

Abstract
Objective. Spondyloarthritis (SpA) and Takayasu arteritis (TA) are 2 chronic inflammatory diseases; their coexistence in a single patient is uncommon. The aims of our study were to describe clinical features of patients having SpA associated with TA and to identify some characteristics of the types of patients with SpA associated with TA. We also analyzed treatments used in this context.
Methods. This French multicenter retrospective survey called for observations on behalf of the Club Rhumatismes et Inflammations, with a standardized questionnaire established by the investigators.
Results. We included 14 patients (women: 10/14; median age at SpA diagnosis: 43.5 yrs, ranging from 19 to 63). Subtypes of SpA were ankylosing spondylitis (n = 11), psoriatic arthritis (n = 2), and synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome (n = 1). HLA-B27 was positive in 3 cases, negative in 9, and unknown in 2. SpA was diagnosed before TA in 13 cases. Imaging findings compatible with the diagnosis of TA were found with computed tomography (11/14) and/or Doppler ultrasound (10/14). Laboratory tests showed increased acute-phase reactants in all cases (C-reactive protein ≥ 25 mg/l in 71% of the cases). All patients except 1 received corticosteroids and 7 were treated with anti–tumor necrosis factor (anti-TNF).
Conclusion. Association of SpA and TA is rare but probably not coincidental. Peripheral pulse palpation and vascular auscultation should be systematic and are the first indicators of TA in patients with SpA. Moreover, increased acute-phase reactants during SpA followup should lead to search for TA. Finally, there are therapeutic implications because anti-TNF are efficient in SpA and might be efficient in TA.
Spondyloarthritis (SpA) represents a heterogeneous group of chronic interrelated inflammatory arthropathies affecting mainly the spine but also entheses and peripheral joints. It shares a close association with HLA-B27. SpA has an overall incidence in whites of 0.30%, with a similar prevalence in women and men in France1. The frequency of HLA-B27 positivity in ankylosing spondylitis (AS) varies from 65.7% to 83.5% in France, depending on the classification criteria used2.
Takayasu arteritis (TA) is a rare chronic large vessel vasculitis of unknown etiology predominantly affecting the aorta, its major division branches, and pulmonary arteries. Women represent 62% to 97% of the patients with TA. Despite many advances in the understanding of genetic susceptibility to TA and its inflammatory mechanisms3, the pathogenesis of this disease remains unclear. The clinical course of TA is thought to progress through nonspecific systemic symptoms such as fatigue, low-grade fever, and weight loss, and depending on the vessels involved, through a wide variety of vascular or ischemic manifestations. Several sets of diagnostic criteria have been proposed, but the criteria proposed by the American College of Rheumatology (ACR) in 1990 for the classification of TA4 are now the most widely used.
SpA and TA are 2 chronic inflammatory diseases, and although their association has been reported occasionally in the literature, some data have suggested that both diseases could coexist in a single patient5,6,7. This association could not be random because in some mouse models of SpA, specific inflammation of the aorta was observed8.
The aim of our study was to describe clinical features of patients who have SpA associated with TA, and to identify some characteristics of the types of SpA patients associated with TA. Finally, we analyzed treatments that were generally used in this clinical context.
MATERIALS AND METHODS
Data collection relied on a call for observations on behalf of the Club Rhumatismes et Inflammations. This organization is a subgroup of the French Society of Rheumatology. It is a Web-based community that forms a professional network of more than 2000 physicians from different medical specialties involved in the treatment of inflammatory diseases. This organization has much experience in retrospective studies on rare diseases or rare associations, done by collecting cases obtained through calls from its electronic newsletter. Cases were included into our study between April 2012 and November 2014. A standardized questionnaire was established by the investigators. As a retrospective survey, no ethics board approval was needed, in accordance with the policy of our institution. Demographic data (age, sex, ethnicity) were collected as well as personal and family history. These data were completed with the description of the first symptoms observed at SpA and/or TA onset and description of treatments used for these patients. TA was diagnosed according to the 1990 ACR criteria4 and SpA according to the Amor criteria9. Diagnosis of synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome corresponded to criteria defined by Kahn and Kahn in 199410.
For SpA, the questionnaire collected the following data: the presence of sacroiliitis, peripheral and/or axial involvement, uveitis, psoriasis, aortic insufficiency, and Crohn or ulcerative colitis. The HLA-B27 status was also considered. Moreover, we collected the highest and lowest C-reactive protein (CRP) levels during SpA evolution. We also asked for the timetable of treatment introduction and interruption including nonsteroidal antiinflammatory drugs (NSAID), disease-modifying antirheumatic drugs (DMARD), and anti-tumor necrosis factor-α (anti-TNF).
For TA, the following data were collected: limb claudication, vascular sounds, diminished or absent pulse, high blood pressure, carotidynia, neurological trouble, stenosis and/or occlusion on ultrasound (US) or computed tomography (CT) images, and a detailed treatment chart (corticosteroid, immunosuppressive therapy, antiaggregant/anticoagulant therapy, and vascular surgery).
RESULTS
This national survey permitted collection of patient cases from 10 French medical centers specialized in rheumatology (n = 8) or internal medicine (n = 2). Of the 14 patients, 10 were women (sex ratio 2.5 women/1 man). All patients were white. Demographic characteristics of the patients are summarized in Table 1. Clinical and biological data are presented in Table 2.
Demographic and clinical characteristics.
Clinical and biological characteristics of SpA and TA and treatments (n = 14).
SpA was diagnosed before TA in 13 cases, with a median time of 4.5 years (from 1 month to 21 yrs), and 3 years after TA in 1 case. SpA diagnosis fulfilled Amor criteria in all cases. Sacroiliitis was identified in 11 cases: 1 by radiograph and magnetic resonance imaging (MRI), 5 by radiograph only, and 5 by MRI only. During SpA patient followup, TA-revealing symptoms were clinical detection of a diminished/absent pulse (4/13), superior limb claudication (2/13), and vascular sound (2/13). Other TA diagnoses were made by the exploration of visual loss (1/13), inflammatory cervical pain (1/13), or the radiological detection of radial artery thrombosis (1/13) or systemic inflammation (2/13). CRP was ≥ 5 mg/l in all 14 patients and ≥ 25 mg/l in 71% of the cases. Before TA diagnosis, median highest CRP observed during SpA evolution was 59 mg/l (from 6 to 250 mg/l).
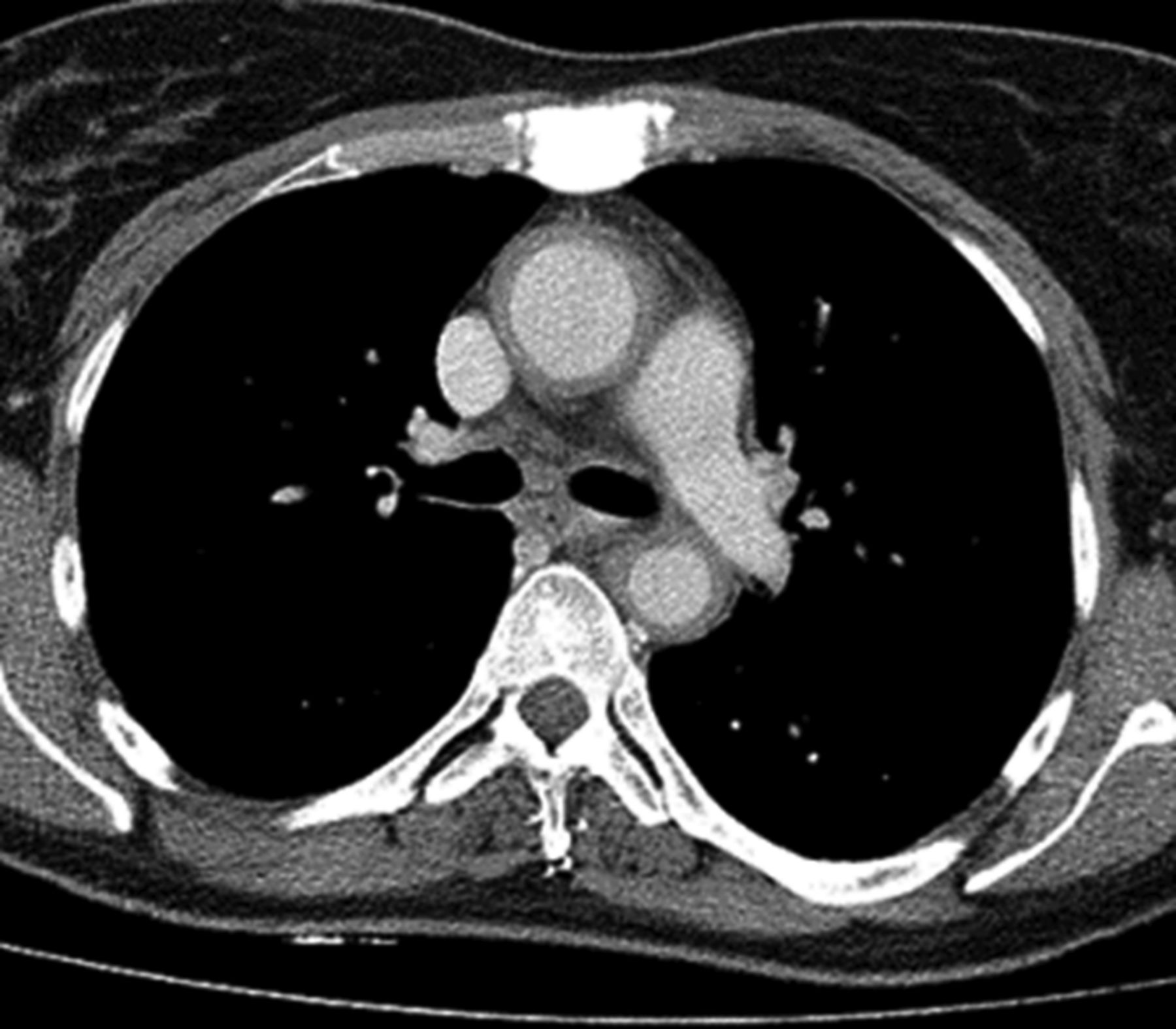
Imaging findings compatible with the diagnosis of TA were found with either contrast-enhanced CT or magnetic resonance angiography (14/14; Figure 1, Figure 2, and Figure 3⇓) and/or Doppler ultrasound (10/14). Positron emission tomography (6/14) was performed for 6 patients and showed fixation on vascular lesions. For 1 patient, histological analysis of a surgical piece of descending aorta showed a giant cell and plasma cells aortitis.

Magnetic resonance angiography showing occlusion of both common carotid arteries. Patient had synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome and Takayasu arteritis. A. Supraaortic vessels. B. Intracranial vessels.
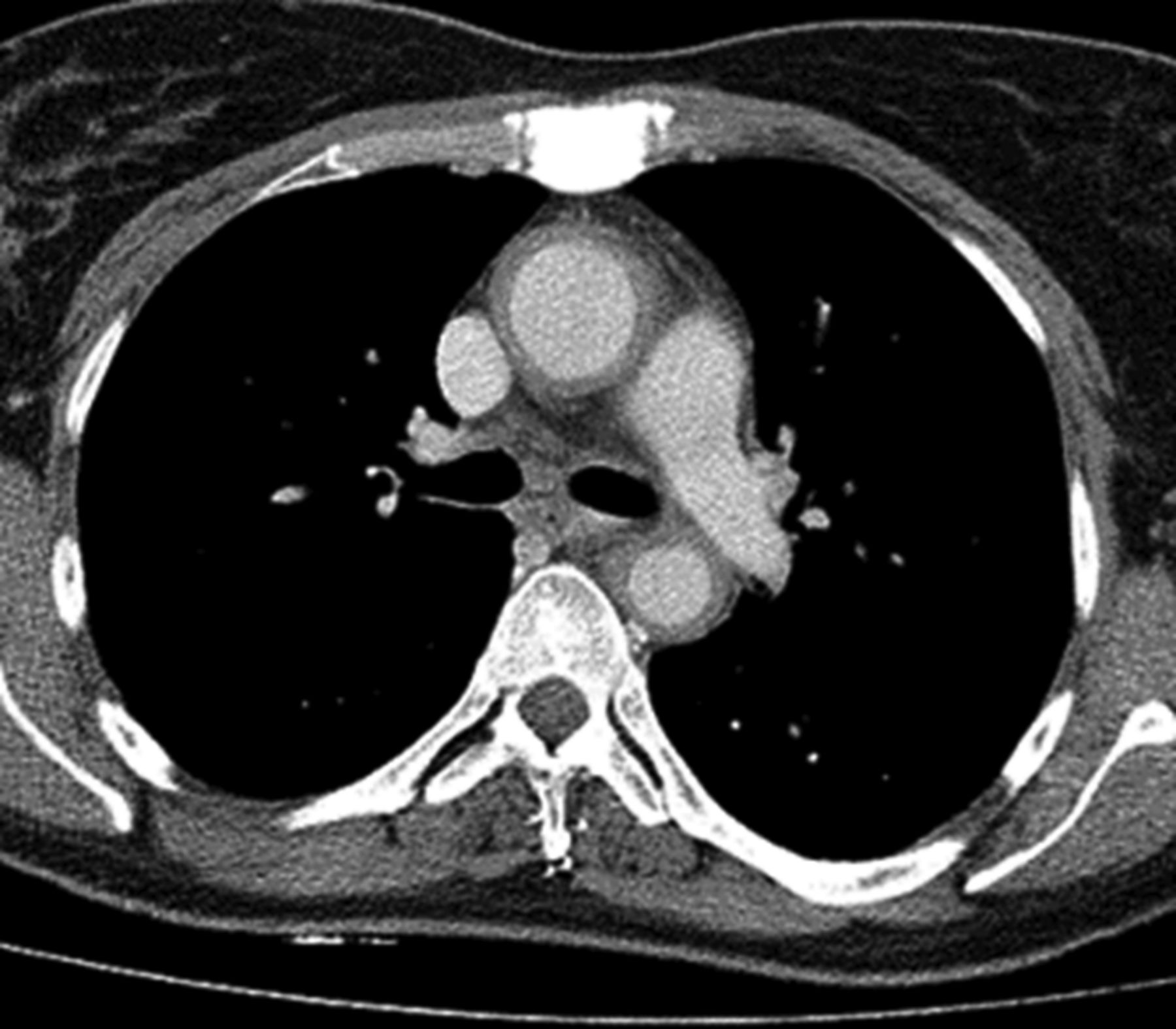
Thoracic contrast-enhanced computed tomography: circumferential thickening of aortic wall up to 4 mm. Patient had synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome and Takayasu arteritis.

Magnetic resonance angiography of supraaortic vessels. Occlusion of the right and left subclavian arteries. Occlusion of proximal segments of right and left vertebral arteries.
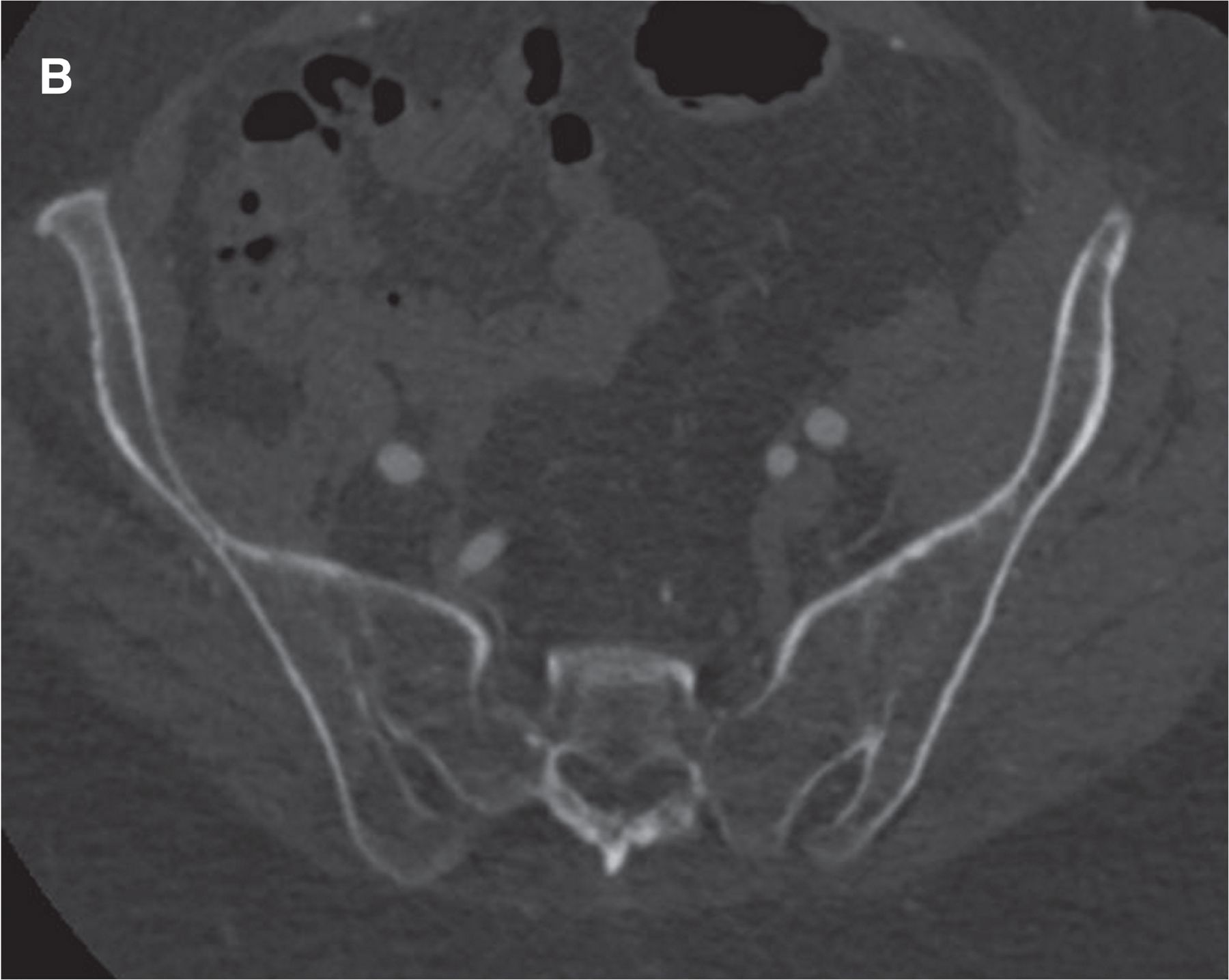
Axial computed tomography scan showing bilateral ankylosis of sacroiliac joints.
Treatment of SpA included NSAID for all patients except 1 (treated with corticosteroids), combined with DMARD (n = 10): methotrexate (MTX; n = 7) and sulfasalazine (SSZ; n = 3). Two allergic skin reactions with SSZ led to withdrawal of the drug. Three patients received only NSAID and did not require DMARD. All patients except 1 (who required surgery immediately) received corticosteroid at TA diagnosis (1 mg/kg/d with progressive decrease for 8 patients; others received from 0.1 mg/kg/d to 0.25 mg/kg/d).
Seven patients were treated with biologic therapies: 4 with etanercept [ETN; among them, 2 had to switch to infliximab (IFX) after TA diagnosis and 1 required a switch to adalimumab (ADA) and then to golimumab because SpA was still active], 2 with ADA [1 required a switch to rituximab after TA diagnosis and was ultimately treated with tocilizumab (TCZ) with good efficacy], and 1 with IFX, which was introduced because of TA activity signs. Anti-TNF treatment was started in 4/7 cases after TA diagnosis. For 3 patients, TA occurred while taking anti-TNF. In these cases, anti-TNF exposure varied from 1 to 5 years and all received ETN. SpA was not well controlled at TA onset for these 3 patients. In 2 cases, the choice of anti-TNF was driven by the TA diagnosis.
Vascular surgery was performed in 4 patients. Two surgeries were followed by severe postoperative complications: 1 sequential double bypass between ascending aorta, subclavian artery and the carotid bifurcation, and 1 Bentall surgery. The 2 other surgeries were 1 bypass between the right subclavian artery and the humeral artery and 1 thoracic descending aorta replacement performed in emergency because of a fissured aneurysm, followed by aortic cross and distal ascending aorta replacement.
Followup data were available for 7 patients. Mean followup duration after diagnosis of TA was 4.5 years. During the last visit of the 7 patients treated with biologic therapy, all were still under biologic therapy. Six patients were treated with anti-TNF and 1 received TCZ. TA was in remission for all of these patients, defined by the absence of new symptoms related to TA and inflammatory syndrome. Imaging followup data were available for 4 patients and showed stabilization or regression of vascular lesions.
DISCUSSION
This retrospective survey identified 14 patients presenting SpA associated with TA, suggesting that this association might not be random. We herein present the largest series reported to date, to our knowledge.
Our results show that characteristics of patients presenting both diseases are different from characteristics usually described for isolated SpA: a major proportion of women (sex ratio of 2.5 women/1 man), a higher median age (43.5 yrs) at SpA diagnosis, and greater frequency of HLA-B27 negativity (9/12), even though the diagnosis of AS was the most frequent type of SpA (11/14 cases). More importantly, we observed in all patients an increase of CRP level before and at the time of TA diagnosis. This suggests that the elevation of acute-phase reactants might constitute a good indicator for TA research in patients with SpA. Therefore, we should be cautious when dealing with a patient presenting a biologic inflammatory syndrome without infectious or other inflammatory disease such as inflammatory bowel disease during SpA evolution.
The main limitation of those results stems from the small number of patients and the retrospective design of our study. However, because of the scarcity of the association, it would have been difficult to find more patients responding to all diagnostic criteria. As noted, SpA was diagnosed before TA in 13 of 14 cases, which may be due to the source of recruitment in internal medicine and rheumatology departments. Recent studies supported the hypothesis of association between SpA and TA. Gudbrandsson, et al11 published a study based on a southeastern Norway population that found a prevalence of 22 cases of TA per 106 in northern Europeans. In that study, authors observed an important frequency of SpA and Crohn disease among patients with TA (7% and 8%, respectively), whereas the usual prevalence of SpA in a French population is estimated at 0.3%. Those results support an association between SpA and TA. As suggested by Gan, et al, in a Chinese population, prevalence of TA in SpA and SpA in TA are both higher than in the general population12. Thus, coexistence of these rare diseases might be more than a coincidence.
Should aortitis associated to SpA and TA be considered as 2 distinct diseases? As suggested by Palazzi, et al13 in their review, patients with AS, and less frequently, with other SpA, may develop cardiovascular manifestations ranging from asymptomatic forms to life-threatening conditions. The most important cardiovascular manifestation of AS is aortitis, which involves the aortic root and the ascending aorta and leads to valvular insufficiency. For 1 case involving the abdominal aorta, pathologic examination of the aneurysmal wall revealed hyalinization of the connective tissue, with several lymphocytic infiltrates, conspicuous calcification, and absence of elastic fibers. These findings are similar to those reported in AS-ascending aortitis. In our cases, patients presented with more than aortitis — they developed other vascular lesions such as stenosis of the subclavian artery, mesenteric arteries, and the common carotid. One hypothesis could also be that SpA with aortitis is in fact SpA associated with TA, that is, the aortitis and TA could constitute a continuum of the same disease. Moreover, we reported TA occurring not only during AS evolution but also during psoriatic arthritis and even SAPHO. Therefore, an exhaustive evaluation of all vessels and a clinical examination of all peripheral arterial pulses is important during SpA followup.
Common pathogenic mechanisms, supported by antigenic analogy between the aorta and the enthesis, could favor the occurrence of both diseases. To illustrate this hypothesis, Sherlock, et al8 showed in an animal model of SpA that the enthesopathy observed is linked with T lymphocytes (enthesis-resident), which have a double-negative phenotype and interleukin 23 (IL-23) receptor. In this model, cells are IL-23 sensitive, and in vivo expression of IL-23 is sufficient to phenocopy the human disease with the development of enthesitis and entheseal new bone formation. Inflammation also develops at the aortic root and valve, which are structurally similar to entheses. Then, on the condition that the animal model corresponds to the human model, this physiopathological hypothesis could explain in part the observations of aortitis occurring during SpA evolution and could explain the association between TA and SpA.
There is evidence that anti-TNF therapy is highly effective in SpA. Conventional therapy for TA consists of glucocorticoids, which may be associated with other immunosuppressive drugs (MTX, cyclophosphamide, or mycophenolate mofetil). However, some patients fail to achieve remission with conventional treatment, and anti-TNF could be useful for them14. Comarmond, et al15 reported the main characteristics, treatments, and outcomes of 84 patients (5 personal cases and 79 patients from the literature) with refractory TA treated with anti-TNF. First-line anti-TNF treatment included IFX in 81% of cases (68/84) and ETN in 19% (16/84). Most patients received IFX (5 mg/kg) associated with MTX or azathioprine. Anti-TNF are efficient in refractory TA patients, although side effects are observed in 20% of the cases. The pathogenesis of TA includes vessel injury due to activated T lymphocytes, natural killers, and macrophage products. Granulomatous inflammation is partly dependent on TNF, which is produced primarily in macrophages, T lymphocytes, and natural killers. TNF induces macrophage production of IL-12, a potent cytokine that enhances CD4 T lymphocyte differentiation to Th1 cells and activates natural killers. It is therefore likely that TNF inhibition might be useful in abrogating the immunoinflammatory features of TA.
Some authors16 reported cases of TA arising under anti-TNF therapy and propose a causal effect of the anti-TNF use on TA development. Others describe aortitis occurring under anti-TNF therapy17. Concerning our cases, we looked at the chronology of anti-TNF introduction and TA diagnosis and observed that in 11 cases out of 14, patients did not receive anti-TNF therapy before the TA diagnosis, discounting the anti-TNF role in the development of TA. Moreover, it is interesting to note that among the 3 patients who received anti-TNF before the diagnosis of TA, all were treated with ETN. As a soluble receptor, ETN has a different mechanism of action from monoclonal antibodies. It has been suggested that ETN preserves some of the mechanisms leading to granuloma formation, explaining the inefficiency of this agent in Crohn disease and certain forms of sarcoidosis. Arterial granulomatous lesions can be detected in TA. That could mean that ETN could not prevent TA in those 3 patients. This information is to be taken with caution because 1 of the patients had also received ADA.
Given those elements, anti-TNF drugs, with caution for ETN, may be good options for treatment of patients presenting SpA and TA when at least 1 of those diseases resists first-line treatments. Several extraarticular manifestations associated with SpA are already well known, such as uveitis, Crohn disease, ulcerative colitis, psoriasis, and cardiac manifestations. TA could represent another associated disease, which may be underdiagnosed in patients with a SpA. Moreover, because both diseases include use of anti-TNF as a therapeutic option, diagnosing their association is even more important.
The association of SpA and TA is rare but probably not coincidental. Careful peripheral pulse palpation and vessel auscultation should be routinely performed to alert the physician to TA diagnosis in patients with SpA. Moreover, increased acute-phase reactants during SpA followup, without alternative explanation, should alert physicians and lead to screening of patients for TA, as well as for inflammatory bowel disease. Finally, the identification of this association has therapeutic implications because anti-TNF have already demonstrated their efficacy in SpA and could also be effective in TA15.
- Accepted for publication February 23, 2017.








{kind=link}
{kind=link}
{kind=link}
{kind=link}