
Abstract
Objective. To report efficacy and safety in patients with chronic nonbacterial osteomyelitis (CNO) unresponsive to nonsteroidal antiinflammatory drugs (NSAID) and bisphosphonates and/or glucocorticoids treated with anakinra.
Methods. Nine patients (6 females) with refractory CNO were treated with anakinra for at least 6 months. We recorded, at baseline and after 6 months of treatment, clinical and laboratory features, and number and distribution of bone lesions detected by 99mTc-MDP bone scintigraphy. Disease activity was evaluated using a physician’s global assessment (PGA).
Results. At baseline, 9/9 patients had mild to severe PGA. After 6 months of treatment, in 5 patients the PGA score was graded from none to minimal. At baseline, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were elevated in 8 out of 9 patients. After 6 months, 5/9 patients had normalized CRP and ESR and in all except 1, CRP and ESR decreased. Before starting anakinra, a total of 77 bone lesions were detected by bone scintigraphy. After 6 months of treatment of the 77 lesions, 42 had resolved and 35 were stable. In 7/9 patients, 20 new lesions appeared during treatment; 2 of these 7 patients were symptomatic. At the last followup visit (median 1.7 yrs, range 0.8–2.8), 6/9 patients maintained a PGA graded as none to minimal.
Conclusion. Anakinra is a possible therapeutic alternative in patients with refractory CNO. The practical significance of clinically silent bone lesions detected by bone scintigraphy remains to be established.
- CHRONIC NONBACTERIAL OSTEOMYELITIS
- ANAKINRA
- RESPONSE TO TREATMENT
Chronic nonbacterial osteomyelitis (CNO) is one of the most common autoinflammatory bone disorders in childhood1. It used to be referred to as chronic recurrent multifocal osteomyelitis (CRMO) because bone lesions are often multifocal and with multiple recurrences2. However, a significant number of children have unifocal and uniphasic bone lesions for which the term CNO has been accepted3. The course of the disease is characterized by periodic exacerbations and remissions, but longterm outcome remains unclear. Treatment of CNO is not yet standardized. Several, all uncontrolled, studies have suggested the efficacy of nonsteroidal antiinflammatory drugs (NSAID; until now first-line therapy), glucocorticoids, methotrexate, bisphosphonates, and tumor necrosis factor-α (TNF-α) inhibitors. These drugs are variably used4 with variable degrees of response1,5,6,7,8,9. After treatment, many subjects show no disease activity and no sequelae, but a variable and substantial number of patients have persistent disease with associated morbidities10,11. Pathological bone fractures are the most frequent complications and often occur in the vertebrae, but also in clavicles and long bones12. Other possible complications are scoliosis, bony overgrowth, leg length discrepancies, and growth failure10. Prolonged use of glucocorticoids may contribute to pathological fractures and growth failure. The etiopathogenesis of CNO remains unclear. Extensive microbiological research has not identified with certainty a causative microorganism. In patients with CNO, chronic inflammation appears to be caused by activation of the innate immune system, leading to an imbalance between proinflammatory [interleukin 6 (IL-6) and TNF-α], and antiinflammatory (IL-10) cytokines1,13. Hofmann, et al reported that in the serum of untreated patients with CNO, levels of IL-6 and TNF-α were elevated, while IL-10 was undetectable14. Scianaro, et al demonstrated an abnormal regulation of the IL-1β axis in patients with CNO leading to increased IL-1β release, as well as to a secondary induction of other cytokines15. In line with the report of Scianaro, et al15, Hofmann, et al reported that CRMO monocytes fail to express IL-10 and IL-19, resulting in enhanced NLRP3 (NLR containing a pyrin domain) inflammasome activation with increased IL-1β release16. Based on the conceivable involvement of IL-1β, blockade of this cytokine has been considered a possible therapeutic approach to CNO. Anecdotal case reports have provided initial information on the possible efficacy of IL-1 inhibition in 1 patient with synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome17 (SAPHO syndrome), in 2 patients with Majeed syndrome18, and in 1 patient with CRMO6. In our report, we present data of 9 patients with CNO unresponsive to NSAID and bisphosphonates and/or glucocorticoids who were treated with the recombinant human IL-1 receptor antagonist anakinra.
MATERIALS AND METHODS
We analyzed retrospectively 9 patients with refractory CNO treated with anakinra for at least 6 months. The diagnosis was based on the clinical presentation and on the features and distribution of the bone lesions detected by imaging studies. In 7 patients, the diagnosis was confirmed by histological analysis of bone biopsies and by the absence of microbiological isolates from bone tissue. In 2 patients, the biopsy was deemed unnecessary because of the typical radiological features of the bone lesions. All patients met the criteria proposed by Jansson, et al for a diagnosis of CNO12.
Demographics, clinical, and laboratory data were collected from the Division of Rheumatology clinical database at baseline and after 6 months of treatment with anakinra. We recorded, at baseline and after 6 months, presence of fever, bone pain, functional impairment, inflammatory markers [C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)], and number and distribution of bone lesions detected by 99mTc-MDP bone scintigraphy.
To evaluate disease activity, we used a physician’s global assessment (PGA), a 5-point scoring system (inactive, minimal, mild, moderate, severe disease) based on fever, number of active bone lesions detected by bone scintigraphy, increase of inflammatory markers, and presence of pain and functional impairment, as described in Table 1. Normal ranges used for laboratory data were as follows: CRP < 0.5 mg/dl and ESR < 15 mm/h. Fever because of intercurrent infections was excluded as a criterion for disease activity.
PGA scoring system to evaluate disease activity based on fever, no. active bone lesions detected by bone scintigraphy, increase of inflammatory markers, and presence of pain and functional impairment. Total score: 0 = inactive, 1 = minimal, 2 = mild, 3 = moderate, and 4 = severe.
The study was performed after approval from the ethics committee of the “Ospedale Pediatrico Bambino Gesù” with the ethics approval number 1181/2016. Signed informed consent was obtained from the patients’ parents and from adolescent patients.
Statistical analysis
Statistical analysis was performed using the Graph Pad Prism 5 software. Quantitative data were presented as median and interquartile range (IQR), and categorical data as absolute numbers and percentages. Proportions were compared using Fisher’s exact test, and p value < 0.05 was considered significant.
RESULTS
The demographic and baseline characteristics of patients are shown in Table 2. We evaluated 9 patients (6 females) with a median age at disease onset of 9.2 years (IQR 9.1–14.8). The observation period during anakinra treatment was from April 2013 to August 2015. All patients showed unsatisfactory response after treatment with NSAID and bisphosphonates with or without systemic glucocorticoids. Median disease duration at anakinra treatment start was 11 months (IQR 8–31.8). Anakinra was used at a median dose of 2 mg/kg/day (IQR 2.0–2.3).
Demographics and baseline characteristics of the 9 patients. Values are n (%) or median (interquartile range).
At baseline, 9 out of 9 patients had mild to severe disease activity as shown by PGA, with only 1 patient showing mild disease activity. This patient (patient 3) had received, before baseline, oral glucocorticoids with unsatisfactory response (i.e., increased pain, low grade fever, and increased number of bone lesions at imaging), and his ESR and CRP were normal. After 6 months of treatment, in 5 patients the PGA score was graded from none to minimal (p = 0.03 vs baseline PGA; Figure 1A). At baseline, 4/9 patients had fever, 9/9 patients had pain, and 4/9 had functional impairment. After 6 months of treatment, only 1 patient had fever, 3/9 patients had pain, and none had functional impairment (p > 0.1 for fever, p = 0.009 for pain, and p = 0.08 for functional impairment). At baseline, ESR and CRP were elevated above the upper limit of normal in all patients, except in 1 who received anakinra after 2 months of oral glucocorticoids with unsatisfactory response (i.e., increased pain, low grade fever, and increased number of bone lesions at imaging). After 6 months, 5/9 patients have normalized ESR and CRP (Figure 1B and Figure 1C) and in all except 1, ESR and CRP decreased. Information concerning associated disease, previous and concomitant therapies, fever, PGA score, and number and distribution of bone lesions at baseline bone scintigraphy and whole-body magnetic resonance imaging (WB-MRI) are shown in Table 3.
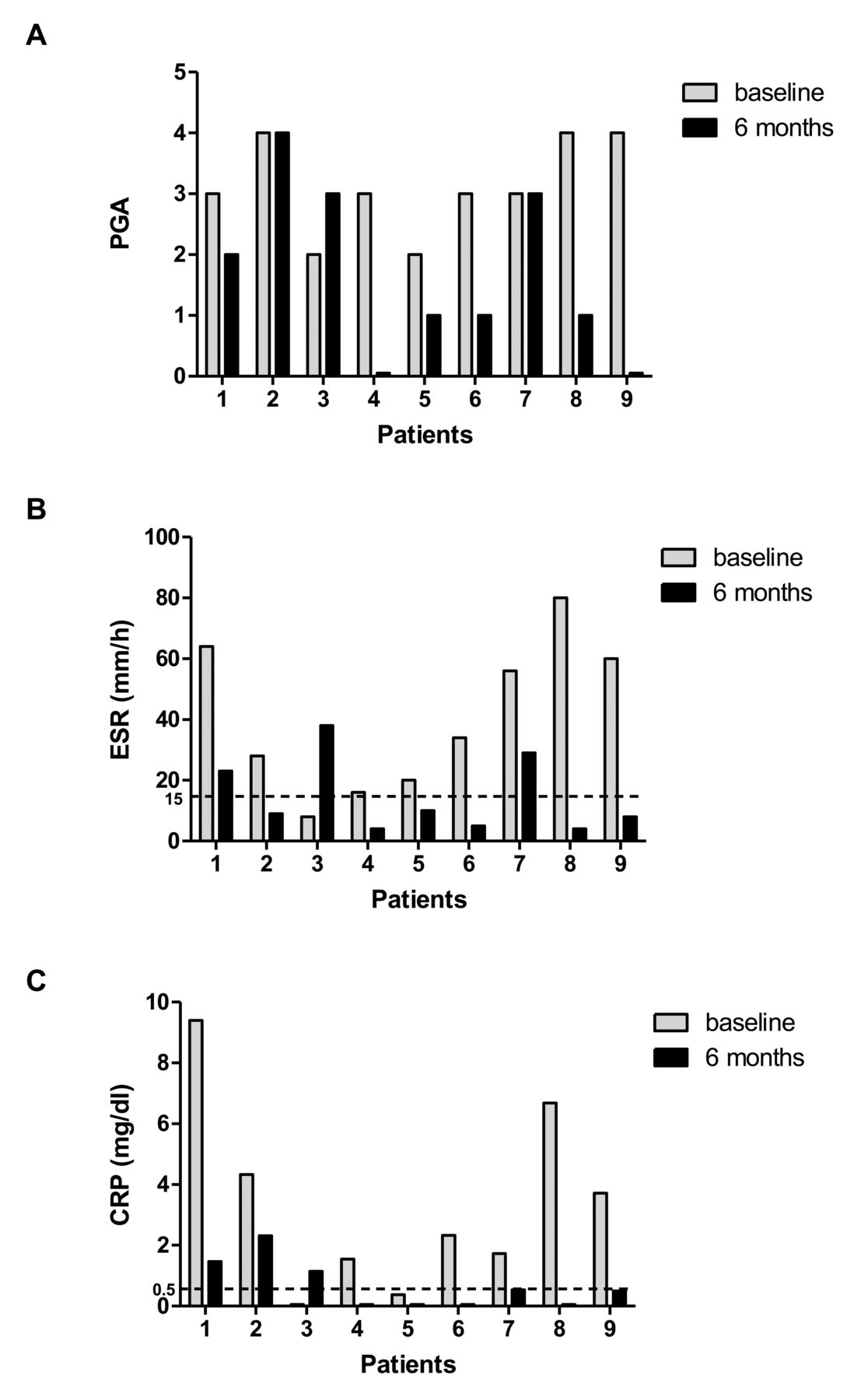
(A) PGA at baseline and after 6 months of treatment with anakinra. (B and C) Inflammatory markers at baseline and after 6 months of treatment with anakinra. PGA: physician’s global assessment; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein.
Associated disease, previous and concomitant therapies, fever, PGA at baseline and after 6 months, and no. and distribution of bone lesions at baseline bone scintigraphy and at WB-MRI.
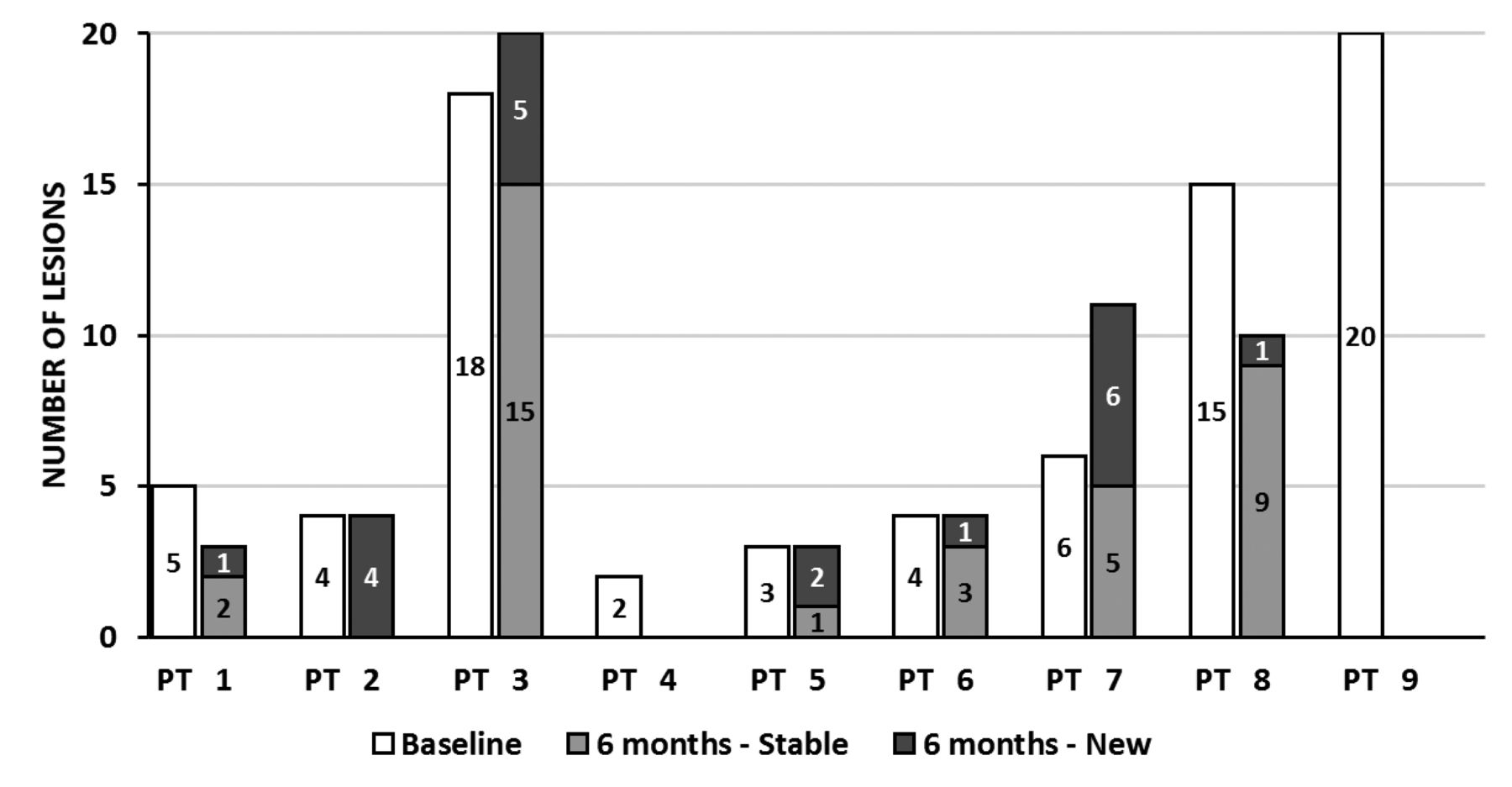
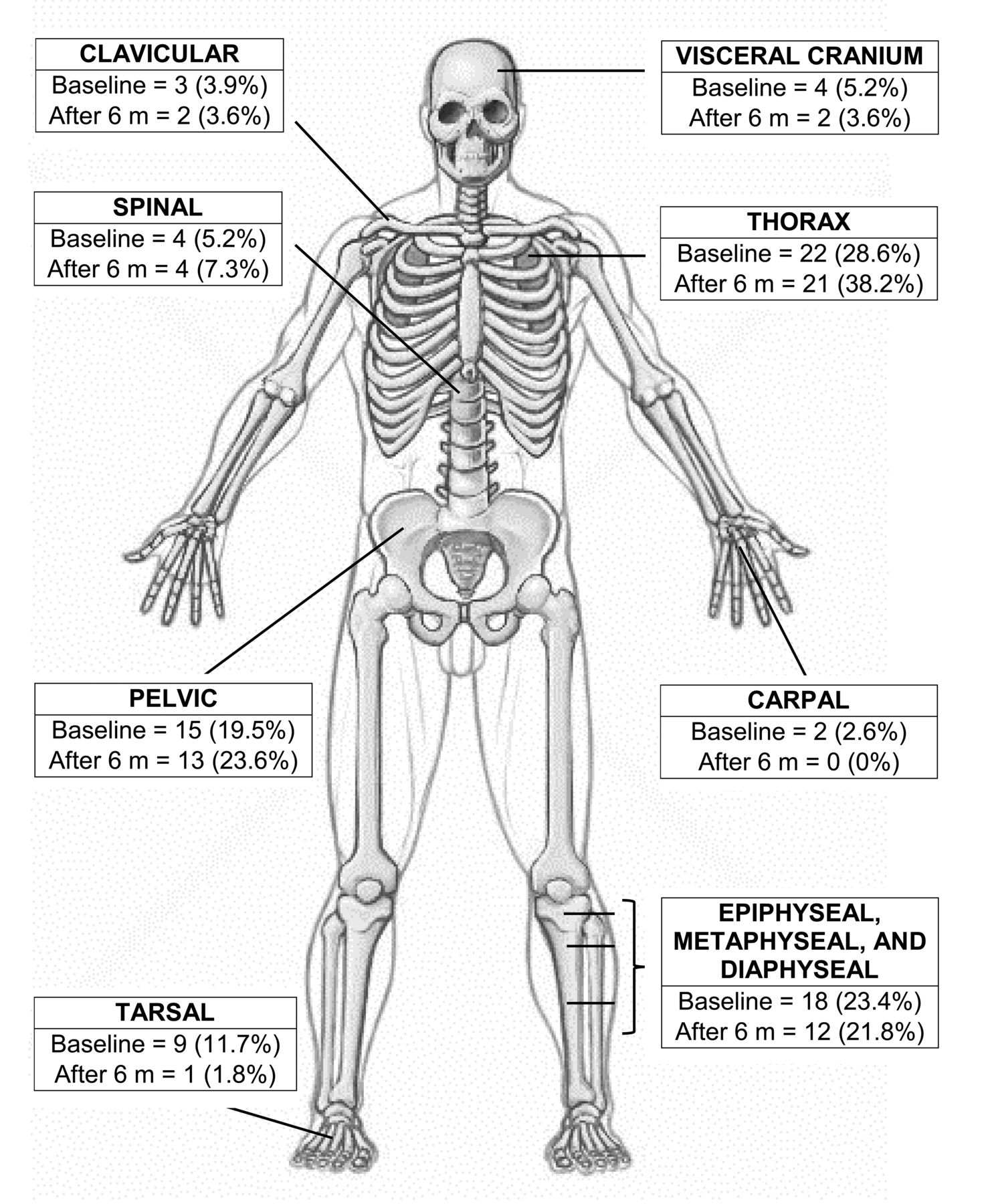
Before starting anakinra, a total of 77 bone lesions in the 9 patients were detected by bone scintigraphy with the distribution shown in Figure 2. After 6 months of treatment, we observed a total of 55 bone lesions, in particular in visceral cranium, carpal, long bones, and tarsal sites. Forty-two out of 77 lesions detected at baseline by bone scintigraphy had resolved while 35 remained stable. In 7 of the 9 patients, 20 new lesions appeared during treatment (Figure 3). Appearance of new bone lesions was particularly evident in 2 patients. Patient 3, an 11-year-old female, had a 2-year history of fever, musculoskeletal pain, functional impairment, elevation of inflammatory markers, and 18 bone lesions with a D9 vertebral crash fracture. Patient 7, a 9-year-old female, had a history of persistent polyarthralgia associated with elevation of inflammatory markers and increased uptake in the right scapulohumeral joint, pelvis, left femur, and the D9 vertebra. After 6 months of treatment with anakinra, both patients showed clear evidence of lack of response with PGA (changing from 2 to 3 in patient 3 and remaining stable at 3 in patient 7), persistently elevated ESR and CRP, and increase in the number of bone lesions by bone scintigraphy in both patients. Anakinra was withdrawn and both were switched to etanercept (ETN). Bone lesions resolved completely in 2 patients: patient 4, a 5-year-old male with isolated bilateral involvement of the mandible, and patient 9, an 18-year-old female with history of fever and pain, elevation of inflammatory markers, and 20 active bone lesions at baseline.

Bone involvement detected by bone scintigraphy at baseline (n = 77) and after 6 months of treatment (n = 55).
{kind=link}
{kind=link}
{kind=link}
Number of active bone lesions detected by bone scintigraphy for each patient at baseline and after 6 months of treatment with anakinra. PT: patient.
At the last visit (median followup duration after anakinra treatment was 1.7 yrs, range 0.8–2.8), 6 out of 9 patients maintained a PGA graded as none to minimal. Of these 6 patients, 4 are continuing anakinra in monotherapy, 1 switched to ETN for lack of efficacy, and 1 was lost at followup. Two out of the 3 patients receiving glucocorticoids at baseline were able, during anakinra treatment, to withdraw glucocorticoids after progressive tapering over 8 weeks. One patient (patient 4) was able to withdraw glucocorticoids after 9 months of treatment. No serious adverse events were recorded in these 9 patients and no cases of severe injection site reactions were reported.
DISCUSSION
In our study, we report a single-center experience with the use of anakinra in recalcitrant CNO following unsatisfactory response to NSAID and bisphosphonates with or without glucocorticoids. To date, there are neither randomized controlled trials nor therapeutic recommendations for treatment of patients with CNO19. Further, the course of the disease is “waxing and waning,” making it difficult to evaluate response to all treatments used in CNO. The treatment strategy of CNO unresponsive to NSAID and bisphosphonates with or without glucocorticoids remains undefined. In a recent review, it is reported that in many European centers, patients with resistant CNO are treated with TNF inhibitors20. However, no studies are available describing efficacy data, although this treatment has also been suggested by other authors6,21,22.
Other studies demonstrate an involvement of the IL-1 pathway in the pathogenesis of the CNO in a murine model23,24. Scianaro, et al showed increased IL-1β secretion by peripheral blood mononuclear cells of patients with CNO during active disease15. These and other observations support the inclusion of CNO in the group of the autoinflammatory diseases.
We evaluated response to anakinra based on clinical features, acute-phase reactants, and number of bone lesions detected by bone scintigraphy. Of note, standardized measurements of disease activity and/or validated composite clinical scores for CNO are not available. Beck, et al5 have proposed a PedCNO score, composed of 5 measures: ESR, number of radiological lesions, severity of disease estimated by the physician, severity of disease estimated by the patient or parent, and the Childhood Health Assessment Questionnaire. This score has not been used in other publications. We decided to assess clinical disease activity using a PGA 5-point scoring system, as is used in other systemic diseases (e.g., psoriasis and Crohn disease)25,26.
After 6 months of treatment, in 6 out of 9 patients the PGA score was graded from none to mild and was maintained after a median duration of followup of 1.7 year. We also observed a decrease in the total number of bone lesions; however, bone inflammation was still detectable by bone scintigraphy after 6 months of treatment with appearance of new lesions in a considerable proportion of patients; these lesions were clinically asymptomatic in the majority of the subjects. In patients with CNO, evaluation of disease activity is difficult because of the unclear correlation between clinical features, inflammatory markers, and radiological findings. The clinical significance of silent bone lesions detected by bone scintigraphy in the followup is unclear. Indeed, Voit, et al27, by using WB-MRI, evaluated the presence of bone lesions in 17 symptom-free patients with CNO who had disease at least 10 years before WB-MRI. They found that 45% of these patients had radiologically active lesions and that the number of lesions in patients in clinical remission was markedly higher than clinically suspected. These results are in agreement with the observations of Fritz, et al, who reported that 68 of 101 bone lesions (67%) detected by WB-MRI in 13 patients with CNO were not symptomatic28. In a retrospective review, Guérin-Pfyffer, et al described 9 patients with CNO studied with WB-MRI that showed 28 bone localizations, several of them asymptomatic29.
A limitation of our study is the use of bone scintigraphy alone to detect bone lesions, both at baseline and during the followup. WB-MRI is progressively being used as an imaging methodology to monitor disease activity and response to therapy in CNO because it is noninvasive, does not imply use of radioactivity, and takes a relatively short time5,28,29. However, younger children require sedation. Moreover, the available data, which are scanty, do not provide definitive conclusions. In some studies, WB-MRI seems to be more sensitive than bone scintigraphy in the detection of signs of acute and chronic inflammation (edema and sclerosis) in bones and in the adjacent soft tissues30. Guérin-Pfyffer, et al reported that WB-MRI, compared to bone scintigraphy, may not be as efficient in detecting inflammation in specific sites (e.g., sternoclavicular or costovertebral joints) that are often involved in CNO29. Morbach, et al suggested that WB-MRI may be particularly useful in evaluating the extent of inflammatory lesions, particularly for symmetrical lesions of long bones. Even more importantly, the clinical significance of inflammatory bone lesion detected by WB-MRI, but metabolically inactive by bone scintigraphy, remains controversial31. Therefore, the involvement of 1 methodology versus the other in CNO diagnosis and management remains controversial. In addition, in our study, baseline and followup WB-MRI data are available only in 4 of the 9 patients (patients 3, 6, 8, and 9); in these patients, we did not find significant differences in the number and distribution of bone lesions between the 2 techniques. Such a small number does not allow a proper comparison or to draw conclusions. The other limitations of our study are the small number of patients and its uncontrolled and retrospective design. It should also be taken into account that the penetration of anakinra in bone tissue is unknown. Indeed, the optimal dosing regimen in CNO is far from having been defined.
Our results suggest a possible therapeutic alternative in patients with CNO refractory to treatment with NSAID and bisphosphonates with or without glucocorticoids. Five out of 9 patients showed a favorable clinical outcome in the first 6 months of treatment with anakinra. At present, comparison with the efficacy of TNF inhibitors is not possible based on the available published data. Further studies in CNO, ideally including randomized controlled trials, are desirable. In the absence of controlled data and based only on retrospective series, the treatment choice should be left to the experience of the treating physicians. The clinical significance of silent bone lesions detected by bone scintigraphy (or in other settings by WB-MRI) remains to be established, possibly through larger multicenter studies with shared imaging protocols.
- Accepted for publication April 20, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.