

Abstract
Objective. Our main objective was to assess the relationship between body composition (BC) and response to tumor necrosis factor-α (TNF-α) blocker treatment in patients with ankylosing spondylitis (AS). Our secondary objective was to evaluate the change of BC after treatment, accounting for sex and age.
Methods. All included patients fulfilled the modified New York criteria for AS and were naive to TNF-α blocker. They were followed for at least 6 months after the start of etanercept or adalimumab. The Ankylosing Spondylitis Disease Activity Score containing C-reactive protein (ASDAS-CRP) and the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) were reported. BC was assessed by whole body dual-energy X-ray absorptiometry. Body fat percentage (BF%), fat mass index (FMI), and fat free mass index (FFMI) were reported as absolute values and as percentiles.
Results. Forty-one patients were included (61% men). The median followup was 14.3 months (interquartile range 8.4–19.4). After multivariate regression analysis, more fat at baseline (BF%, FMI, or FMI percentile) was significantly related with a lower chance of achieving a clinically important improvement of the ASDAS-CRP or BASDAI after treatment. The body composition did not change significantly after treatment, but there was a trend toward muscle recovery in men (FFMI change from 34.0th to 37.4th percentile).
Conclusion. Higher body fat content at baseline was independently associated with a worse response to treatment with TNF-α blockers, measured by ASDAS-CRP and BASDAI change, and might contribute to the lower response rates in female patients. Also, there is a trend toward muscle mass recovery in male patients after treatment.
To date, only very limited data are available regarding sex differences and body composition in ankylosing spondylitis (AS) and its influence in the response to tumor necrosis factor-α (TNF-α) blockers. Several studies have demonstrated that women with AS are less responsive to TNF-α blockers and have a shorter drug survival1,2,3,4,5. Also, being overweight or obese, according to the body mass index (BMI) classification, has been associated with a lower rate of success6,7,8,9. This might be explained by differences in body composition because women have higher total body fat10, and adipose tissue is capable of producing different proinflammatory cytokines, called adipokines, which can influence immunological processes11,12.
However, although BMI is widely used, this measure does not distinguish between muscle and fat mass, therefore it cannot identify body composition characteristics and their effects on the disease13. Dual-energy X-ray absorptiometry (DEXA) can accurately measure whole body and regional distribution of fat and lean tissue in men and women, compared to anthropometric methods such as BMI, with a very low radiograph-associated radiation and relatively modest cost compared with computed tomography (CT) and magnetic resonance imaging. It also has shown a very strong correlation to CT measurements14,15,16. There is scarce information about body composition change in patients with AS under TNF-α blocker treatment. French researchers found a significant increase in body weight, mostly because of fat mass, and an increase in abdominal obesity, with significant increase in visceral (VAT) and subcutaneous adipose tissue after treatment17,18,19. Another group found similar changes in 12 patients with AS, although these were not significant for VAT increase20. However, these studies did not account for the natural tendency for weight gain and changes in adipose tissue distribution with age21. Our main objective was to assess the relationship between body composition, measured by DEXA, and response to TNF-α blocker treatment in a cohort of patients with AS who have not received biologic treatment before. Our secondary objective was to evaluate the change of body composition in patients under TNF-α treatment, accounting for sex and age.
MATERIALS AND METHODS
Study design
Retrospective cohort study.
Setting
The Amsterdam Rheumatology and Immunology Center (ARC) initiated a prospective cohort of patients with axial spondyloarthritis (the AmSpA cohort) in 1999, in which all patients who started with TNF-α blockers were included. For our study, we analyzed the patients who started adalimumab (ADA) or etanercept (ETN), which were most commonly used at that time, and no other TNF-α blockers because there were no financial resources to perform DEXA in all other TNF blockers.
Participants
We selected, from the AmSpA cohort, all the consecutive patients who fulfilled the diagnosis of AS according to the 1984 modified New York criteria, were > 18 years old, and had a DEXA analysis before the start of TNF-α blocker treatment and at least 6 months thereafter. Only patients who were TNF-naive before the DEXA was performed and who were eligible for the start of TNF-α blockers because of high disease activity were included. The first DEXA was performed in January 2008 and the last in January 2016.
Baseline variables
The data regarding sex, age, disease duration (yrs with symptoms and yrs since diagnosis), extraarticular manifestations, use of nonsteroidal antiinflammatory drugs (NSAID), disease-modifying antirheumatic drugs (DMARD) and/or prednisone, and tobacco use by a yes/no questionnaire were collected.
Body composition variables
The body composition variables were assessed before the start of the TNF-α blocker and at the end of followup, when the second DEXA analysis was performed.
To calculate the BMI, body weight was measured during patients’ visits, without shoes and clothes, to the nearest 0.1 kg on a digital scale (Seca Deutschland). Height was measured without shoes, to the nearest 1 cm. BMI was calculated as weight/height2 (kg/m2) ratio and categorized according to sex independent of the World Health Organization categories (underweight < 18.5, normal range 18.5–24.99, overweight range 25–29.99, obese ≥ 30)22.
Body composition was assessed with a whole body DEXA (GE Lunar iDxa, GE Corporate) and the measurements were carried out according to the protocol of the manufacturer. The total body mass (TBM) is the sum of the total fat mass, total lean mass (LM), and bone mineral content (BMC). Fat mass (sum of trunk, both arms and legs, and head) was reported as body fat percentage (ratio fat mass/TBM). Because absolute fat mass is dependent on height, the fat mass index (FMI) was calculated (fat mass kg/height m2). Fat free mass (FFM) was calculated as LM + BMC. Likewise, the FFM index was calculated (FFM kg/height m2). Android and gynoid fat percentages were analyzed, and the android to gynoid fat ratio was calculated. Body fat percentage, FMI, and FFM index were also reported as percentiles, according to the reference population tables23, which are stratified by ethnicity, age, and sex (the 50th percentile reflects the median of the reference population).
Disease activity variables
The disease activity variables were assessed before the start of the TNF-α blocker and at the end of followup, when the second DEXA analysis was performed.
These variables were recorded: C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) levels, the Ankylosing Spondylitis Disease Activity Score containing CRP (ASDAS-CRP; < 1.3 = “inactive disease;” range 1.3–2 = “moderate disease activity;” range 2.1–3.5 = “high disease activity;” > 3.5 = “very high disease activity”), and the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI; a cutoff of 4 is used to define active disease). Patients were classified according to the ASDAS-CRP response cutoffs (a Δ ≥ 1.1 is clinically important and ≥ 2 is a major improvement), and by the recently proposed minimum clinically important improvement cutoff for BASDAI (a Δ ≥ 1.1) in patients with a baseline BASDAI ≥ 424.
Statistical analysis
The data were analyzed using SPSS 22.0 for Windows (SPSS). The patients were stratified by sex for the analysis. Categorical variables were described as frequencies and/or percentages, and quantitative variables were described as mean and SD for those normally distributed or median and interquartile range (IQR) for those not normally distributed. Changes in body composition and disease activity measurements from baseline to end of followup were analyzed using the Student t test for paired variables or Wilcoxon signed-rank sum test, as appropriate. Associations between variables and differences between men and women were assessed using the Student t test for normally distributed continuous variables, the Mann-Whitney U test for not normally distributed continuous variables, and the chi-square test or Fisher’s exact test for categorical variables.
For the analysis of the main outcome (influence of body composition on disease activity change after treatment with ETN or ADA), we first performed a univariate analysis (logistic regression for the categorical achievement of a clinically important improvement of ASDAS-CRP or BASDAI, and linear regression for the improvement of ASDAS-CRP or BASDAI as continuous variables), analyzing the relationship between the baseline variables, the biologic used, the body composition, and the improvement of ASDAS-CRP or BASDAI after treatment. The variables that were found to be significantly related to the improvement of ASDAS-CRP and BASDAI were included in the multivariate analysis. The covariates included in the multivariate analysis model were age, sex, disease duration (yrs with symptoms), time of followup, NSAID and DMARD use, the baseline value of the dependent variable, and other covariates that had a p value < 0.05 in the univariate analysis if appropriate. For percentiles, we did not include age and sex in the multivariate analysis because the percentiles were already stratified by those variables. Statistical significance was defined as p < 0.05. In case of missing data, the analysis was performed only with the available data.
Ethical approval
All patients gave written informed consent prior to participation in the study, according to the Declaration of Helsinki. The study protocol was approved by the Medical Ethical Committee of the VU University Medical Center, Amsterdam, the Netherlands (approval number 2005-179).
RESULTS
Baseline characteristics
Forty-one patients were included, of whom 25 (61%) were men. These characteristics were similar between men and women: age, years with symptoms, HLA-B27 positivity, extraarticular manifestations, percentage of tobacco, and NSAID and DMARD use (Table 1). None of the patients used prednisone.
Baseline characteristics of 41 TNF-α blocker–naive patients with ankylosing spondylitis, stratified by sex. No p values were significant.
Followup
The median followup was 14.3 months (IQR 8.4–19.4) for all patients: 16.4 months (IQR 11.9–19.6) for men and 12 months (IQR 7.3–17.8) for women, without significant difference between the 2 groups. ETN was started in 17 patients (41.5%): 10 men (40%) and 7 women (43.8%), and the other patients received ADA. None of the patients interrupted the use of the TNF-α blocker before the end of followup.
Body composition according to sex
BMI was higher in women, with a higher percentage of patients classified as overweight or obese, but the difference did not reach statistical significance. At baseline and after treatment, women had a significantly higher body fat percentage and FMI, and lower FFM index and android to gynoid fat ratio as absolute values (Table 2). However, after adjusting for age and sex, women had similar percentiles for body fat percentages and FMI compared with men, and significantly higher percentages for FFM index that was remarkably low in men, probably reflecting muscle wasting (Figure 1).
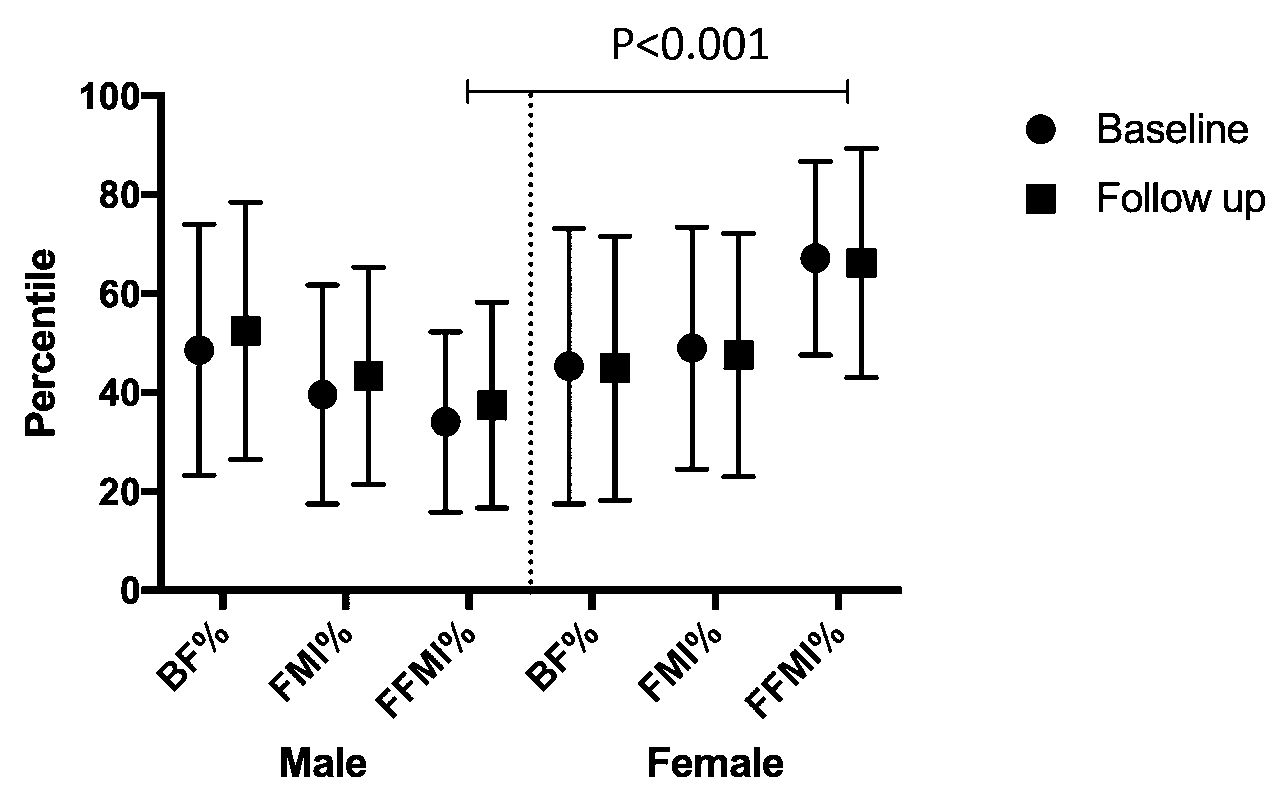
BF%, FMI, and FFMI percentiles according to reference population tables, stratified by sex. At baseline and followup, the FFMI was significantly higher in female patients (p < 0.001). Median followup was 14.3 months (IQR 11.2). BF%: body fat percentage; FMI: fat mass index; FFMI: fat free mass index.
Body composition characteristics at baseline and followup stratified by sex.
Regarding the change from baseline to followup, there was a significant mean increase of 0.06 in the android to gynoid fat ratio (SD 0.1, p = 0.001) in the whole group. Other variables did not show a significant change. Twenty percent of the male patients changed from being categorized by BMI as normal weight at baseline to overweight or obese after treatment, with a significant increase of BMI (median 0.5, IQR 0–1.1, p = 0.027), fat mass (mean 1.3 kg, SD 3.1, p = 0.046), and android to gynoid fat ratio (mean 0.1, SD 0.1, p = 0.001).
There was a statistically significant difference between men and women in the change from baseline to end of followup only for the android to gynoid fat ratio increase (greater increase in men, mean difference 0.1, SD 0.03, p = 0.048).
For body fat percentage, FMI, and FFM index percentiles, there was no statistically significant change from baseline to the end of followup, or difference of change between men and women, but there was a trend toward an increase in all the percentiles in men and a decrease in women (Figure 1).
The change of body composition variables was not related to the response to treatment measured by ASDAS and BASDAI change.
Disease activity
At baseline, 78% of the patients had an ASDAS-CRP ≥ 2.1 and 75.6% had a BASDAI ≥ 4 (Table 3).
Disease activity markers at baseline and followup.
After treatment with TNF-α blockers, the decrease of disease activity was statistically significant for all the measurements as continuous variables in the whole group and in men when analyzed separately. In women, only the decrease of ESR reached statistical significance (Supplementary Table 1, available with the online version of this article). There was no statistically significant difference in the change after treatment between men and women, or between ADA and ETN.
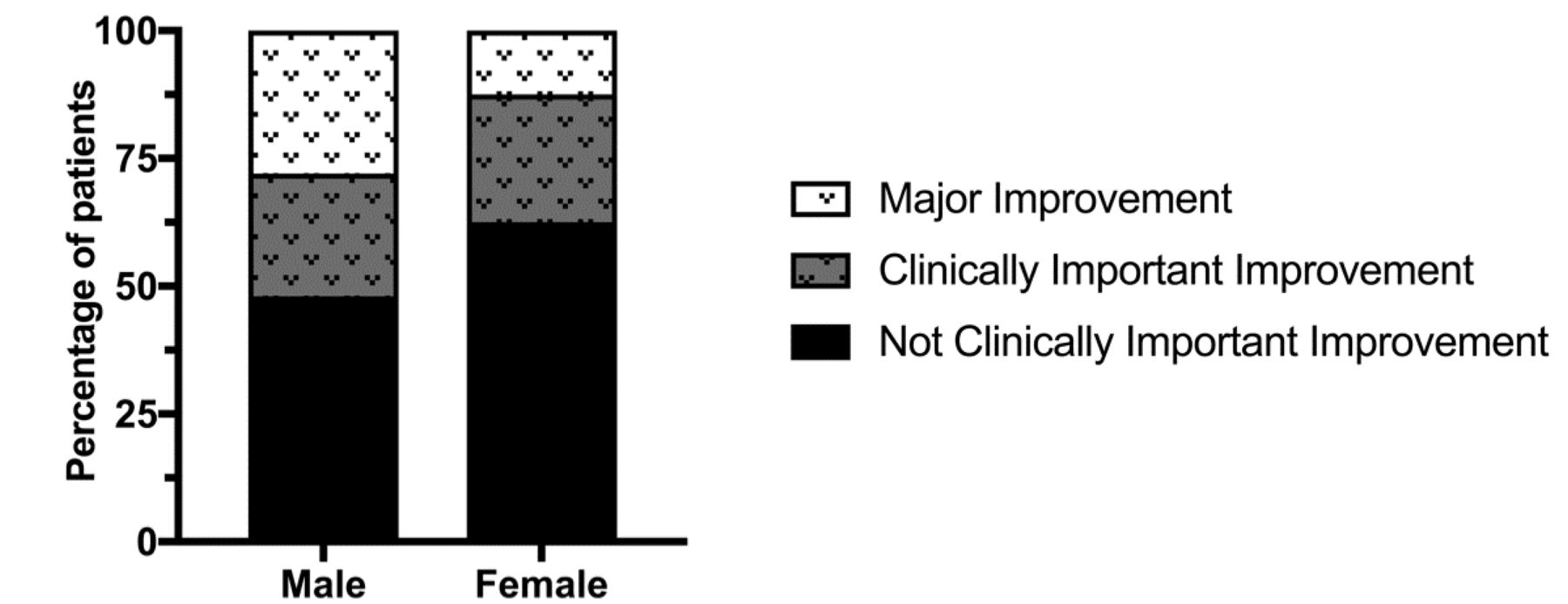
A clinically important improvement of the ASDAS-CRP was achieved by 46.4% of the patients, 52% of men versus 37.5% of women (Figure 2). The minimum clinically important improvement of the BASDAI was achieved by 51.6% of the patients who had a BASDAI ≥ 4 at baseline (only 35.7% of the female patients vs 64.7% of male). The difference in response rates between men and women, and between ADA and ETN users, did not reach statistical significance.

Response to tumor necrosis factor-α blocker treatment according to ASDAS-CRP change stratified by sex. Fifty-two percent of men had at least a clinically important improvement, whereas only 37.5% of women did. The differences were not statistically significant. ASDAS: Ankylosing Spondylitis Disease Activity Score; CRP: C-reactive protein.
Influence of body composition in disease activity
A higher BMI, body fat percentage, fat mass, FMI, and FMI percentile at baseline were significantly associated with a lower chance of having at least a clinically important improvement according to the ASDAS-CRP in the univariate analysis. For the BASDAI minimum clinically important improvement, there were significant associations for higher body fat measurements and a worse outcome in the univariate analysis (Supplementary Table 2, available with the online version of this article). After multivariate analysis, only the following associations remained statistically significant: higher body fat percentage, FMI or FMI percentile at baseline lowered the chance of achieving at least a clinically important improvement according to ASDAS-CRP change. The same relationship was found between FMI percentile at baseline and the chance of achieving the minimum clinically important improvement for BASDAI (Table 4).
Multivariate logistic regression analysis resultsa.
Regarding the improvement of the ASDAS-CRP and BASDAI as continuous variables, there were significant associations in the univariate analysis between higher values of different body fat measurements and a worse outcome (Supplementary Table 3, available with the online version of this article). After multivariate analysis, a higher body fat percentage at baseline (β coefficient −0.08, 95% CI −0.1 to −0.02; p = 0.012), FMI at baseline (β coefficient −0.2, 95% CI −0.3 to −0.04; p = 0.016), and FMI percentile at baseline (β coefficient −0.02, 95% CI −0.04 to −0.01; p = 0.004) remained significantly associated with a lower chance of ASDAS-CRP improvement. A higher body fat percentage percentile at baseline (β coefficient −0.03, 95% CI −0.1 to −0.002; p = 0.038) and FMI percentile at baseline (β coefficient −0.04, 95% CI −0.07 to −0.01; p = 0.012) were also related with a negative change of BASDAI.
After multivariate analysis, separately for men and women, and for ADA and ETN users, no significant associations were found between body composition variables and response to treatment.
DISCUSSION
In our study, a higher body fat content at baseline was associated with less chance to achieve at least a clinically important response to treatment with a TNF-α blocker, according to the ASDAS-CRP and BASDAI change.
To our knowledge, ours is the first report regarding the relationship between fat mass measurements and response to TNF-α blocker treatment in patients with AS. This supports the concept that adipose tissue, through the release of different bioactive molecules and hormones such as adiponectin, leptin, resistin, TNF, and interleukin 6, can participate in different inflammatory and autoimmune processes11,12. Also, more body fat content could limit the absorption and distribution of the TNF-α blockers administered.
It is remarkable that we did not find a relationship, after multivariate analysis, between higher BMI and worse response to treatment as reported in other studies6,7,8,9, confirming that BMI is not capable of identifying the effect of body composition on the disease.
The influence of body fat on the response to treatment seems to be independent of height, because the FMI adjusts the fat mass (kg) for height, and also independent of age and sex, because we controlled for these variables in the multivariate analysis, and — most important — because the FMI percentile is stratified by age and sex according to the reference population tables, which are specific for the DEXA machine used in our study23.
In our study, men had lower than expected fat free mass index percentile, which was also significantly lower than women, probably reflecting muscle wasting in response to persistent inflammation. This is consistent with the results found in our analysis25. In absolute numbers, the FFM and FFM index did not improve after treatment, but these measurements do not take into account the changes associated with age. The FFM index percentile, which takes into account age and sex, improved in men, although not significantly, by 3.4%, possibly because of muscle recovery in response to TNF-α blocker treatment.
The patients had a significant increase of the android to gynoid fat ratio (more pronounced in men) that is associated with visceral adiposity and cardiometabolic risks26,27,28, and might contribute to the increased cardiovascular risk in patients with AS.
Men had a better response to treatment, because 52.0% achieved at least a clinically important ASDAS-CRP improvement, versus only 37.5% of women, and the mean changes for the ASDAS-CRP and BASDAI were greater in men. There could be a relationship between the worse response to treatment in women and the higher content of fat, because women had higher fat mass, body fat percentage, and FMI than men, and we have shown that a higher body fat content is independently associated with a worse response to TNF-α blockers.
Our study has some limitations. We were not able to find statistically significant worse outcomes in women versus men, or a significant relationship between fat mass indices and worse outcomes in women, probably because of the low number of patients.
Higher body fat content at baseline was independently associated with a worse response to treatment with TNF-α blockers, measured by ASDAS-CRP and BASDAI change, and might contribute to the lower response rates to treatment in female patients. In addition, there was a trend toward muscle mass recovery in male patients after treatment with TNF-α blockers.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
This study was endorsed by an Assessment of Spondyloarthritis international Society Fellowship grant.
- Accepted for publication May 25, 2017.








{kind=link}
{kind=link}