

Abstract
Objective. To determine whether anticyclic citrullinated peptide antibodies (anti-CCP) and rheumatoid factor (RF) are risk factors for 10-year cardiovascular disease (CVD) in patients with rheumatoid arthritis (RA).
Methods. Analyses were performed using data from the Nijmegen early RA inception cohort, in which patients with newly diagnosed RA, consecutively included since 1985, were regularly followed up. Anti-CCP and RF were determined at baseline (diagnosis). Outcome was the first cardiovascular disease (CVD) event [ischemic heart disease, nonhemorrhagic cerebrovascular accident (CVA), or peripheral artery disease (PAD)] after baseline as retrieved from physician diagnosis. Fatality was checked against death certificates. Cox regression including correction for baseline confounders was performed to estimate the effect of anti-CCP, RF, and their interaction on 10-year CVD-free survival.
Results. Of 929 patients included, 628 were anti-CCP–positive and 697 were RF-positive. During followup, with a median of 7.5 years, 162 CV events were observed (101 ischemic heart disease, 45 CVA, and 16 PAD), of which 15 were fatal. The HRadjusted for anti-CCP was 1.17 (95% CI 0.82–1.67) and the HRadjusted for RF was 1.52 (95% CI 1.00–2.30). The association of RF positivity with CVD was even stronger in the anti-CCP–negative patients: HRadjusted 2.09 (95% CI 1.18–3.71). There was no significant interaction (p = 0.098) between anti-CCP and RF.
Conclusion. Rather than anti-CCP, presence of RF was associated with CVD in this cohort of patients with RA.
- RHEUMATOID ARTHRITIS
- ANTICYCLIC CITRULLINATED PEPTIDE ANTIBODIES
- CARDIOVASCULAR DISEASE
- RHEUMATOID FACTOR
The incidence and mortality of cardiovascular diseases (CVD) is considerably higher in patients with rheumatoid arthritis (RA) compared with the general population1,2. Compared to non-RA subjects, the overall effect of traditional CVD risk factors is less in patients with RA, suggesting other factors to contribute to the development of CVD in RA3. The presence of anticyclic citrullinated peptide antibodies (anti-CCP) is associated with higher disease activity over time and more severe radiological damage in RA4, is involved in the activation of leukocytes and the proatherogenic status of patients with RA5, and is associated with a worse CV risk profile6. It can, therefore, be suggested that the highly RA-specific anti-CCP serves as a link between RA and CVD in these patients. However, evidence for a direct relation between anti-CCP and CVD in several cohorts of patients with RA is equivocal7,8,9,10,11,12,13. Presence of rheumatoid factor (RF) is closely associated with presence of anti-CCP positivity in RA, and for RF the evidence for an association with CVD is unclear7,9,10,13.
Therefore, the aim of our study was to determine whether anti-CCP and RF are risk factors for 10-year CV morbidity in Dutch patients with RA.
MATERIALS AND METHODS
Study population
Analyses were performed using data from the Nijmegen early RA inception cohort, in which patients with newly diagnosed RA were consecutively included. They had attended the outpatient clinic of the departments of rheumatology at the Radboud University Medical Centre (since 1985) or the St. Maartenskliniek in Nijmegen (since 1990). At inclusion, patients had a disease duration of less than 1 year, were diagnosed with RA according to the American College of Rheumatology (ACR) 1987 classification criteria and/or the ACR/European League Against Rheumatism 2010 criteria, and were naive to disease-modifying antirheumatic drug (DMARD). Eligibility criteria consisted of a known anti-CCP status, no history of CVD at baseline, and a followup of at least 6 months. A total of 1047 patients were included in the cohort at the time of analysis. Of these patients, 75 without values for anti-CCP were excluded, as well as 43 who had a followup of less than 6 months, resulting in a total of 929 eligible patients.
Ethical considerations
All patients who were included in the cohort were informed orally and in writing and all patients provided written informed consent. According to the observational design of this study and in agreement with Dutch law and regulations, approval of an ethical committee was not needed.
Clinical assessments at baseline
Clinical assessments at diagnosis with RA (baseline) were performed by a rheumatologist or trained research nurse and included drawing blood samples for determining anti-CCP, RF, and erythrocyte sedimentation rate, while 1 sample was stored frozen. A swollen joint count and a tender joint count (of 28) were performed and the patient filled in a visual analog scale to indicate the patients’ global assessment (PtGA) of disease activity. The Disease Activity Score in 28 joints (DAS28) was calculated using the usual formula. Time-averaged DAS28 for each patient was calculated using the trapezoid method, allowing for differences in number and spacing of followup visits. At baseline, the patients also filled in the disability section of the Health Assessment Questionnaire (HAQ). Smoking habits and alcohol use (patient report), family history of CVD, and comorbidities and treatment information at baseline were derived from the patient charts. Lipid levels [total cholesterol (TC), high-density cholesterol] at baseline were determined using stored blood samples.
Anti-CCP and RF
Anti-CCP titers were determined using ELISA (anti-CCP2 ELISA, Eurodiagnostica) or fluorescent-enzyme immune-assay (FEIA; EliA, Phadia). Anti-CCP status was regarded as positive when concentrations exceeded 25 U/ml or 10 U/ml, respectively. Any lower value was considered negative. Exact titers were available for 339 patients. To compare ELISA and FEIA values, titers were converted to times above the upper limit of normal (ULN). RF positivity was assessed at the local laboratory for clinical chemistry, using in-house ELISA with 10 U/ml as the limit to determine positivity; RF titers were not available.
Cardiovascular disease
Disease outcome was the first (nonfatal or fatal) CVD event, retrieved from physician diagnosis by extensive review of medical charts and electronic patient files, including medical correspondence and history. CVD was defined as ischemic heart disease (IHD; including myocardial infarction, revascularization procedure, unstable angina pectoris), nonhemorrhagic cerebrovascular accident (CVA), or peripheral artery disease (PAD). All deaths were verified from death certificates, provided by Statistics Netherlands. CVD events included deaths because of CVD, excluding cerebral hemorrhage and noncoronary cardiac death (i.e., arrhythmia).
Statistical analysis
Anti-CCP was the determinant of primary interest. Potential confounding variables were compared between the anti-CCP–positive and –negative group by use of the chi-square test, Wilcoxon rank-sum test, or Student t test. To determine whether anti-CCP titers differed among potential confounding variables, we used Pearson correlation or the Student t test. A cutoff value of p < 0.2 was chosen to include variables potentially significant in a larger sample. Missing values on potential confounding variables were imputed using multiple imputation analysis with 20 repetitions. Followup was calculated from date of diagnosis to date of event. Censoring was performed at date of last observation or end of study. Unadjusted survival rates were estimated using the Kaplan-Meier method, and compared using the log-rank test. Multivariable Cox proportional hazard analyses were conducted to correct for confounding and to estimate HR with 95% CI for the association between anti-CCP status, RF status, and their interaction, with CVD-free survival. Individual potential confounding variables were consecutively added to the model with anti-CCP status (or RF status, or anti-CCP status with RF status and an interaction term) and remained in the model when the regression coefficient of anti-CCP changed ≥ 10%. Similarly, the relation between anti-CCP titers and CVD-free survival was analyzed. The cumulative survival function of anti-CCP titers was plotted, and individual predictions for 10-year CVD-free survival were plotted against the individuals’ titer. All statistical analyses were performed using SPSS version 20.0 (IBM Statistics). Given the limited number of several types of events, we decided to perform and present the analysis on pooled CVD events only.
RESULTS
Patient characteristics
Among the 929 patients included, 628 were anti-CCP–positive and 301 anti-CCP–negative, 697 were RF-positive and 232 were RF-negative at baseline. There were 177 patients negative for both anti-CCP and RF, and 574 patients were positive for both. Baseline characteristics are shown in Table 1, stratified by anti-CCP positivity. In general, anti-CCP–positive patients had more traditional risk factors for CVD, including positive smoking status and higher cholesterol levels, and the majority was male. However, systolic blood pressure and family history of CVD did not differ between the groups, and neither did the DAS28 score, which was similar between the groups. Anti-CCP–negative patients more often started treatment with a DMARD other than methotrexate or sulfasalazine, and more often had a glucocorticosteroids injection at start. During followup, with a median (interquartile range) of 7.5 (4–13) years, 162 CV events were observed (101 IHD, 45 CVA, and 16 PAD), of which 15 were fatal. The amount of disease activity over time, as reflected by the mean (SD) time-averaged DAS28, did not appear to be different (p = 0.73) between anti-CCP–positive and anti-CCP–negative patients [3.7 (1.2) and 3.8 (1.1), respectively]. Baseline DAS28 also was not different between the groups (Table 1).
Baseline characteristics of patients with rheumatoid arthritis overall and specified for anti-CCP status. Values are n (%) unless otherwise specified.
Anti-CCP and the risk of CVD
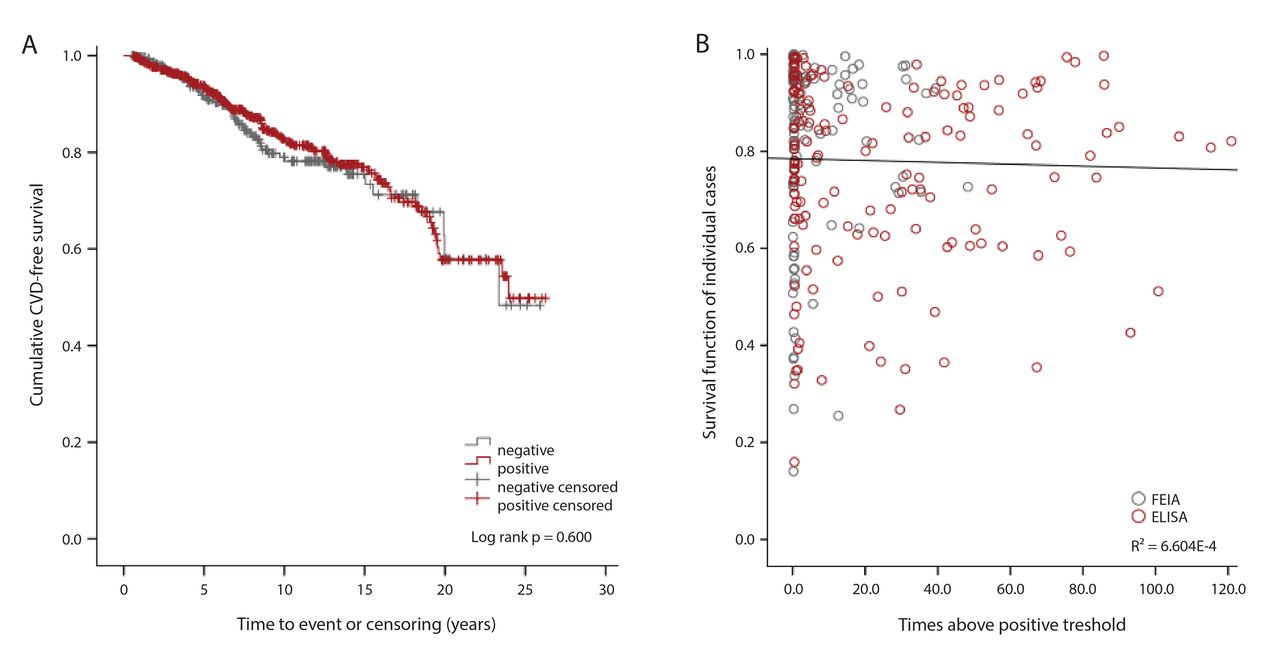
In the anti-CCP–positive group, 112 patients (cumulative proportion at 10 yrs 18%) experienced a CV event in 5828 patient-years compared with 50 (cumulative proportion at 10 yrs 22%) in 2457 patient-years in the anti-CCP–negative group. Applying the Cox regression model, this resulted in a crude HR of 0.91 (95% CI 0.66–1.28), illustrated by a similar cumulative CVD-free survival of anti-CCP–positive and –negative patients in Figure 1A. After adjustment for sex, age, smoking, body mass index, TC/high-density lipoprotein ratio, diabetes, and PtGA and HAQ score, the HR remained insignificant (Table 2). Baseline medication did not act as a confounder in the analysis. Sensitivity analyses showed the robustness of the effects when groups with different age at onset were compared (patients aged < 65 HR 1.09, 0.70–1.72 vs ≥ 65 HR 1.25, 0.90–2.25) or when IHD was used as the outcome variable (HR 1.15, 0.74–1.80).
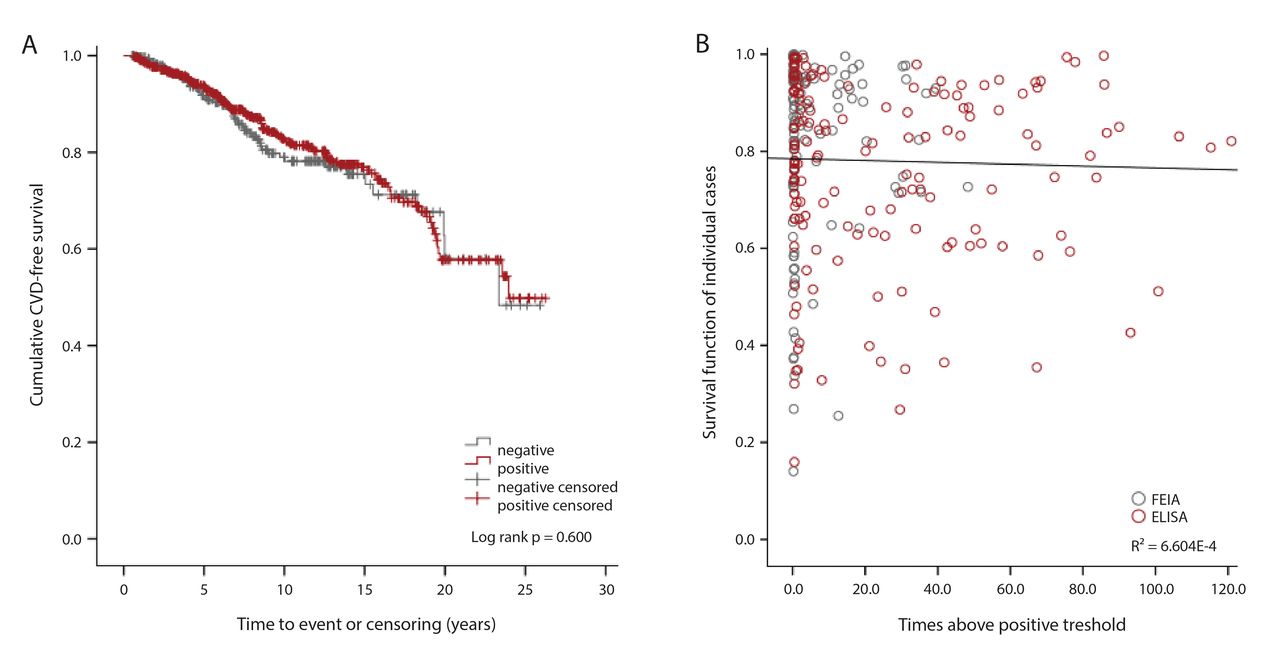
CVD-free survival of patients with RA. (A) Cumulative survival of CVD events in patients with RA. Time to event is depicted on the X-axis. Censored patients are illustrated with vertical lines. (B) Probability of survival for every individual patient, separated by type of assay: FEIA black circles and ELISA red circles. Times above the upper limit of normal are depicted on the X-axis. No effect of anti-CCP status or titer is observed, resulting in a comparable decline of survival (A) and absence of a decline in survival function with increasing anticyclic citrullinated peptide antibodies titers (B). CVD: cardiovascular disease; RA: rheumatoid arthritis; FEIA: fluorescent-enzyme immune-assay.
Effect of anti-CCP positivity, RF positivity, and anti-CCP titer on the risk of cardiovascular disease, and results of the Cox proportional hazards model.
Among the patients with available anti-CCP titers (n = 339), 97 patients (28.6%) experienced a CV event. Anti-CCP titers ranged from 0–120× the ULN (Figure 1B). The crude HR was 0.99 (0.97–1.00). After adjustment for the same confounding variables, the HR remained unchanged (Table 2), as illustrated by an absence of decline in the survival function with increasing anti-CCP titers (Figure 1B). The dots depict the estimated probabilities of 10-year CVD-free survival for each patient.
Anti-CCP, RF, and the risk of CVD
The crude HR of RF on occurrence of CV events was 1.44 (0.96–2.16) and not significant (Table 2). After correction for the same confounders as in the analysis of anti-CCP positivity, the HR of RF was 1.52 (1.00-2.30). In the crude model as well as in the adjusted model (Table 2) of anti-CCP, RF, and their interaction (not shown), it appeared that the effect (HR) of RF was larger than the effect of anti-CCP on CVD, while the interaction term was in a “protective” direction and not statistically significant. To better understand these results, we performed the analysis in subgroups of patients according to their RF and anti-CCP status (negative, positive). As shown in Table 2, the highest HR of RF with CVD was in the anti-CCP–negative patients (HR 2.16, 1.20–3.89, p = 0.010, after adjusting for the same confounders). Similarly, if analyzed in 4 subgroups of patients according to their RF and anti-CCP status, the lowest risk was in the reference group (all HR-positive), with the highest HR for the group that was RF-positive and anti-CCP–negative.
DISCUSSION
According to the results of our study, no association exists between anti-CCP status or titer and CVD-free survival (HR 1.17, 0.82–1.67, and 0.99, 0.98–1.01, respectively) in patients with RA. Rather, there appeared to be an association between RF status and CVD-free survival (HR 1.52, 1.00–2.30) in absence of a statistically significant interaction effect between anti-CCP and RF. Many patients with RA who were RF-positive were also anti-CCP–positive. In combination, it appeared that the CVD risk was lowest in RF-negative, anti-CCP–negative patients, while it was highest in RF-positive, anti-CCP–negative patients.
The results regarding anti-CCP seem in contrast to findings of Hjeltnes, et al14 who showed an association between anti-CCP and endothelial dysfunction, and other studies examining preclinical CV functioning6,15. Similarly, an association of RF, but not of anti-CCP, and endothelial dysfunction in patients with RA was shown by Rojas-Villarraga, et al16. Regarding clinical outcomes, studies that examined the effect on overall CVD, including IHD, CVA, and PAD, supported our findings7,8,9. Ajeganova, et al found an association between anti-CCP status and overall CVD only after subgroup analysis for patients < 65 years at RA onset and stated that absence of an association may reflect an older age group9. In our population, 78% of the patients were aged < 65 at RA onset and the mean age was comparable to studies that do show an association10,11,12, and in our sensitivity analysis HR for patients < 65 years at RA onset was still insignificant, making this explanation unlikely. Studies that do show an association examined the effect of anti-CCP on IHD rather than on overall CVD10,11,12. This could indicate a higher susceptibility of coronary arteries to anti-CCP seropositivity. However, in an additional analysis, we found no significant effect of anti-CCP on IHD (HR 1.15, 0.74–1.80). It is more likely that the described effect of anti-CCP is an artifact of a higher level of disease activity. Studies that found an association, including a recent study in which data from three early RA cohorts were combined13, did not correct for disease severity, e.g., DAS28 score, while the studies that did not find an association with anti-CCP corrected for this and showed that it was an important risk factor for CVD7,8. Our findings are in line with this because in our study the baseline DAS28 score is comparable between the anti-CCP–positive and anti-CCP–negative groups. Despite the lack of association with CVD, it cannot be ruled out that anti-CCP antibodies are contributing to atherosclerosis-associated inflammation in patients with RA. The involvement of RF is similarly unclear because the evidence for an association with CVD is contradictory7,9,10,13,16. The results of large studies on CVD in RA in which both anti-CCP and RF were analyzed, conclude against7,10 as well as in favor13 of an influence of RF and anti-CCP on CVD in RA.
Strengths and limitations of our study
Important strengths of our study are the large sample size, long followup, and adjustment for RA- and CVD-related confounders. In addition, we investigated the influence of anti-CCP titers on 10-year CVD-free survival to overcome the possible drawback of dichotomization. Further, we could study the influence of RF on CVD in the same population and analyses. Another important strength of our study is the use of Cox regression. In this way, we could take time to event into account, in contrast to other studies that used logistic regression.
A limitation of our study is the lack of knowledge about change in variables during followup. All variables were measured at baseline, including the DAS28 score. The time-averaged DAS28 was similar between anti-CCP–positive and –negative patients, but use of variables over time in Cox regression may lead to bias. Further, data on treatment after baseline is lacking, for which Cox proportional hazards modeling allowing for time-variant confounders could be used. Different treatment regimens could have had different effects on CVD prognosis because it has been described that the use of anti-TNF may improve CV prognosis by suppressing systemic inflammation favoring atherosclerosis17. Nevertheless, all patients were usually treated with immune suppressive drugs, and because DMARD failure with higher DAS28 level drives the indication for anti-TNF, it is unlikely that this would have influenced the results. Because we had a large cohort and were able to adjust for a large number of confounding variables, we think it is unlikely that we missed an important existing association between anti-CCP and CVD in patients with RA.
In a large group of patients with RA, we found that neither the presence of anti-CCP antibodies nor their titer at moment of diagnosis associates with 10-year CVD. On the other hand, RF positivity was associated with occurrence of CVD, independently from anti-CCP positivity. This suggests that anti-CCP should not be considered an extra CVD risk factor in RA, irrespective of age at onset of disease. The involvement of RF as a predictive factor for occurrence of CVD in RA is still quite unclear.
- Accepted for publication April 26, 2017.








{kind=link}