

Abstract
Objective. To examine the rate, risks factors, and consequences of neutropenia induced by intravenous (IV) biologic disease-modifying antirheumatic drugs (bDMARD).
Methods. We conducted a retrospective cohort study in 499 patients with rheumatic diseases treated by IV abatacept (ABA), infliximab (IFX), or tocilizumab (TCZ).
Results. Rheumatoid arthritis (RA) was the most frequent diagnosis (72%). Fifty-two patients (10.4%) experienced at least 1 episode of neutropenia. No episodes of grade 4 neutropenia were documented. TCZ was more frequently related to neutropenia than ABA or IFX (18.6% vs 3.8% and 2.8%, respectively, p < 0.001). The following factors were identified as predictors of experiencing neutropenia with IV bDMARD: history of neutropenia with methotrexate (MTX; synthetic DMARD; OR 1.56, 95% CI 1.17–7.14), concomitant treatment by MTX (OR 1.21, 95% CI 1.01–2.64), and TCZ treatment (OR 2.72, 95% CI 1.53–9.05). Patients experiencing a TCZ-induced neutropenia did not show a higher risk of severe infections; however, this group had a shorter drug survival (9 mos vs 20 mos, p < 0.02) compared with TCZ patients without neutropenia.
Conclusion. Among 3 different classes of IV bDMARD, TCZ is associated with the higher risk of neutropenia. No increased frequency of infection episodes was documented in this group.
Biologic disease-modifying antirheumatic drugs (bDMARD) have redefined the treatment of rheumatic diseases over the past decade. Despite their well-recognized safety, hematologic abnormalities, and in particular, neutropenia have been reported1,2.
Neutropenia is here defined by a circulating absolute neutrophil count (ANC) inferior to 2 × 109/l3. Besides dissimilar data collected in pre- and postmarketing trials, only a few studies have investigated bDMARD-induced neutropenia in real-world cohorts of patients with rheumatic diseases. Hastings, et al4 reported on a large cohort with 367 patients treated by tumor necrosis factor (TNF) inhibitors, and found that 18.8% patients had at least 1 episode of neutropenia during treatment. To our knowledge, no comparison between different classes of biologics has ever been made. Further, aspects such as predisposing factors, involvement of concomitant therapy by synthetic DMARD (sDMARD), and consequences of neutropenia remain unclear. Because the major serious event of biologics is infection, a serious concern is whether bDMARD-induced neutropenia could eventually increase this risk.
The aim of this report is to examine neutropenia in a cohort of patients treated with 3 different classes of intravenous (IV) bDMARD: a CTLA-4 antagonist, abatacept (ABA); a TNF-α inhibitor (TNFi), infliximab (IFX); and an interleukin (IL)-6 inhibitor, tocilizumab (TCZ). Incidence, risk factors, and effect of neutropenia on both risk of infection and drug survival were analyzed.
MATERIALS AND METHODS
Study population
A retrospective study was conducted of 499 patients treated with at least 1 of 3 IV bDMARD (ABA, IFX, or TCZ) from April 2009 to June 2014 at the Department of Rheumatology of Lapeyronie University Hospital (Montpellier, France). The start of followup was the first infusion of IV bDMARD, and the end of followup was last infusion by calendar date, lost to followup, or death. The analysis was performed only in the IV form because all the clinical and laboratory data were available owing to the rigorous followup made in each monthly or bimonthly visit patients made to receive their infusion. The study has received approval from the CHU of Montpellier ethics board (Comité de Protection des Personnes, CHU Montpellier, registered code 2014-A00824-43).
Data were collected from medical records. Demographic, clinical, and therapeutic features were recorded, including age, sex, type of rheumatic disease, disease duration, antibody status, history of neutropenia, baseline neutrophil counts, lowest observed ANC, white blood cell count, platelets blood count, and concomitant or prior use of medications including DMARD, corticosteroids, and IV or subcutaneous (SC) biologics.
“Drug survival” measures the length of time a patient continues to take a particular drug and encompasses factors such as drug effectiveness and side effects. To measure it, we consider the time between the onset and the last dose of the drug. “Drug failure” may be defined as either a lack of efficacy or patient intolerability to the treatment.
Rate of infection/severe infection was also recorded and expressed as 100 patient-years (PY). The criteria for defining a severe infection were (1) severe sepsis, (2) any infection requiring hospitalization or IV antibiotics, (3) any infection leading to need for oxygen or intubation, and (4) any of the following: pneumonia, pyelonephritis, deep tissue (invasive) infection, pseudomembranous colitis because of Clostridium difficile, meningitis, osteomyelitis, disseminated or complicated herpes zoster, and any infection that requires adjunctive surgical intervention.
To define neutropenia severity, common toxicity criteria3 grade was used as follows: grade 1, ≥ 1.5 and < 2.0 × 109/l; grade 2, ≥ 1.0 and < 1.5 × 109/l; grade 3, ≥ 0.5 and < 1.0 × 109/l, and grade 4 < 0.5 × 109/l4. The ANC was obtained within 3 days prior to IV biologic dose.
Statistical analysis
Comparisons were performed using the chi-square test for qualitative variables, and the Student t test or the Wilcoxon test depending on variable distribution for quantitative variable. To compare a variable in the 3 groups, a 1-way ANOVA test was performed. P value and 95% CI were estimated. To determine predisposing factors of neutropenia, a multivariate logistic regression analysis was done. Patients were divided into 2 groups according to the presence or absent of neutropenia. Comparisons were made between these 2 groups and variables associated with a p value inferior to 0.05 were chosen in a stepwise selection process to perform the analysis. OR and 95% CI were estimated.
A Cox regression analysis was carried out to estimate the HR of neutropenia comparing the 3 groups of treatment. With the purpose of analyzing TCZ survival between patients with and without neutropenia, a Mantel-Cox test was used. The significance level was set at 5% for all tests. Statistical analysis was performed using STATA software version 13.0 (StataCorp LP).
RESULTS
Demographics
Characteristics of the 499 patients are summarized in Table 1. Mean age was 57 years. Women represented 83% of the sample. Rheumatoid arthritis (RA) was the more common diagnosis (72.3%), followed by axial spondyloarthritis (AS; 20.2%). Concomitant treatment by sDMARD was documented in 51.5% of the sample and in 61.7% of patients with RA. Oral corticosteroid treatment was used by 49.8% of subjects. Sixty-four patients (12.8%) received 2 of the 3 IV bDMARD and 34 patients (6.8%) received all 3 of them. There were 129 patients treated with ABA, 213 with IFX, and 221 with TCZ (Table 2).
General characteristics of cohort.
Characteristics of patients according to IV bDMARD. Values are % unless otherwise specified.
Analysis of neutropenia
Details are summarized in Table 3. At least 1 episode of neutropenia was recorded in 10.4% (n = 52) of patients (ANC range 0.6–1.94 × 109/l) and 96% of them presented more than 5 episodes. Most subjects (90%) experienced a moderate neutropenia (grades 2 and 3). No episodes of grade 4 neutropenia were registered. The mean ANC before starting the drug was 3.2 ± 1.4 × 109/l. Suspensions of IV bDMARD were noted in 5.6% of patients because ANC was under 1 × 109/l. Treatment was stopped in only 1 patient (Felty syndrome) because of a concomitant severe thrombocytopenia. In this particular case, neutropenia improved transiently after stopping treatment; however, neutropenia returned later with an sDMARD.
Neutropenia and related variables according to IV bDMARD analyzed. Values are n unless otherwise specified.
Except for 1 patient who had AS, all other cases occurred in patients with RA. Neutropenia was more frequent with TCZ therapy (18.6% vs 2.8% and 3.8% in IFX and ABA groups, respectively, p < 0.001).
The first episode of neutropenia generally occurred within the first 3 months of treatment (median 9.5 weeks, range 1–108 weeks), although with TCZ therapy it was possible to identify 4 patients (9.7%) who developed neutropenia after the first year of treatment. Most patients receiving ABA and IFX had a history of neutropenia, mainly while treated with methotrexate (MTX). By contrast, patients experiencing their first event while treated with TCZ represented 93% of the group.
We found other cytopenias associated to neutropenia. Thrombocytopenia, lymphopenia, and the association of both were observed. No difference between the treatment groups was found. With ABA, 1 case of pancytopenia was identified. This patient had Felty syndrome. In 2 patients (1 ABA, 1 IFX), a bone marrow biopsy was performed showing in both cases a normal trilineage differentiation.
All patients receiving both ABA and IFX continued treatment without adjustments in dose or infusion interval. The course of neutropenia with TCZ therapy is analyzed below.
Predisposing factors of neutropenia
A multivariate logistic regression was performed to identify independent variables associated with the occurrence of neutropenia. Predisposing factors to develop neutropenia with IV bDMARD were (1) history of neutropenia while treated with MTX (OR 1.56, 95% CI 1.17–7.14), (2) concomitant use of MTX (OR 1.21, 95% CI 1.01–2.64), and (3) TCZ therapy (OR 2.72, 95% CI 1.53–9.05). No correlations with disease duration, antibodies status, or sex were identified (Table 4).
Predisposing factors of neutropenia. Values are % unless otherwise specified.
Neutropenia associated to TCZ therapy
Patients receiving TCZ treatment had a higher risk of experiencing an episode of neutropenia compared with other treatments (HR 2.55, 95% CI 1.09–5.33, p = 0.029). Forty-one patients (18.6%) presented at least 1 episode of neutropenia. In those patients, we observed an ANC mean reduction of 32% compared with the baseline. The magnitude of neutropenia was not associated to treatment response [American College of Rheumatology (ACR) 20, ACR50]. No differences were found between neutropenic and no neutropenic patients regarding mortality rate (0.9 vs 1.1, p = 0.89).
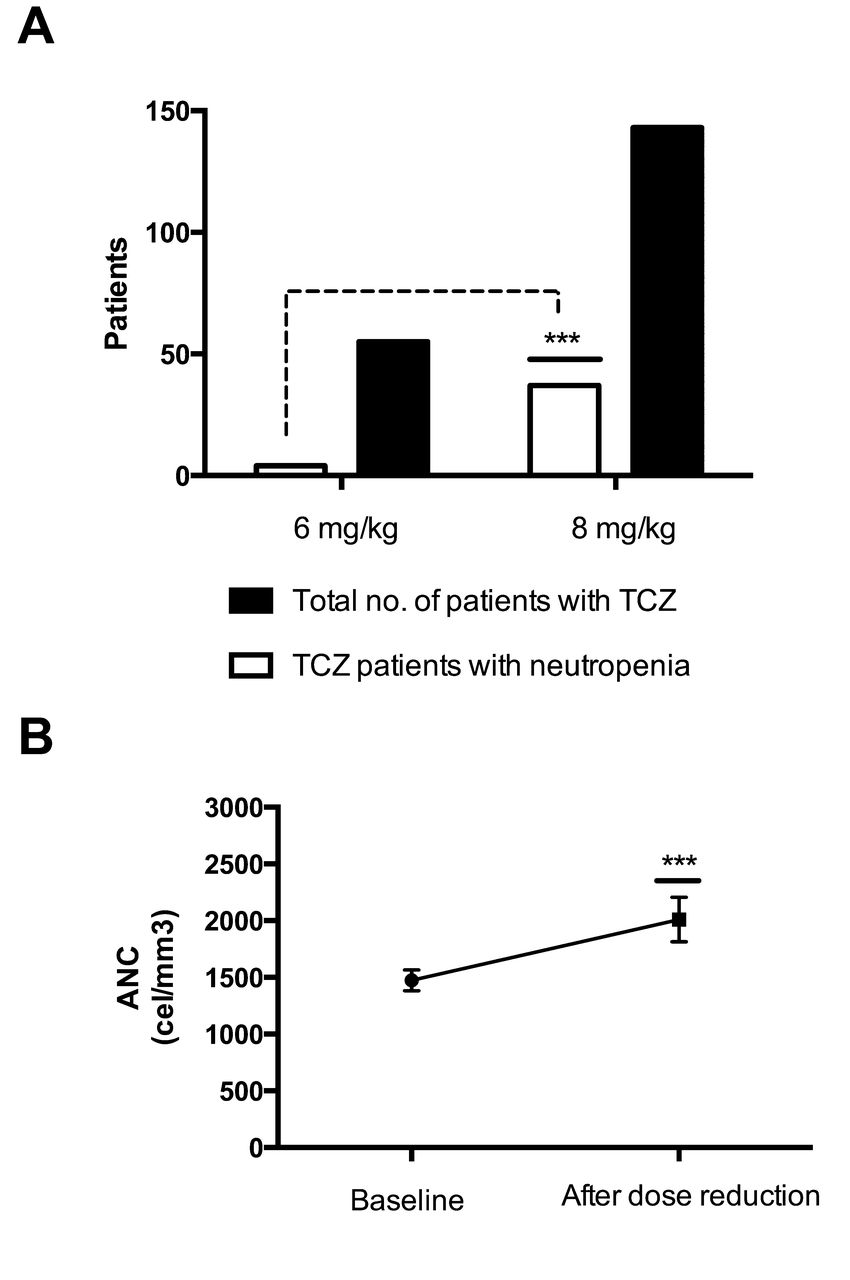
Neutropenia with TCZ seemed to be dose-dependent: an incidence of only 7.2% was found in patients who started TCZ at 6 mg/kg in comparison with 25.8% of patients who started at 8 mg/kg (p < 0.001; Figure 1A).

Incidence of neutropenia according to TCZ dose. (A) Comparison of neutropenia incidence between doses of 6 mg/kg versus 8 mg/kg. (B) Kinetic of ANC after a dose reduction. *** p < 0.001. TCZ: tocilizumab; ANC: absolute neutrophil count.
A reduction of TCZ dose was made in 98.3% of patients experiencing more than 3 episodes of neutropenia. With this strategy, an increase in ANC from 1474 ± 44.9 cel/mm3 to 2010 ± 95.9 cel/mm3 was achieved (p < 0.001; Figure 1B). A longterm dose of 6 mg/kg was maintained in 27.1% of patients, but in all other cases (72.9%) the dose was finally reduced to 4 mg/kg.
No cases of drug withdrawal were observed. Nonetheless, treatment failure occurred more frequently in the group of patients experiencing neutropenia (16.6% vs 9.4%, p < 0.001), leading to a shorter median drug survival in those patients (9 mos vs 20 mos, 95% CI 1.16–14.78, p < 0.02) compared with TCZ patients without neutropenia (Figure 2).

Median drug survival by a Kaplan-Meier analysis between TCZ patients with and without neutropenia. TCZ: tocilizumab.
Rate of infection regarding neutropenia
No differences were noted between TCZ patients with and without neutropenia regarding the rate of infection (92,100 PY vs 88,100 PY, 95% CI −0.04 to 0.07, p = 0.15) or severe infections (12,100 PY vs 11,100 PY, 95% CI −0.02 to 0.003, p = 0.13).
For IFX, the rate of infection was 97,100 PY (95% CI 79.1–121.3) and for ABA, 76,100 PY (95% CI 54.7–98.3). In both treatments, a comparison between patients with or without neutropenia was not possible because of the lower incidence of neutropenia.
DISCUSSION
In our study, we have scrutinized the characteristics of neutropenia associated to IV bDMARD in a real-world cohort of 499 patients with inflammatory rheumatic diseases. No comparatives studies between biologics with different molecular targets have been previously published, to our knowledge. TCZ, an IL-6 inhibitor, entails a higher frequency of neutropenia in comparison to ABA, a CTLA-4 antagonist, and IFX, a TNFi. TCZ-induced neutropenia remains moderate, without an increased risk of infection, but is associated to a higher rate of drug failure.
Ten percent of patients in our cohort presented at least 1 episode of neutropenia with dissimilar frequencies between each group of treatment. In ABA and IFX, very low frequencies of neutropenia were found. In both groups, previous history of neutropenia, mostly with MTX, was documented.
ABA phase III/IV studies did not report episodes of neutropenia5,6,7,8. Regarding IFX, initial safety studies suggested no increase in the risk of leukopenia9,10. Although in later observational studies, an elevated frequency of neutropenia was described11,12. Rajakulendran, et al13 reported an incidence of 14.3% in patients with RA. Subsequently, in an expanded cohort of patients with RA, AS, and psoriatic arthritis, Hastings, et al4 found an incidence of 18.8% for all TNFi [IFX, adalimumab (ADA), and etanercept] and up to 25.4% with IFX. Pappas, et al14 found an incidence of neutropenia of 13.8% in ADA and of 10.6% with other TNFi. In the analysis of 1322 biologic-naive patients with RA of the Corrona registry, no increased risk for developing neutropenia with TNFi was found because in about 8.7% of patients a neutropenic episode had already been documented before TNFi was initiated.
Data for neutropenia with TCZ incidence are divergent. In the TociLIzumab Safety and THE Prevention of Structural Joint Damage (LITHE) study15, a neutropenia frequency of 4.5% at 8 mg/kg was found; while De Benedetti, et al16 in a cohort of 112 patients with juvenile idiopathic arthritis (JIA) found an incidence as high as 57%. Several other studies, such as the TOWARD (Tocilizumab in cOmbination With traditional DMARD therapy)17, RADIATE (RheumAtoiD ArthrItis study in Anti-TNF failurEs)18, or AMBITION (Actemra versus Methotrexate double-Blind Investigative Trial In mONotherapy)19 trials, reported a frequency around 30%. The SUMMACTA [A Study to compare subcutaneous versus intravenous administration of RoActemra/Actemra (Tocilizumab) in participants with moderate to severe active rheumatoid arthritis] study20 comparing the safety and efficacy of IV versus SC TCZ found an incidence of 26% on IV and 37% on SC form. A dose-dependent effect on neutropenia-onset had been already noted in the LITHE and OPTION (Tocilizumab Pivotal Trial in Methotrexate Inadequate RespONders)21 studies, where the incidence of neutropenia at 8 mg/kg was almost twice that observed at 4 mg/kg. In addition, data from these trials confirm that grade 4 neutropenia (< 0.5 ANC × 109/l) is extremely uncommon.
A multivariate analysis was performed to elucidate independent risk factors associated to the appearance of neutropenia on IV bDMARD. History of neutropenia with MTX was supported by Hastings, et al4 as a predisposing factor. Interestingly, the analysis shows that concomitant use of sDMARD predisposes to develop neutropenia with biologics. In the univariate analysis, an association between RA and neutropenia was obtained. However, 2 of the 3 IV biologics are prescribed only for RA, therefore this association was not confirmed in the final model.
We considered the consequences of neutropenia, in particular regarding treatment with TCZ. Our study did not find an increased risk of infection among neutropenic patients receiving TCZ. De Benedetti, et al16 did not document an increased rate of infections either over 112 patients with JIA with higher incidence of neutropenia. The likelihood of infection is related probably to severity and duration of neutropenia episodes. In our cohort, as in the patients with JIA, neutropenia episodes were moderate. Further, TCZ-induced neutropenia seems to be explained by the margination of circulating neutrophils provoked by IL-6 inhibition22. In this sense, neither the ANC nor phagocytic neutrophil function are diminished. On the other hand, a shorter drug survival among TCZ patients experiencing neutropenia was observed. It is likely that drug failure was related to dose reduction made in patients with repetitive episodes of neutropenia.
An important strength of our study is the analysis of a real-world cohort of rheumatic patients treated by different IV bDMARD. However, our report also has some limitations. The retrospective design of our study limited the gathering of more accurate data regarding neutrophil kinetics. We cannot evaluate the approach to neutropenia events, in particular modifications of TCZ dose. Findings such as the involvement of concomitant sDMARD in neutropenia or shorter TCZ survival in neutropenic patients must be verified in prospective studies.
We believe that the data presented here permit a better perspective on the problem regarding frequency, severity, associated risk factors, and consequences. We report 3 major findings: (1) risk factors for developing neutropenia with IV bDMARD are history of neutropenia with MTX, concurrent treatment with sDMARD, and TCZ therapy; (2) neutropenia with TCZ is not associated to an increased risk of infections; and (3) TCZ-induced neutropenia is dose-dependent. Shorter TCZ drug survival could be associated to dose decrease strategy to improve ANC.
- Accepted for publication February 10, 2017.








{kind=link}
{kind=link}