

Abstract
Objective. Anterior uveitis (AU) is an intraocular inflammatory condition closely linked to spondyloarthritis (SpA). Clinical disease variables may often underestimate the true effect of the disease on patient’s quality of life. This study examines AU and associated undiagnosed SpA using established quality-of-life tools to inform clinicians of the effect of these diseases.
Methods. The Dublin Uveitis Evaluation Tool (DUET) algorithm was developed and validated in a cohort of consecutive patients with AU who were all screened by a rheumatologist for the presence of SpA. This same cohort completed vision-related [Vision Core Measure 1 (VCM1)] and general health [Medical Outcomes Study Short Form-36 (SF-36)] questionnaires when AU was active and resolved.
Results. VCM1 scores improved with AU resolution. VCM1 did not correlate with vision at baseline, but did on resolution of inflammation. Physical SF-36 scores were reduced during AU episodes and improved on resolution remaining below those of population norms. Subanalysis revealed that SpA scores were more affected than the idiopathic AU group.
Conclusion. AU affects physical aspects of quality of life more than is appreciated by clinical variables, especially in those with pre-existing, undiagnosed SpA. This study is unique in examining the effect of SpA on patients prior to diagnosis. These results highlight the role of the ophthalmologist in identifying patients with SpA who present with AU using the DUET algorithm.
Uveitis refers to inflammation of the uveal tract, the middle vascular layer of the eye. Uveitis is defined by anatomical location1 with anterior uveitis (AU) occurring within the anterior chamber of the eye. This accounts for 50% to 92% of all cases of uveitis2,3,4. The reported incidence of AU is 17.4 to 52.4 cases per 100,000 person-years with a prevalence of 58.0 to 114.5 per 100,000 persons5,6,7,8. Symptoms include redness of the affected eye, blurred vision, pain, and photophobia. Whereas diseases such as diabetic retinopathy and age-related macular degeneration are more prevalent with older age, uveitis occurs in younger patients of working age. It accounts for 10% to 15% of all causes of blindness in the developed world9,10 with the consequent significant longterm personal and population-based burden of this disease.
AU may be idiopathic or may occur in the presence of systemic autoimmune conditions. Spondyloarthritis (SpA) is the most common systemic disease association2. The prevalence of SpA has been reported to be as high as 1.9%11. Major strides have been made regarding the treatment of patients with SpA. However, the major stumbling block toward overall success in SpA remains the poor recognition and consequent late referral to rheumatologists. While there have been some improvements, the average time to diagnosis of SpA from symptom onset remains greater than 6 years12.
Patients with backache of insidious onset that improves with exercise may not seek medical attention for years. In contrast, those with ocular pain, redness, and photophobia will seek urgent medical care13,14. Therefore, the ophthalmologist is uniquely placed to screen patients with AU for the presence of SpA. Previous work by our group developed and validated the Dublin Uveitis Evaluation Tool (DUET), a highly sensitive and specific algorithm to streamline referrals between ophthalmologists and rheumatologists15.
The effect of AU on the patient
The effect of AU on visual impairment is not known. Visual acuity (VA) is traditionally used as a marker of uveitis severity and activity, and is used as the primary outcome measure in many uveitis clinical trials. However, considered alone, it inadequately describes visual performance.
Vision-related quality-of-life (VR-QoL) questionnaires measure global effect of visual impairment on physical, psychological, and social functioning in day-to-day life. They provide an effective means of measuring visual functioning, as has been demonstrated for patients with glaucoma, retinal detachment, cataract, and uveitis16,17,18,19,20. Composite scores of disease activity in uveitis have been proposed, derived from objective clinical tests (VA, contrast sensitivity, and uveitis grading) and functional measurements (such as VR-QoL) assimilated into a single reliable and valid outcome21. In addition to VR-QoL, patient well-being can also be assessed using generic instruments that measure overall health-related quality of life (HRQOL), such as the Medical Outcomes Study Short Form-36 (SF-36) questionnaire, which is commonly used as an outcome measure in clinical trials22.
There are many possible reasons why patients with uveitis may perceive impaired quality of life, including visual impairment, pain, and worry about visual prognosis. Specifically, for noninfectious AU, the relationship with underlying undiagnosed systemic disease association is particularly relevant where patients may be experiencing grumbling systemic symptoms for many years. This cohort of patients is especially unique in that it offers the opportunity to evaluate the quality of life in patients with SpA prior to the diagnosis.
It is important to understand the effect of uveitis on subjective and objective visual functioning and quality of life to measure the outcome of treatment and optimize disease management in general. In our study, we performed an evaluation of the effect of noninfectious AU on VR-QoL and HRQOL to provide a more global assessment of the effect of disease on patients.
MATERIALS AND METHODS
Setting of the research
Recruitment for this study was through the eye casualty unit at Royal Victoria Eye and Ear Hospital, Dublin, Ireland, to a dedicated research clinic. Approval was obtained from the local ethics committees (Royal Victoria Eye and Ear Hospital ethics committee approval number 20110701).
Patient selection
To minimize recruitment bias, consecutively attending patients with presumed immune-mediated acute AU who were over 18 years of age and capable of providing informed consent were included in our study. Patients with a history of intraocular surgery or penetrating or blunt eye trauma were excluded. Patients with evidence of viral etiology for their uveitis were also excluded. Patients with a known systemic etiology for their uveitis were excluded.
All recruited patients had a thorough clinical history undertaken. Best-corrected VA was measured using the Snellen or LogMAR VA charts and obtained using the patient’s own spectacle correction. VA was converted to logMAR VA. Slit lamp biomicroscopy of the anterior segment was undertaken to grade anterior chamber reaction as per the Standardization of Uveitis Nomenclature working group guidelines1. All patients had HLA-B27 status checked. Additional diagnostic investigations were performed if clinically indicated based on patient history and examination. “Baseline” examination refers to the patient’s first examination in the research clinic. “Resolution” refers to final examination prior to the patient’s discharge with no evidence of intraocular inflammation and cessation of topical treatment. Rheumatological assessment was carried out independently on all patients. Radiographs were taken where indicated and SpA was diagnosed as per the Assessment of Spondyloarthritis international Society classification criteria23 and the ClASsification for Psoriatic ARthritis criteria24.
Assessment of HRQOL and VR-QoL
Questionnaires that measure HRQOL have increasingly gained acceptance as useful tools for evaluating effect of disease and treatment on the patient. The SF-36 questionnaire is the most widely used generic HRQOL tool. As a generic tool, the SF-36 does not measure disease- or treatment-specific quality-of-life issues. The SF-36 consists of 8 scaled scores that are the weighted sums of questions in their sections. These include physical function, role physical, role emotional, social functioning, mental health, energy and vitality, pain, and general health perception. Patients rate their own health and how it limits them physically and mentally.
In ophthalmology, the concept of VR-QoL has developed and many questionnaires have been validated for the measurement of the effect of visual impairment on quality of life. One such questionnaire is the Vision Core Measure 1 (VCM1), a 10-item questionnaire that provides a subjective measure of concern regarding vision25. The patient rates the physical, social, and psychological effect of performing common daily activities because of problems with their eyesight. After a thorough explanation of how to complete the questionnaires, the SF-36 and VCM1 were self-administered in about 10 min.
Data analysis
To facilitate comparison with age- and sex-matched general population norms, the SF-36 subscale scores are presented as T scores, calculated using means and SD from the age- and sex-matched UK normative set26. For T scores, the normative dataset has a mean (SD) of 50 (10). Patient scores greater than 50 represent better-than-average quality of life and below 50 represent worse-than-average quality of life. The 8 domains of the SF-36 were summarized into the physical component summary score (PCS; derived from the physical functioning, role physical, bodily pain, and general health perception subscales) and the mental component summary score (MCS; derived from the energy/vitality, social functioning, role emotional, and the mental health subscales) to reduce the number of SF-36 variables for statistical analysis27.
The responsiveness of the VCM1 questionnaire to treatment and the accompanying change in vision were evaluated by calculating the effect size and the standardized response mean (SRM) for the group28. The effect size was defined as the mean change in the VCM1 score from baseline to resolution divided by its SD at baseline, and reflects the magnitude of the change in VCM1 in response to the treatment started at baseline. Cohen defines an effect size of 0.2 as a small change, 0.5 as a medium change, and ≥ 0.8 as a large change29. The SRM was defined as the mean change in the VCM1 score between baseline and resolution for the group divided by the SD of the change in score over the same period.
Statistical analyses were performed using Prism version 6.0d for Mac. All tests were 2-tailed and statistical significance attributed when p < 0.05. To counteract the problem of multiple comparisons, the Bonferroni method was used to give a new α value of 0.005. Patients and normative data were compared using independent Student t tests. Paired Student t tests were used to compare pre- and post-treatment data from the same patients. The associations between visual functions tests and quality-of-life scores were examined using Spearman correlation analysis.
RESULTS
Patient demographics
In total, 173 patients were recruited to our study. The clinical and demographic characteristics of the entire cohort are described in Table 1. As part of the inclusion criteria of the study, none of these patients had a known systemic-associated disease on recruitment. All patients underwent rheumatological screening to assess for the presence of SpA. The diagnosis of sarcoidosis was established following referral to a respiratory physician. History guided the necessity of a chest radiograph and serum angiotensin-converting enzyme level and onward referral based on these results. One patient who presented only with hypopyon uveitis was diagnosed with Behçet disease. He described a history of recurrent mouth ulcers, was HLA-B51–positive, and was referred for rheumatology opinion. He subsequently developed deep venous thrombosis.
The clinical and demographic details of the patient cohort. Consecutive patients (n = 173) attending the eye casualty unit at the Royal Victoria Eye and Ear Hospital, Dublin, with noninfectious AU without any known systemic associations were recruited to a dedicated research clinic. All patients had HLA-B27 checked and were screened by a rheumatologist for the presence of SpA. Further investigations were undertaken based on clinical history and examination. Values are n (%) unless otherwise specified.
Visual acuity
Overall, VA remained good in patients with AU. The mean (SD) LogMAR VA of the affected eye at baseline and resolution were 0.18 (0.24) and 0.06 (0.16), respectively, with a significant improvement in VA (p < 0.001) on resolution. A total of 86.6% and 95.4% patients had LogMAR VA of 0.3 (20/40) or better at baseline and resolution, respectively. VA recovered to normal in all patients except in those affected by amblyopia.
Vision-related quality of life
The mean (SD) of the VCM1 score of the patients at baseline and resolution was 1.06 (1.02) and 0.81 (0.92), respectively. There was a significant improvement in VCM1 scores from active AU to resolution (p < 0.001) with effect size and SRM of VCM1 being 0.26 and 0.32, respectively, indicating a small change in the VCM1 score in response to resolution of uveitis.
As shown in Figure 1, 14.6% at baseline and 11% at resolution had a VCM1 score of more than 2.0, which represents “more than a little” concern about vision. There was no correlation between the VCM1 score and affected eye VA at baseline. However, VCM1 score correlated weakly with affected eye VA at resolution. (Spearman r = 0.2, p = 0.047).
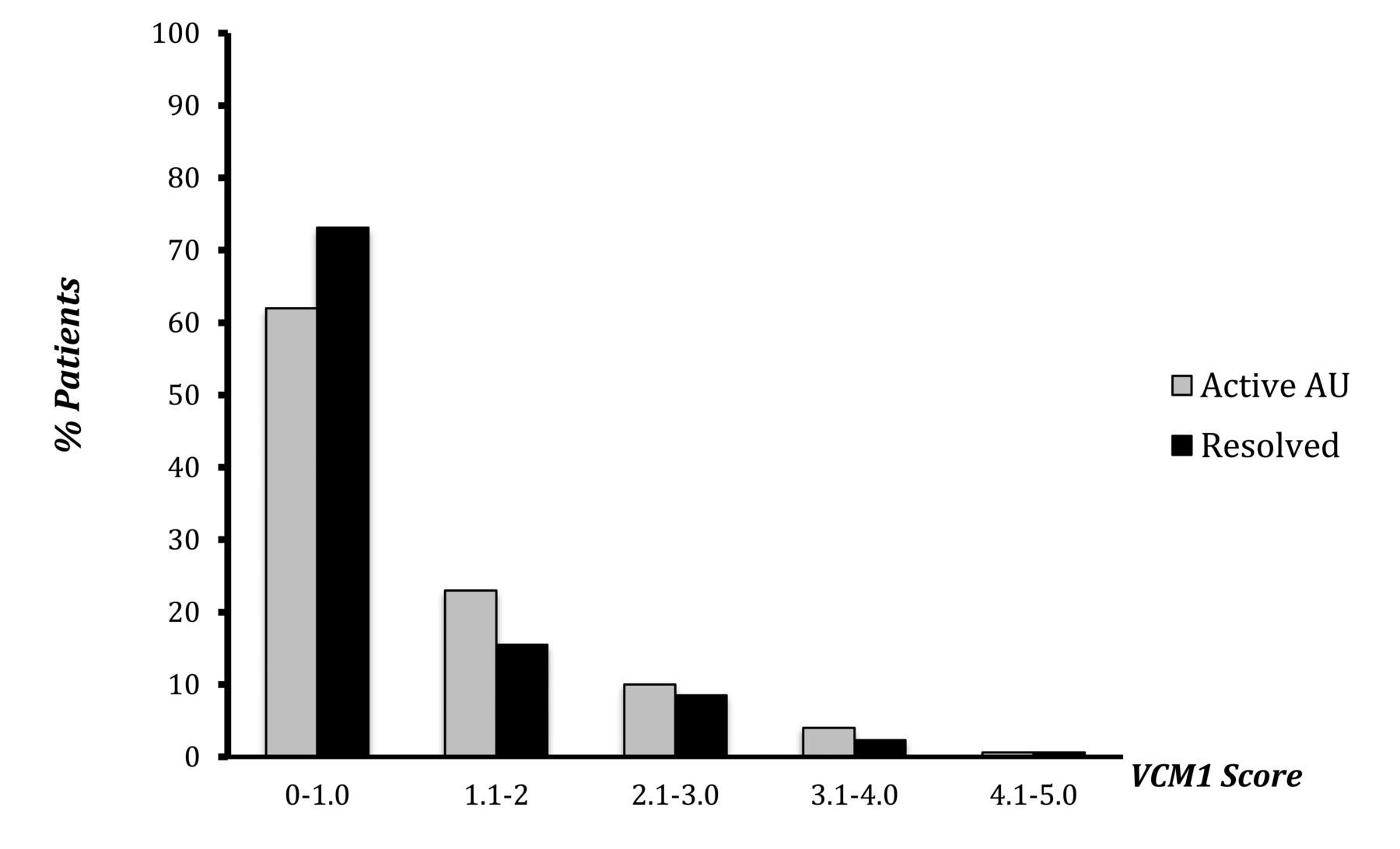
Vision-related quality of life in AU. VCM1 questionnaires were completed by the patients at recruitment and again at resolution (n = 173). Analysis shows a significant improvement in VCM1 scores on resolution of AU (p < 0.001). Only 14.6% of patients during active AU and 11% on AU resolution recorded a score of greater than 2.0, which represents “more than a little concern about vision.” AU: anterior uveitis; VCM1: Vision Core Measure 1.
Summary of HRQOL
The results of the SF-36 scores for the entire cohort are shown in Table 2. During active AU, all physical scores (physical function, role physical, pain) were affected (p < 0.0001), with patients also reporting significantly reduced social functioning (p < 0.0001). They also perceived their general health to be worse than that of the general population (p < 0.001). Overall, the PCS and MCS were reduced compared with the general population (p < 0.0001).
SF-36 subscale T scores for all patients with AU (n = 173) during active and resolved stages of AU compared with an age- and sex-matched population using UK normative data. Most SF-36 scores are reduced during the active phase of AU. While these improved on resolution, they remained below that of population norms. A significant improvement was seen for pain (p < 0.0001) with an SRM of 0.4; however, pain scores still remained significantly below population norms on resolution of AU (p = 0.0008).
All SF-36 scores improved on resolution of ocular inflammation with a significant improvement for pain (p < 0.0001), social functioning (p < 0.005), and energy and vitality scores (p < 0.005), as well as the composite PCS (p < 0.0001) and MCS (p < 0.0001).
Although the SF-36 scores did improve on resolution of ocular inflammation, physical function (p < 0.005), role physical (p < 0.0001), social functioning (p < 0.005), and pain (p < 0.005) remained below that of the general population. Similarly, while composite scores improved on resolution, both the PCS (p < 0.0001) and MCS (p < 0.001) remained worse than the general population on resolution of AU.
Given that all patients were subsequently screened by a rheumatologist, a new diagnosis of SpA was made in 41% of patients15. Subgroup analysis was therefore carried out by examining the SF-36 scores in those with a new diagnosis of SpA and those who had idiopathic uveitis. Patients with other systemic diagnoses were excluded (n = 5).
In the SpA group (n = 71; Table 3), questionnaires completed during the active stage of AU showed reduced scores for physical function (p < 0.0001), role physical (p < 0.0001), social functioning (p < 0.0001), and pain (p < 0.0001), as well as for PCS (p < 0.0001) and MCS (p < 0.0001). SF-36 questionnaires completed on resolution of AU showed the same scores remaining reduced. Only the pain score improved between active phase of AU and resolution (p < 0.0001) with SRM of 0.5. However, pain scores remained lower when compared with the general population (p < 0.001). Likewise, PCS and MCS scores improved on resolution of ocular inflammation (p < 0.0001, p < 0.001), but remained reduced compared with the general population (p < 0.0001, p < 0.001). Sex did not affect quality-of-life scores. However, SF-36 scores were normalized to age- and sex-matched norms. Over 90.5% of the patients with newly diagnosed SpA were HLA-B27–positive, therefore direct comparison between HLA-B27–positive and –negative cases within the newly diagnosed SpA group was not possible because of the small numbers of HLA-B27–negative cases.
SF-36 subscale T scores for the subgroup of patients with newly diagnosed SpA (n = 71) who presented with AU during active and resolved stages of AU compared with an age- and sex-matched population using UK normative data. Reduced physical scores during the active phase of AU remained affected on resolution with only pain scores significantly improving. However, pain scores remained significantly reduced compared with population norms (p = 0.0004).
For the idiopathic AU group (n = 97; Table 4), during the active AU stage, pain (p < 0.005) and social functioning (p < 0.0001) scores were reduced compared with the general population, with PCS (p < 0.0001) and MCS (p < 0.005) scores also reduced. On AU resolution, all SF-36 scores were comparable with the general population, with a significant improvement in pain (p = 0.01; SRM = 0.4), PCS (p < 0.0001), and MCS (p < 0.0001) scores.
SF-36 subscale T scores for the subgroup of patients with idiopathic AU (n = 97) during active and resolved stages of AU compared with an age- and sex-matched population using UK normative data. On AU resolution, all SF-36 scores were comparable with the general population with a significant improvement in pain (p < 0.005, SRM = 0.37).
A direct comparison of the newly diagnosed SpA patients with AU and the patients with idiopathic AU is shown in Table 5. The SpA group had significantly worse physical function (p < 0.005), role physical (p < 0.005), pain (p < 0.005), and PCS (p < 0.005) during the active AU phase. While the SF-36 scores remained lower in the SpA group on resolution of AU, only physical function was statistically lower at this stage in the SpA group (p < 0.005). Of note, patients’ perception of their health, as indicated by general health perception score, was not different between the 2 groups. Patients with newly diagnosed SpA had a higher number of previous AU episodes (p < 0.001); however, the number of previous AU flares did not correlate with quality-of-life scores.
SF-36 subscale T scores for comparing AU patients with SpA (n = 71) or idiopathic disease (n = 97) during the active and resolved stages of AU inflammation. UK age- and sex-matched normative data were used in calculating the T scores. Those with underlying SpA had worse physical scores during active AU. While SF-36 scores remained lower in the SpA on resolution of AU, only physical function was statistically lower at this stage in the SpA group (p < 0.005). Of note, patient perception of their health, as indicated by GHP score, was not different between the 2 groups.
All SF-36 subscales cohorts correlated with VCM1 scores at baseline and resolution (r = −0.19 to −0.45 at baseline, and r = −0.36 to −0.53 at resolution). However, there was no correlation between any SF-36 subscales and VA at baseline or resolution.
DISCUSSION
Quality-of-life questionnaires are well established as useful tools for measurement of patients’ perception of their health problems. They offer an insight into the effect of the disease on the patient that may not be obvious from measurement of clinical variables of disease. They are often used to evaluate treatment efficacy in clinical trials. Combining objective measures of inflammation and vision with subjective assessments such as VR-QoL and HRQOL scores into a composite scoring system may improve the clinical approach to managing the patient with uveitis.
Clinical characteristics and demographics of our cohort reflect those reported in similar international groups2,30,31,32. Sex preponderance is seen in AU with men being affected almost 1.5 times more than women. The mean age of presentation was similar in both men and women at 41.5 years. These results are consistent with previously published reports31,33,34. Most AU is idiopathic with a range of 38%–88%, depending on geographical region34,35,36,37.
Although both VA and VCM1 scores were affected, there was no significant correlation during the active phase of AU. This suggests that VR-QoL is affected more than is quantifiable by VA alone. Such factors may include AC activity, ocular pain, photophobia, decreased contrast sensitivity, or the use of cycloplegia in the early treatment of AU. The ophthalmologist may not consider AU as a disease, although it is severely sight-threatening; however, the results of the VCM1 scores show that the clinician needs to be aware of the effect of the disease on VR-QoL and appreciate the effect on the patient beyond VA measurement alone. On resolution of inflammation, both VA and VCM1 scores improved and were significantly correlated at this point. There was no difference in VR-QoL between those with systemic disease and those without. Previous research on a large non-homogeneous group of patients with uveitis found that patients with uveitis reported a markedly poorer visual functioning and general health status than healthy subjects38. Herpetic AU has also been found to affect VR-QoL to a moderate degree19. Depression is thought to be a significant and underrecognized comorbidity in patients with ocular inflammatory conditions39, although it is difficult to decipher whether quality of life affects the immune system itself or if this results from the effect of the immune system on quality of life40.
The SF-36 results suggest that this questionnaire may have relevance in distinguishing aspects of HRQOL in patients with AU. HRQOL scores were reduced during AU with significant reduction in the composite PCS and MCS scores. Pain is the most severely affected subscale; the largest SRM is seen on resolution. While all scores improved on resolution of inflammation, many subscale scores remained significantly lower than those of matched population norms.
Our quality-of-life study offers a unique insight into patients with underlying SpA and the occurrence of an episode of AU. Ankylosing spondylitis is known to affect patient’s quality of life41,42,43; however, this is the first study we are aware of that examines the effect of SpA on the patient prior to its diagnosis. All patients were recruited to our study through an ophthalmic casualty department, where their main reason for presentation was for symptoms of AU and not SpA. Although none of the patients were aware of their diagnosis of underlying SpA when presenting with AU, those who were subsequently diagnosed had significantly reduced quality of life scores, particularly for PCS, which remained reduced even after resolution of inflammation. The SF-36 results highlight the presence of underlying symptoms and illustrates the effect of SpA on the patient, even though the patient is unaware of the diagnosis. An episode of AU further reduces the patient’s quality of life acutely in those with SpA, but scores do not return to normal, as occurs in the idiopathic group on resolution of the AU. These results underline AU as a very acute disease that affects the patient’s physical and social functioning and therefore requires medical attention by an ophthalmologist. The onus is thus on the ophthalmologist, using the DUET algorithm15 to appropriately refer those at risk of having an underlying SpA.
The early diagnosis and treatment of SpA has consistently been shown to improve short- and longterm outcomes44,45,46. It is imperative that efforts are made to expedite its diagnosis. The results of our study are unique in identifying reduced quality of life scores in patients with underlying SpA prior to diagnosis. Scores decrease further on development of an episode of AU, which is when the patient attends the acute ophthalmology service. Previous published work on this same cohort of patients described the role of the ophthalmologist in recognizing SpA through specific clinical questions regarding backache. Quality-of-life questionnaires help the clinician to understand the true effect of disease on a patient. Results from the VCM1 and SF-36 questionnaires in patients with AU and SpA identify the physical and mental effects of these diseases on patients more than can be appreciated by clinical variables alone. Composite scores that include quality-of-life questionnaires as well as clinical variables may prove more useful for the clinician in assessing disease effect and response to treatment in the future.
Footnotes
Supported by the Research Foundation, Royal Victoria Eye and Ear Hospital, Dublin, Ireland.
- Accepted for publication April 28, 2017.








{kind=link}