

Abstract
Objective. To identify the factors relevant to work and activity impairment in patients with rheumatoid arthritis.
Methods. In total, 1274 consecutive patients were included. Work and activity impairment were measured by the Work Productivity and Activity Impairment questionnaire, and related clinical factors were examined.
Results. Work and activity impairment was reported by 67.4% of the patients. Multivariable linear regression analyses revealed pain and non-remission to be associated with activity impairment and presenteeism. Patients in remission had significantly less activity impairment and presenteeism than those with low disease activity.
Conclusion. Remission achievement is essential for ensuring work performance and activity.
Rheumatoid arthritis (RA) has a profound effect on quality of life and work productivity. The decline in work productivity is especially important because it affects patients’ quality of life, income, and social costs. Many studies have demonstrated that a large proportion of patients with RA experience work impairment1,2,3. About 20%–70% of patients experience work impairment 7–10 years after disease onset2. Work disability among patients with RA is about double that of the general population3.
With the advent of improved therapies, the primary aim of RA treatment is to control the disease and maximize health-related quality of life, thereby allowing patients to participate in social and work activities4. Several factors, such as age, education, disease activity, and functional disability, affect the work performance of patients with RA5,6,7,8,9,10,11. However, only a few studies have analyzed the factors relevant to detailed work performance of patients with RA, such as absenteeism, presenteeism, and activity impairment12, although deterioration in these variables usually precedes work cessation and accounts for the largest component of total productivity losses.
In our study, we aimed to identify the factors related to work and activity impairment in patients with RA.
MATERIALS AND METHODS
Consecutive patients with RA who visited the Keio University hospital between January and September 2015 were included. Clinical information, including age, disease duration, comorbidity, tender or swollen joint count, visual analog scale (VAS), inflammatory markers, medication, the Health Assessment Questionnaire-Disability Index13, and the quality of life by EQ-5D14 were obtained from medical records. Disease activity and remission were calculated on the basis of the Disease Activity Score in 28 joints (DAS28)15, the Simplified Disease Activity Index (SDAI)16, and the Clinical Disease Activity Index (CDAI). Treatment was decided according to the treat-to-target strategy by certified rheumatologists in our department17,18. This study was approved by the ethics committee of Keio University School of Medicine (approval number: 20110136).
Work and activity impairment were measured by using the Work Productivity and Activity Impairment (WPAI) questionnaire for RA19,20, a self-reported questionnaire consisting of 6 questions on the extent of disease effects on patients’ productivity at work or home in the past 7 days. Absenteeism (% work absence because of RA), presenteeism (% impairment while working because of RA) for patients who were working for pay, and activity impairment (% health-related effect on regular activities because of RA) were calculated from the WPAI questionnaire responses.
Continuous variables were compared using the Student t test, the Mann-Whitney U test, or 1-way factorial analysis of variance with Bonferroni correction. Multivariable linear regression analyses were performed to identify the factors associated with work and activity impairment, adjusted for variables that were found to be significant in crude analyses or previous reports. Moreover, multivariable regression analysis adjusted for propensity score was performed to determine the benefit of productivity in remission over low disease activity (LDA) in various disease activity indices. Correlations were examined using Spearman correlations. Statistical analysis was performed with SPSS version 23.0 for Windows (SPSS Inc.). A p value < 0.05 was considered significant.
RESULTS
Among the 1558 patients with RA, 284 for whom information on activity impairment was not available were excluded. Thus, 1274 patients, including 451 who worked for pay (employed patients) and 823 who did not work, were enrolled (Supplementary Figure 1, available with the online version of this article). There were 524 homemakers included in the unemployed group. The characteristics of all patients and the employed patients are shown in Table 1.
Comparison of patients who are employed or unemployed in this study. Values are mean ± SD unless otherwise specified.
Of all the patients, 67.4% reported activity impairment (mean 23.7 ± 26.7%). Absenteeism (1.7 ± 9.1%) was reported by 5.2% and presenteeism (15.1 ± 21.5%) was reported by 52.7% of the employed patients.
Multivariable regression analyses after adjustment revealed the independent risk factors for activity impairment, absenteeism, and presenteeism (Table 2). Activity impairment in all patients was associated with factors pertinent to disease activity. Higher pain VAS scores (ß = 0.41, 95% CI 0.35–0.47, p < 0.01), use of biologic agents (ß = 3.57, 95% CI 1.60–5.54, p < 0.01), and oral corticosteroid (ß = 5.71, 95% CI 3.10–8.32, p < 0.01) were associated with exacerbated activity impairment, and DAS28 remission (ß = −2.97, 95% CI = −5.13 to −0.81, p < 0.01) and higher EQ-5D (ß = −58.71, 95% CI −65.15 to −52.27, p < 0.01) were protective factors. Among the employed patients, presenteeism was similarly associated with the disease-related variables, while the EQ-5D (ß = −11.98, 95% CI −18.28 to −5.68, p < 0.01) was the only independent factor associated with absenteeism. The disease duration was not related with either index.
Effect of remission in work and activity impairment in patients with RA.
We compared work and activity impairment among patients with different disease activity statuses as determined by the DAS28, SDAI, and CDAI (Figure 1). The patients in DAS28 remission showed significantly less activity impairment than those with LDA or moderate/high disease activity (MDA/HDA; 13.4 ± 18.9 vs 26.7 ± 26.7 vs 42.0 ± 29.3, respectively, p < 0.01), and similar results were obtained for both SDAI and CDAI. Among the employed patients, there was a significant difference in presenteeism among the DAS28 remission, LDA, and MDA/HDA groups (9.3 ± 16.2 vs 21.0 ± 22.8 vs 30.0 ± 24.3, respectively, p < 0.01), and the results were comparable with those obtained for SDAI and CDAI. The overall absenteeism rate was low, and no significant differences were observed among patients with different disease activity statuses; however, the absenteeism rate was lowest for remission patients, followed by LDA and MDA/HDA patients according to the SDAI and CDAI (SDAI: 1.1 vs 2.5 vs 4.1, p = 0.18; CDAI: 1.0 vs 2.6 vs 3.8, p = 0.14, respectively). Additionally, we found positive correlations between DAS28 and activity impairment (r = 0.42, p < 0.01) and presenteeism (r = 0.47, p < 0.01).
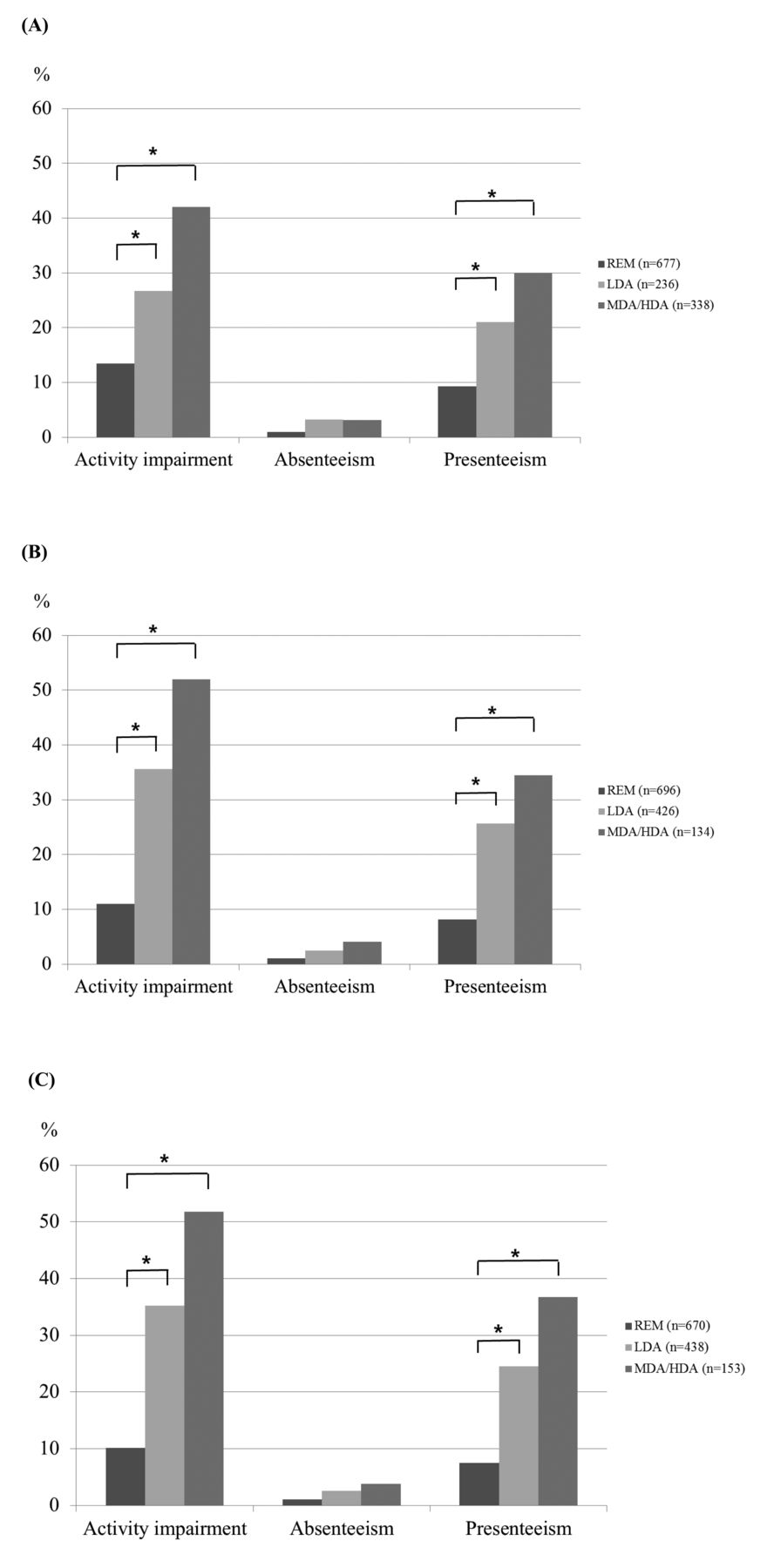
Comparison of work and activity impairment by disease activity indices. A. Disease Activity Score in 28 joints. B. Simplified Disease Activity Index. C. Clinical Disease Activity Index. * p < 0.0167 by Bonferroni adjustment. REM: remission; LDA: low disease activity; MDA: moderate disease activity; HDA: high disease activity.
Further, to validate the benefit of remission over LDA on productivity, we adjusted influential factors to work productivity and/or disease activity by propensity score adjustment, including age, sex, RA disease duration, comorbidity positivity, pain VAS, EQ-5D, and use of methotrexate, other conventional synthetic disease-modifying antirheumatic drugs, biologic agents, and oral corticosteroids. Obtaining remission had a significant protective effect on activity impairment compared with LDA in all indices (ß = −3.95, 95% CI −6.67 to −1.22, p < 0.01 in DAS28; ß = −3.00, 95% CI −5.88 to −0.12, p = 0.01 in SDAI; and ß = −4.20, 95% CI −7.10 to −1.30, p < 0.01 in CDAI), while remission was not associated with absenteeism in all indices (Supplementary Table 1, available with the online version of this article). In presenteeism, remission showed a significant protective effect only in DAS28 (ß = −5.63, 95% CI −10.02 to −1.24, p = 0.01 in DAS28; ß = −3.13, 95% CI −7.85 to 1.58, p = 0.19 in SDAI; and ß = −4.41, 95% CI −8.99 to 0.17, p = 0.06 in CDAI).
DISCUSSION
Our study revealed that about two-thirds of patients with RA were experiencing activity and work impairment, and when compared to patients in remission, activity impairment and presenteeism were not reduced adequately in patients in LDA.
Although absenteeism was very low (1.7%), presenteeism was as high as 15.1% and activity impairment was 23.7%, indicating that the majority of patients with RA still experienced difficulties engaging in full work or activity despite the recent treatment advancements. A few studies reported an association between work productivity and patient activity scale12, pain, and poor physical function21. Similar to previous studies, the multivariable linear regression analyses in our study demonstrated an association between overall activity impairment and presenteeism and disease-related indices, including pain, functional disability, and disease activity scores. Although pain and functional disability could be a result of longterm RA, it could also be attributed to residual disease activity because disease duration was not associated with activity impairment and presenteeism. Indeed, productivity loss was significantly correlated with the disease activity score in our study.
We showed that presenteeism and activity impairment were significantly improved in patients in remission as compared with patients in LDA, even after adjusting for various background characteristics and treatments. Although absenteeism was very low among all patients, it was the lowest for patients in remission. In addition to the mounting evidence of the benefits of clinical remission over LDA regarding better outcomes, such as radiographic changes and disability, our results indicate that clinical remission is also essential to improve work productivity. Notably, the considerably low absenteeism rate observed in our study, which was conducted in 2015, is unique. Studies conducted in 2008 reported that 26% of patients with early arthritis took sick leave for longer than 2 weeks within a span of 6 months21, and 41% had taken leave in the last 12 months22. A UK registry reported absenteeism to be 8.7% in 20129. The improvement in absenteeism rates with time can be attributed to advancements in therapies; differences in socioeconomic and cultural background would also contribute to the difference.
The EQ-5D index score was significantly associated with all indices. This finding is in line with a previous study that reported a strong association between quality of life determined with the Medical Outcomes Study Short Form-36 survey23 and work impairment24. A reciprocal relationship between quality of life and activity and work impairment may exist. Reduced mobility, self-care ability, and increased pain by arthritis may lead to impaired work and activity, and work productivity impairment can also increase anxiety and depression among patients with RA. However, because our study was cross-sectional in design, it was not possible to reveal the causal relationship.
Our study has some limitations. First, it was a retrospective study, and data related to important socioeconomic factors such as job type, education level, disability pension, and income were not available. Second, the cross-sectional design of the study prevented us from identifying time-series changes in work productivity, and further prospective longitudinal studies are needed to evaluate those changes.
Two-thirds of patients with RA experienced work and activity impairment. Remission achievement is essential to improve work and activity impairment.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
- Accepted for publication April 11, 2017.








{kind=link}