundation Fund, Montreal, Québec, Canada. Grant support for Dr. Lundberg is from the regional agreement on medical training and clinical research between Stockholm County Council and the Karolinska Institutet, the Heart and Lung Foundation, and the Konung Gustaf V’s and Queen Victoria’s funds.








{kind=link}
{kind=link}