
Abstract
Objective. There is increasing evidence that early therapeutic intervention improves longterm joint outcome in juvenile idiopathic arthritis (JIA). Given the existence of highly effective treatments, there is an urgent need for reliable and accurate measures of disease activity and joint damage in JIA. Our objective was to assess the reliability of 2 magnetic resonance imaging (MRI) scoring methods: the Juvenile Arthritis MRI Scoring (JAMRIS) system and the International Prophylaxis Study Group (IPSG) consensus score, for evaluating disease status of the knee in patients with JIA.
Methods. Four international readers independently scored an MRI dataset of 25 JIA patients with clinical knee involvement. Synovial thickening, joint effusion, bone marrow changes, cartilage lesions, bone erosions, and subchondral cysts were scored using the JAMRIS and IPSG systems. Further, synovial enhancement, infrapatellar fat pad heterogeneity, tendinopathy, and enthesopathy were scored. Interreader reliability was analyzed by using the generalized κ, ICC, and the smallest detectable difference (SDD).
Results. ICC regarding interreader reliability ranged from 0.33 (95% CI 0.12–0.52, SDD = 0.29) for enthesopathy up to 0.95 (95% CI 0.92–0.97, SDD = 3.19) for synovial thickening. Good interreader reliability was found concerning joint effusion (ICC 0.93, 95% CI 0.89–0.95, SDD = 0.51), synovial enhancement (ICC 0.90, 95% CI 0.85–0.94, SDD = 9.85), and bone marrow changes (ICC 0.87, 95% CI 0.80–0.92, SDD = 10.94). Moderate to substantial reliability was found concerning cartilage lesions and bone erosions (ICC 0.55–0.72, SDD 1.41–13.65).
Conclusion. The preliminary results are promising for most of the scored JAMRIS and IPSG items. However, further refinement of the scoring system is warranted for unsatisfactorily reliable items such as bone erosions, cartilage lesions, and enthesopathy.
- JUVENILE IDIOPATHIC ARTHRITIS
- MAGNETIC RESONANCE IMAGING
- OUTCOMES
- REPRODUCIBILITY OF RESULTS
- KNEE JOINT
Persistent synovitis can lead to osteochondral abnormalities that are responsible for disability and impaired quality of life in patients with juvenile idiopathic arthritis (JIA)1,2,3,4. The main goal of treatment in JIA is the complete suppression of joint inflammation. Therefore, outcome measures in daily practice and clinical trials must include sensitive and reliable measures of disease activity5.
Magnetic resonance imaging (MRI) holds potential to become an important outcome measure for assessment of joints in patients with JIA5,6. Although MRI is the preferred imaging modality for detection of synovial inflammation, and early destructive bone changes in JIA7,8,9, experiences on the use of MRI for assessing JIA is limited. Consequently, this method is underused in both clinical practice and research. One of the most important causes for underuse of MRI for assessment of JIA is the absence of standardized protocols and scales for data acquisition and interpretation5,6,10. The use of such protocols and scales by different centers across the globe is crucial for meaningful and comparable results acquired in multicenter clinical trials.
Over the years, different MRI scoring methods have been developed for assessment of joints. Two of them focus on the assessment of large pediatric joints. The Juvenile Arthritis MRI Scoring (JAMRIS) system11 focuses on JIA and the International Prophylaxis Study Group (IPSG) MRI Scoring system12 focuses on hemophilic arthropathy. Both the JAMRIS and IPSG systems consist of 2 domains: 1 soft tissue and 1 osteochondral (bone and cartilage items). Whereas the soft tissue domain of the JAMRIS system consists of synovial hypertrophy, the soft tissue domain of the IPSG system consists of synovial hypertrophy and joint effusion. In the JAMRIS system, the bone items include bone marrow edema (BME), bone erosions, and cartilage lesions/loss. In the IPSG system, the bone item includes bone erosions, subchondral cysts, and cartilage loss. Subchondral cysts are items of the IPSG MRI system, but not of the JAMRIS system. Nevertheless, whereas in the JAMRIS system the final score for each item represents the sum of maximum scores in pre-established sites of the knee, in the IPSG system the final score for each item represents the maximum score of any area of the knee without summing up scores of regions.
Regardless of their conceptual methodological differences, both scoring methods are limited because they are not internationally validated for the evaluation of disease activity in JIA6. Prior to the Outcome Measures in Rheumatology (OMERACT) 11 meeting, a Special Interest Group (SIG) was formed focusing on MRI in JIA. One of the aims of this SIG was to standardize and develop an MRI outcome measure to objectively assess disease activity, including large joints such as the knee10. To develop a unique consensus, MRI scale for the assessment of large pediatric joints, we used items from existing MRI scales and assessed the reliability of the aforementioned MRI scoring systems. Therefore, the objective of our study was to assess the reliability of the JAMRIS and the IPSG scoring systems for evaluating disease activity and osteochondral changes in JIA of the knee.
MATERIALS AND METHODS
Design and patients
To evaluate the interobserver reliability of the JAMRIS and IPSG systems, 4 readers independently scored MRI datasets of 25 JIA patients with current or previous knee involvement attending the pediatric rheumatology clinic of 2 tertiary centers from 2011 to 2014 (Academic Medical Center, Amsterdam, the Netherlands, and the Hospital for Sick Children, Toronto, Ontario, Canada). Contrast-enhanced MRI were selected from examinations of clinically active patients with JIA obtained in Amsterdam, the Netherlands (n = 20) and Toronto, Ontario, Canada (n = 5). Readers consisted of 1 musculoskeletal radiologist (MM, 19 yrs of experience), 1 pediatric radiologist (ASD, 11 yrs of experience), 1 pediatric rheumatologist (NT, 9 yrs of experience), and 1 radiology trainee (RH, 6 yrs of experience). All readers were blinded to clinical history.
Patients fulfilled the International League of Associations for Rheumatology criteria for JIA13. Institutional Review Board approval was granted for the current study, with informed consent being waived in both centers [Academic Medical Center (NL41846.018.12), Hospital for Sick Children (10000422167)]. The study was performed in accordance with the Declaration of Helsinki.
MRI protocol
The MRI sequences acquired in Amsterdam were obtained using an open-bore 1.0T magnet (Panorama HFO, Philips Medical Systems) and those derived from Toronto were obtained using a standard 1.5T magnet (Avanto-Fit, Siemens Healthcare). The nonsedated children were placed in the supine position with the knee joint lying centrally in the magnetic field in a dedicated knee coil (16 channel and 8 channel knee coil in Amsterdam and Toronto, respectively).
Sequences included sagittal T2-weighted fat-saturated images, coronal T2-weighted fat-saturated images, axial T2-weighted fat-saturated images, sagittal T1-weighted (obtained in Amsterdam), and sagittal proton-density (obtained in Toronto), and sagittal and axial T1-weighted fat-saturated images obtained after intravenous (IV) contrast injection (obtained in both centers). Postcontrast axial images were obtained in the early phase (< 5 min) after IV injection of gadolinium. Additional sagittal 3-D double-echo steady state images of the knee were obtained in Toronto for cartilage assessment.
MRI scoring system
MRI datasets were scored by using the JAMRIS and the IPSG systems, complemented with 4 additional MRI features: infrapatellar fat pad heterogeneity, enthesopathy, tendinopathy, and synovial enhancement. The rationale for including these additional features in our analysis was to determine the effect of them on the reliability of the scales. A prior study has assessed the value of these features in the content validity of the JAMRIS system14.
An easy-to-use scoring form is depicted in the Supplementary Data (available with the online version of this article).
The JAMRIS system
The JAMRIS scoring method has been described before in detail12. Briefly, synovial thickening was scored when thickness of the contrast-enhanced synovial membrane was ≥ 2 mm. Synovial thickening was scored at 6 locations. The maximal thickness of any slice at each site was graded as follows: grade 0 = < 2 mm, grade 1 = ≥ 2–4 mm, and grade 2 = > 4 mm, resulting in a minimum score of 0 and a maximum of 12.
Bone marrow changes, cartilage lesions, and bone erosions were scored at 8 locations. BME was scored semiquantitatively based on the subjectively estimated percentage of involved bone volume at each site as follows: grade 0 = none, grade 1 = < 10%, grade 2 = ≥ 10–25%, and grade 3 = > 25% of the whole bone volume or of the region of the cartilage surface area, resulting in a minimum score of 0 and a maximum of 24.
MRI definitions of BME, cartilage lesions, and bone erosions were previously described12. For example, a bone erosion was defined as a sharply marginated bone lesion with correct juxtaarticular localization, typical signal characteristics, and visible in 2 planes with a cortical break in at least 1 plane. On T1-weighted images, there is a loss of the normal low signal intensity of cortical bone and loss of the normal high signal intensity of trabecular bone.
The IPSG scoring system
The IPSG score has been developed and validated for use in hemophilic arthritis and described before11,15. Briefly, synovial thickening was scored when thickness of the contrast-enhanced synovial membrane was > 1 mm. In the IPSG score, the location with the maximal score does count16. Synovial thickening was graded semiquantitatively as follows: grade 0 = none, grade 1 (mild) = > 2–3 mm, grade 2 (moderate) = > 3–5 mm, and grade 3 (severe) = > 5 mm.
Joint effusion was scored when the maximal diameter of the largest pocket was ≥ 3 mm as previously described16.
Erosions and subchondral cysts were graded semiquantitatively according to the area involved. Bone erosions were scored by evaluating the presence of any surface erosion. For bone erosions, 1 score was given for any surface erosion, and 1 score was given for half or more of the articular surface eroded in at least 1 bone, yielding a maximum of 2. The presence of subchondral cysts was scored when there was at least 1 subchondral cyst anywhere in the knee. For subchondral cysts, 1 score was given for at least 1 subchondral cyst, and 1 score was given for subchondral cysts in at least 2 bones, yielding a maximum of 2. Cartilage lesions/loss were scored by evaluating the presence of any loss of the normal cartilage. Normal values for cartilage thickness in healthy children was used for the evaluation of cartilage thinning17. For cartilage loss, 1 score was given for any cartilage damage, 1 score was given for loss of half or more of the total volume of joint cartilage in at least 1 bone, 1 score was given for full thickness loss of joint cartilage in at least some area in at least 1 bone, and 1 score was given for full thickness loss of joint cartilage including at least 1 half of the joint surface in at least 1 bone yielding a maximum of 4 scores per joint. MRI definitions of bone erosions, subchondral cysts, and cartilage loss were previously described16.
Additional MRI features
Four additional MRI features were scored as well, including synovial enhancement, infrapatellar fat pad heterogeneity, enthesopathy, and tendinopathy.
The degree of synovial enhancement was scored per JAMRIS region as described by Damasio, et al18 as follows: 0 = normal synovial enhancement as compared to neighboring muscle, 1 = mildly increased synovial enhancement, and 2 = moderately to severely increased synovial enhancement.
The infrapatellar fat pad was scored for heterogeneity (0 = absent, 1 = present) being caused by water infiltration or by scar tissue14.
Tendinopathy of enthesopathy of the patellar and quadriceps tendons were assessed for increased signal intensity on T2-weighted images within the tendon or the enthesis, respectively (0 = absent, 1 = present).
Statistics
Descriptive statistics were calculated for each reader. Reliability was comprehensively evaluated with 3 statistical methods. The average measure ICC was classified as follows: ICC < 0.40 = poor, ≥ 0.40–0.60 = moderate, > 0.60–0.80 = substantial, and > 0.80 = excellent reliability19. Second, the smallest detectable difference (SDD) was assessed deriving from the limits of agreement method. The SDD was calculated for all the summated scores using the residual error variance from repeated measures ANOVA20,21. Moreover, the SDD was calculated as a percentage of the highest score reached. For categorical data, the generalized κ statistics were used and classified as follows: κ < 0.20 = poor, > 0.20–0.40 = fair, > 0.40–0.60 = moderate, > 0.60–0.80 = substantial, and > 0.80 = excellent reliability.
RESULTS
Patients
In our reliability study, MRI datasets of 25 patients with JIA were scored (60% women; mean age 12.3 yrs, SD 2.7; mean disease duration 5.6 yrs, SD 4.8). Frequencies of JIA subtypes were as follows: 8/25 (32%) persistent oligoarthritis, 4/25 (16%) extended oligoarthritis, 8/25 (32%) polyarthritis, 2/25 (8%) psoriatic arthritis (PsA), and 3/25 (12%) enthesitis-related arthritis. Of these patients, 4 (16%) were clinically inactive, while 21 (84%) had clinically active disease activity.
Reliability study
Descriptive statistics (mean, minimum and maximum scores) per reader of the different item scores are shown in Table 1.
Descriptive statistics per reader of the different items scored from 25 juvenile idiopathic arthritis patients with MRI of the knee. Values are mean (interquartile range) unless otherwise specified.
Interreader reliability concerning MRI features focusing on disease activity was excellent for all scores (ICC 0.87–0.95; Table 2). Synovial thickening according to the JAMRIS and IPSG scores were ICC 0.95 (SDD 3.19) and 0.94 (SDD 0.39), respectively. Synovial enhancement was ICC 0.90 (SDD 9.85), joint effusion was ICC 0.93 (SDD 0.51), and bone marrow changes was ICC 0.87 (SDD 10.94). An example of synovial thickening with a good agreement between readers is depicted in Figure 1, whereas Figure 2 illustrates a case with good agreement on the scoring of joint effusion.
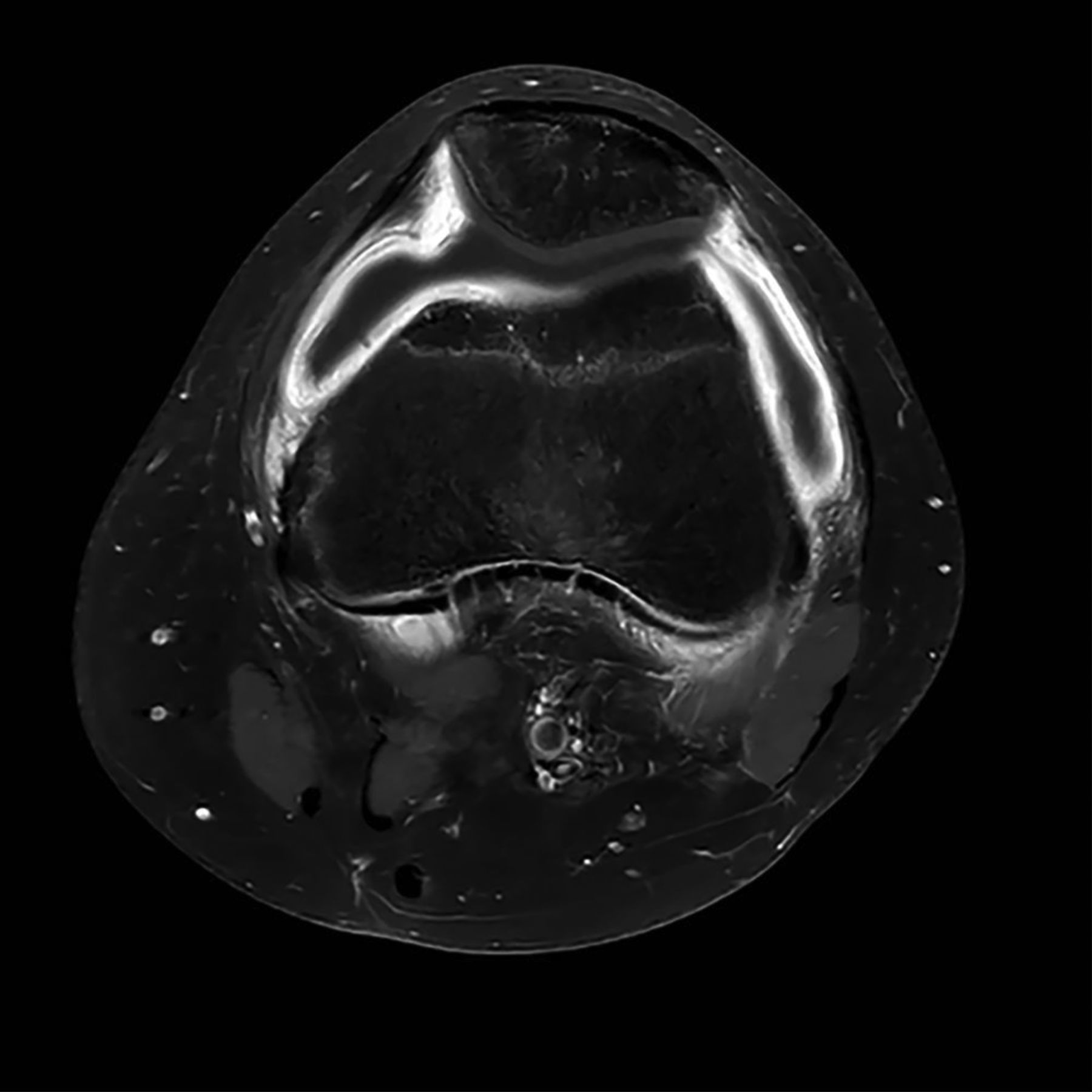
Synovial thickening. Axial fat-saturated contrast-enhanced T1-weighted image obtained in a 12-year-old girl showing retropatellar and parapatellar synovial thickening.
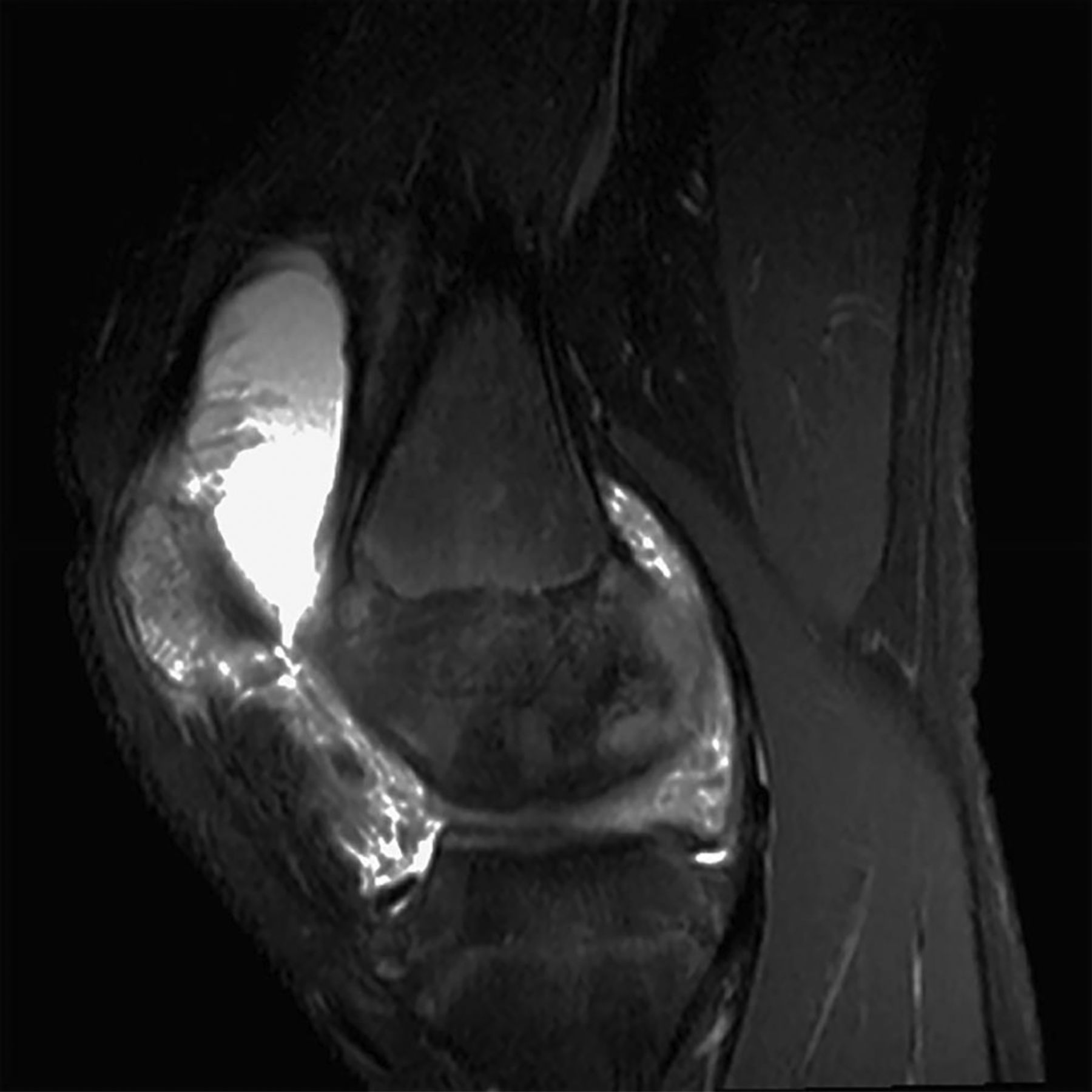
Joint effusion. Sagittal fat-saturated T2-weighted image obtained in a 14-year-old girl showing extensive joint effusion in the suprapatellar recess.
Generalized κ, ICC, and SDD statistics of the different items scored from 25 juvenile idiopathic arthritis patients with MRI of the knee.
Interreader reliability for the MRI features focusing on destructive joint changes was moderate to substantial (ICC 0.55–0.72; Table 2). Assessment of cartilage lesions according to the JAMRIS and ISPG scores demonstrated ICC 0.55 (SDD 13.65) and 0.60 (SDD 8.30), respectively. Evaluation of bone erosions according to the JAMRIS and ISPG scores showed ICC 0.72 (SDD 1.41) and 0.57 (SDD 4.10), respectively. Figure 3 depicts an example of a bone erosion that was not scored by all readers. The generalized κ of subchondral cysts according to the IPSG score was poor (κ = 0.01).

{kind=link}
{kind=link}
{kind=link}
Bone erosion. Sagittal T1-weighted postcontrast magnetic resonance image obtained in a 17-year-old girl with clinically active juvenile idiopathic arthritis shows a bone erosion in the tibial plateau with loss of normal high signal intensity of the trabecular bone and irregular cortical outlines.
Generalized κ concerning the additional scored MRI features (infrapatellar fat pad heterogeneity, enthesopathy, and tendinopathy) were relatively poor (range 0.01–0.27; Table 2).
DISCUSSION
In our study, we assessed the interreader agreement of the JAMRIS and the IPSG scoring systems for evaluating disease activity of the knee in patients with JIA. Overall the interreader reliability was excellent for MRI scores focusing on active disease (e.g., synovial hypertrophy, effusion, and bone marrow changes). Interreader reliability focusing on osteochondral changes (e.g., cartilage lesions, bone erosions) was moderate to substantial.
Out of 2 MRI scales designed to assess morphologic changes of the knee in pediatric patients11,12, the JAMRIS system was purposely developed for the use in JIA and the IPSG scoring system for the use in hemophilic arthritis. Although the pathophysiology, clinical presentation, and genetic background of hemophilic arthritis differ from those of JIA, there is a considerable structural overlap of MRI characteristics of affected joints that may present with (reactive) synovial hypertrophy, bone marrow changes, and destruction of cartilage and bone. In our current study, we were intentionally broadly inclusive of scoring items that could identify a wide range of MRI features in these 2 types of arthritis. Therefore, items of each score were assessed independently. The scoring methods used have some conceptual methodological differences. For example, in the JAMRIS system, the final score for each item represents the sum of maximum scores in preestablished sites of the knee, and in the IPSG system, the final score for each item represents the maximum score of any area of the knee without summing up scores of regions. By doing so, the JAMRIS system has a significantly wider range of score compared with the method used in the IPSG score, making the JAMRIS system, in all probability, more sensitive to change compared with the IPSG method. On the other hand, a simpler score with a lower range of score (such as the IPSG method) could be more reliable when focusing on less common abnormalities. The sensitivity to change over time of the methods used should be evaluated in future studies.
Although abnormalities of the infrapatellar fat pad and tendons might be associated with disease activity in JIA, in our present study, most discrepancies were noted about the assessment of infrapatellar fat pad heterogeneity, enthesopathy, and tendinopathy (κ 0.01–0.27). Therefore, we should consider improving the definitions for characterization of these findings or excluding them from a final score in the future if appropriate.
MRI has some technical limitations for its use in children. Limitations include, among others, the necessity for sedation in young children and the limited number of joints that can be evaluated during 1 imaging session. Moreover, MRI using an IV contrast agent is indispensable for the sensitive differentiation of joint effusion and synovial hypertrophy8. Despite these limitations, MRI is deemed the most sensitive technique for the evaluation of disease status in patients with JIA6. The appropriateness and feasibility of different imaging modalities differs with age. Therefore, the use of ultrasound can be helpful in patients with JIA as well.
Our study has methodological limitations. The most important drawback is the lack of severely affected patients with JIA. The reliability of the JAMRIS and IPSG score has only been tested in patients with JIA visiting referral pediatric rheumatology centers with full access to current treatment. This has resulted in a population of studied patients with only mild to moderate disease activity. Consequently, the presence of destructive changes was relatively low. Additional research is necessary to evaluate the value of a scoring system as a sensitive measure regarding these destructive changes. For further validation of an objective and easy-to-use scoring system, international collaboration is warranted, especially with research centers with access to more severely affected patients with JIA.
Second, there is sparse information about normal MRI values in healthy knees of children at different ages17,22. For example, thinning of the articular cartilage can be either physiologic or pathologic, and bony depressions simulating joint damage are common in wrists of healthy children23. Early joint damage in children with JIA can, therefore, be masked on MRI24. International collaboration is required to solve these challenges in the interpretation of MRI. The development of MRI scores to measure JIA disease activity and joint damage in growing joints can be otherwise seriously limited, which affects the care of children with JIA.
Another limitation is the lack of a specific cartilage-sensitive MRI technique in a great number of examinations. The Amsterdam cohort had only proton-density sequence available for assessment of cartilage. This could have reduced the readers’ ability to identify early cartilage changes. It is well known that proton density–weighted imaging is capable of depicting surface cartilaginous defects as well as abnormalities of internal cartilage composition. Nevertheless, institutions prefer to use intermediate-weighted sequences that combine the contrast advantage of proton density weighting with that of T2 weighting by using a TE of 33–60 ms. These sequences provide higher overall signal intensity in cartilage than standard T2-weighted sequences do, allowing better differentiation between cartilage and subchondral bone. In addition, they are less susceptible to the magic angle effects seen in proton density–weighted imaging with a shorter TE25.
Previous studies have pointed out that with fat-suppressed proton density and T2-weighted fast spin echo sequences, normal hyaline cartilage has intermediate signal intensity, and intraarticular fluid appears bright, thus displaying good contrast because of an “arthrographic” effect that identifies surface abnormalities as well as abnormalities in cartilage matrix26. Proton density-weighted sequences provide greater contrast in the cartilage structure and evaluate the cartilage-synovial fluid interface and the subchondral bone, being previously used for detecting chondral lesions27,28,29.
There was a variance concerning the level of experience and training of the readers, different backgrounds and slightly different MRI protocols for data acquisition; this might have resulted in lower reliability values in the osteochondral domain compared with the Amsterdam reliability studies of the JAMRIS system12. However, our reliability scores of disease activity and osteochondral damage were comparable to the values obtained in reliability studies regarding JIA and rheumatoid arthritis MRI scores of the wrist30,31. On the other hand, with regard to the assessment of joint damage (e.g., cartilage lesions, bone erosions), in our study reliability scores were somewhat lower (ICC 0.55–0.72) than the scores of the wrist in patients with JIA as described by Malattia, et al30 and the patients with PsA as described by the OMERACT SIG in Inflammatory Arthritis31. Our findings are in line with validation exercises focusing on the wrist in patients with JIA, in which it was shown that damage MRI scores can be relatively inaccurate18,32,33,34. Finally, the studied cohort was not consecutive, which may have caused selection bias and had mild osteochondral changes that reduced the generalizability of the results of our study to populations with more severe changes.
Moreover, reliability was evaluated using the ICC in a relatively small number of MRI datasets, and data were considered as continuous. This topic is controversial because some authors consider the variables of scoring systems whose maximum value is above a certain limit (e.g., 10) to be continuous rather than categorical data. Nevertheless, our intention was to compare the results of our study with results from the OMERACT studies conducted in adults that also used ICC and SDD35,36.
To develop and validate an easy-to-use MRI scoring system, further formal expert consensus processes and discrete choice experiments are required to determine the relevance of items of the scale and to refine definitions of items that demonstrated poor interreader reliability in our study. Another question is whether to use the extensive JAMRIS method for the quantification of findings per MRI feature or the more simplified IPSG method in a final future MRI scale. Although an extensive quantification scoring method is relatively more time-consuming, it is probably more accurate as well, especially in depicting small changes over time.
Several advanced MRI techniques are available for the evaluation of inflammatory and destructive changes in JIA, including dynamic contrast–enhanced MRI, T2-mapping, diffusion-weighted MRI, and delayed gadolinium-enhanced MRI of cartilage. Currently, these imaging techniques are used particularly in the context of research and to a lesser extent in daily practice. Moreover, specialized knowledge is needed for the interpretation and postprocessing of these images. To date, advanced imaging techniques are therefore not valuable for use in an easy-to-use scoring method such as the JAMRIS system.
Our preliminary results are promising for most scored JAMRIS and IPSG items for assessment of mild joint changes in JIA. Because interreader reliability, focusing on destructive changes, was moderate to substantial in the studied cohort, further refinement of the scoring system items and definitions are warranted for the next step of development of a single MRI scoring system to assess different stages of disease activity in patients with JIA. With this regard, the concurrent development of an atlas with representative images of different stages of disease activity in JIA can potentially improve the interpretability of the scoring system items.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
- Accepted for publication April 17, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.