

Abstract
Objective. To compare submaximal exercise capacity in patients with juvenile dermatomyositis (JDM) with controls, and analyze contributions of muscle, heart, and lung impairment in patients.
Methods. Fifty-nine patients with JDM, with a mean 16.9 years after symptom onset, and 59 sex- and age-matched controls completed a 6-min walk test (6MWT) and a timed up and go (TUG) test. Muscle function, disease activity/damage, and health-related quality of life (HRQOL) were assessed by validated tools; heart function by echocardiography and electrocardiography; and lung function by spirometry, DLCO, and body plethysmography. A thoracic high-resolution computed tomography (HRCT) scan and magnetic resonance imaging of the thighs were completed in patients.
Results. The 6MWT distance (6MWD) was 592 ± 81 m in patients versus 649 ± 79 m in controls (p < 0.001), and 563 ± 75 m in active versus 622 ± 76 m in inactive JDM (p = 0.004). The TUG time was 13.1 ± 2.1 s in patients versus 12.3 ± 2.0 s in controls (p = 0.034), and 13.7 ± 2.2 s in active versus 12.5 ± 1.8 s in inactive JDM (p = 0.028). No statistically significant difference was found between inactive JDM and controls in either test. In patients, the Childhood Myositis Assessment Score influenced the 6MWD and TUG time the most, followed by a low DLCO and HRCT pathology in the 6MWT and forced vital capacity in the TUG test. Medical Outcomes Study Short Form-36 physical component summary correlated strongly with both tests.
Conclusion. Submaximal exercise capacity was reduced in patients with JDM, particularly those with active disease. This reduction was associated with muscle and lung dysfunction and poorer HRQOL.
- JUVENILE DERMATOMYOSITIS
- LONGTERM DISEASE
- TIMED UP AND GO
- SUBMAXIMAL EXERCISE TESTING
- FUNCTIONAL CAPACITY
- 6-MIN WALK TEST
Juvenile dermatomyositis (JDM) is a rare autoimmune vasculopathy affecting mainly the skin and proximal skeletal muscle in children. Internal organs such as the heart and lungs may be involved. Research emphasis on longterm outcome has been growing during the last decades1,2,3. Literature has shown that about 60% of the patients have a chronic or polycyclic course2,4, while 60%–80% have disease damage2,3,5 at longterm followup.
In a Norwegian JDM cohort established by our research group, we have previously shown that 90% of patients had measurable cumulative organ damage1 and 50% had active disease6 after a median 16.5 years of disease duration. Compared with controls from the general population, patients had impaired muscle function7; subclinical, reduced lung function8; and subclinical systolic and diastolic cardiac dysfunction9,10. Fifty-two percent had magnetic resonance imaging (MRI)–detected muscle damage7 and 37% had thoracic high-resolution computed tomography (HRCT) pathology8. Patients also reported impaired health-related quality of life (HRQOL) through lower Medical Outcomes Study Short Form-36 (SF-36) physical component summary (PCS) compared with controls11. A Danish study found decreased maximal exercise capacity in patients with JDM in remission 14 years (mean) after disease onset12. We do not know, however, whether submaximal functional capacity, resembling activities of daily living, is reduced in JDM after longterm disease, or how muscle, lung, and heart impairment may influence this.
The 6-min walk test (6MWT) is a well-established submaximal exercise test most commonly used to assess cardiopulmonary function13. It has been validated for certain rheumatologic diseases such as systemic sclerosis14 and juvenile idiopathic arthritis15. In adult DM, a study of patients with interstitial lung disease (ILD), but without signs of muscle disease, showed a decreased 6-min walk distance (6MWD) comparable to patients with idiopathic interstitial pneumonia16. The 6MWT has never been systematically assessed in JDM. However, based on expert consensus, it was recently suggested as a core set test of submaximal aerobic fitness in both adult and juvenile idiopathic inflammatory myopathy (IIM)17, as well as a measure of both pulmonary and physical function to be included in clinical studies of IIM18.
The Timed Up and Go (TUG) test is an objective version of the earlier subjective Get Up and Go from 1986 that evaluated falling tendency in the elderly19. The TUG test assesses basic mobility skills by measuring the total time to complete a set of everyday tasks20. To our knowledge, the TUG test has never previously been assessed in patients with JDM, but has been shown to improve with blood flow resistance training in adult patients with DM/polymyositis21. Also, it was recently recommended through expert consensus as a physical function measure to be studied in IIM18.
The aims of our study were to compare submaximal exercise capacity by the 6MWT and the TUG test in patients with JDM after longterm followup with controls; find associations between these outcomes and disease variables in patients; and analyze the contribution of skeletal muscle, heart, and lung dysfunction to the 6MWT and TUG results.
MATERIALS AND METHODS
Patients and controls
Sixty-six patients diagnosed with JDM between 1970 and 2006 were identified as previously described1: 4 patients were dead, and 59 (95%) of the remaining 62 participated in the study. Inclusion criteria were a definite or probable DM according to the Peter and Bohan criteria22 diagnosed before the age of 18, and age ≥ 6 years at inclusion. There were no exclusion criteria for patients.
Controls (n = 59) from Oslo, Norway, and its surroundings matched for sex and age with the patients were randomly drawn from the Norwegian National Registry. Exclusion criteria were serious heart or lung disease, rheumatic disease, or the use of immunosuppressive medication for other immunologic conditions. Only 1 patient was excluded because of heart or lung disease (a woman with chronic atrial fibrillation).
Ethics
All participants (and guardians if age ≤ 16 yrs) submitted written consent prior to inclusion according to the World Medical Association of Helsinki. The study was approved by the Norwegian South East Regional Committee for Medical and Health Research Ethics (S-05144).
The 6MWT protocol
The 6MWT was set up in a plane, straight, indoor corridor of 20 m confined by 2 lines. Two research nurses alternated instructing the test. All participants wore a pulse watch and comfortable shoes, and were given the same instructions: to walk as fast and far as possible for 6 min without running; to turn behind the lines; and to regulate the tempo to stay in motion for 6 min if strenuous. Termination criteria were breathing difficulties, chest pain, or other major physical troubles. Encouragement during the test was reduced to informing about the time spent at 2, 4, and 5 min, and when 30 s remained. A countdown of the last 10 s was loudly proclaimed to prepare for stop. The 6MWD was registered every 40 m and at the end. Heart rate was measured before, directly after, and 1 min after the test. All participants scored their experienced exhaustion on a modified version of the Borg scale23, a grading scale of perceived exertion, ranging in whole numbers from 1 = very easy to 7 = extremely exhausting performance.
The TUG Test Protocol
For the TUG test, a chair was placed in the middle of a room with a perpendicular line marked on the floor 10 m away. All participants were instructed to use comfortable shoes as well as any aiding devices needed to complete the test: to rise from the chair, walk to the line, turn behind the line, walk back to the chair, and sit down. Total time spent (TUG time) was measured with a stopwatch. After test completion, the research nurse scored falling tendency ranging from 1 = normal to 5 = severely abnormal.
Self-assessment and scoring of disease activity and damage
A self-reporting questionnaire was used to assess average weekly physical activity inducing sweating or breathlessness during the last year, as previously described in detail7. For the present study, we recategorized according to hours of exercise: 0 = < 2–3 h/week and 1 = ≥ 2–3 h/week; and to exercise frequency: 0 = < 2–3×/week and 1 = ≥ 2–3 h/week. The following validated tools were used as reviewed by Rider, et al24: HRQOL was measured by the SF-36 in all participants ≥ 14 years. In patients, self-reported physical disability was measured by the Health Assessment Questionnaire (HAQ)-Disability Index in subjects ≥ 18 years and the childhood HAQ (CHAQ) in subjects < 18 years. Disease activity was scored by 1 physician according to the Disease Activity Score (DAS), as well as the Myositis Disease Activity Assessment Tool consisting of the Myositis Disease Activity Assessment Visual Analogue Scale and the Myositis Intention to Treat Activity Index. Disease damage was scored according to the Myositis Damage Index. Also, the Pediatric Rheumatology International Trials Organization criteria for inactive disease were used to divide the patient cohort into active and inactive disease25.
Muscle, lung, and heart evaluation
As previously described in detail7, muscle strength in both patients and controls was assessed by the unilateral manual muscle test (MMT-8), and muscle endurance by the Childhood Myositis Assessment Scale (CMAS)24,26. Lung function was assessed by dynamic spirometry, whole-body plethysmography, and single breath diffusion capacity of carbon monoxide adjusted for hemoglobin concentration (DLCOc)27,28,29. Low forced vital capacity (FVC), total lung capacity, and DLCOc were defined as less than the fifth percentile of predicted values30. Heart function was assessed by a resting electrocardiography (ECG), blood pressure, and echocardiography10,31,32. MRI of thigh muscles and thoracic HRCT were completed in patients only. MRI was used to assess muscle edema (reflecting disease activity) and muscle fat infiltration, atrophy, and calcification (reflecting disease damage), and HRCT was used to assess ILD, airway disease, and chest wall calcinosis7,8.
Statistical analyses
For statistical analyses, we used IBM SPSS statistics version 22. For comparison of 2 groups, the independent sample Student t test and the Mann-Whitney U test were used for continuous variables as appropriate; the chi-square test was used for categorical variables. To control for physical activity frequency as a confounder for the 6MWD and TUG time, hierarchical, linear multiple regression analysis was used. To find associations between the main outcomes and disease-specific variables in the patient group, as well as determinants for the main outcomes, correlation analyses [Pearson (r) and Spearman (Rsp) as appropriate] were used. Correlations were defined as strong r ≥ 0.7, medium r = 0.3–0.69, or weak r < 0.3. Then, a multiple linear regression analysis using a manual, backward stepwise elimination procedure was performed. Independent heart, lung, and muscle variables were tested in the multivariate model if their univariate p were < 0.1. The regression analysis of the 6MWT was controlled for age, sex, weight, and height as recommended13; the analysis of the TUG test was controlled for age and sex. Controlling variables were forced into the model. Independent variables that intercorrelated r > 0.7 were avoided. MMT-8 was excluded because of clinical similarity with CMAS despite r < 0.7, and ECG pathology was excluded because of a positive correlation with the 6MWD regarded as a type I error. For all analyses, a p < 0.05 was considered significant using 2-tailed tests. Effect size was calculated using Cohen d according to the formula (mean group 1 − mean group 2) ÷ pooled SD. Effect sizes were defined as small = 0.3, medium = 0.5, or large ≥ 0.8.
RESULTS
General and disease-specific characteristics of patients and controls
As described earlier1,6,7,8, patients with JDM were not significantly different from controls in sex, age, height, weight, number of smokers, or body mass index (Table 1). The same applied to patients with active disease compared with those with inactive disease, as well as patients with active or inactive disease compared with controls (data not shown). Twenty-one percent more controls exercised ≥ 2–3× weekly compared with patients (p = 0.014), while there was no statistically significant difference in exercise frequency between patients with active and inactive disease. The SF-36 PCS score was lower in patients compared with controls, as well as in patients with active compared to inactive disease.
General- and disease-specific characteristics of patients and controls and of patients with active and inactive disease. Continuous variables are presented as mean (SD) or median (interquartile range). Categorical variables are presented as frequency (%) or frequency/total (%) in the case of missing data.
Patients had reduced muscle strength, pulmonary function, and systolic and diastolic cardiac function compared with controls, as earlier described in detail7,8,9,10 (Table 1). Patients with active disease had reduced scores on both muscle strength and muscle endurance, and had reduced cardiac diastolic function compared with patients with inactive disease. No statistically significant difference in lung function was found between patients with active and inactive disease.
The 6MWT and the TUG test in patients (including active and inactive patients) and controls
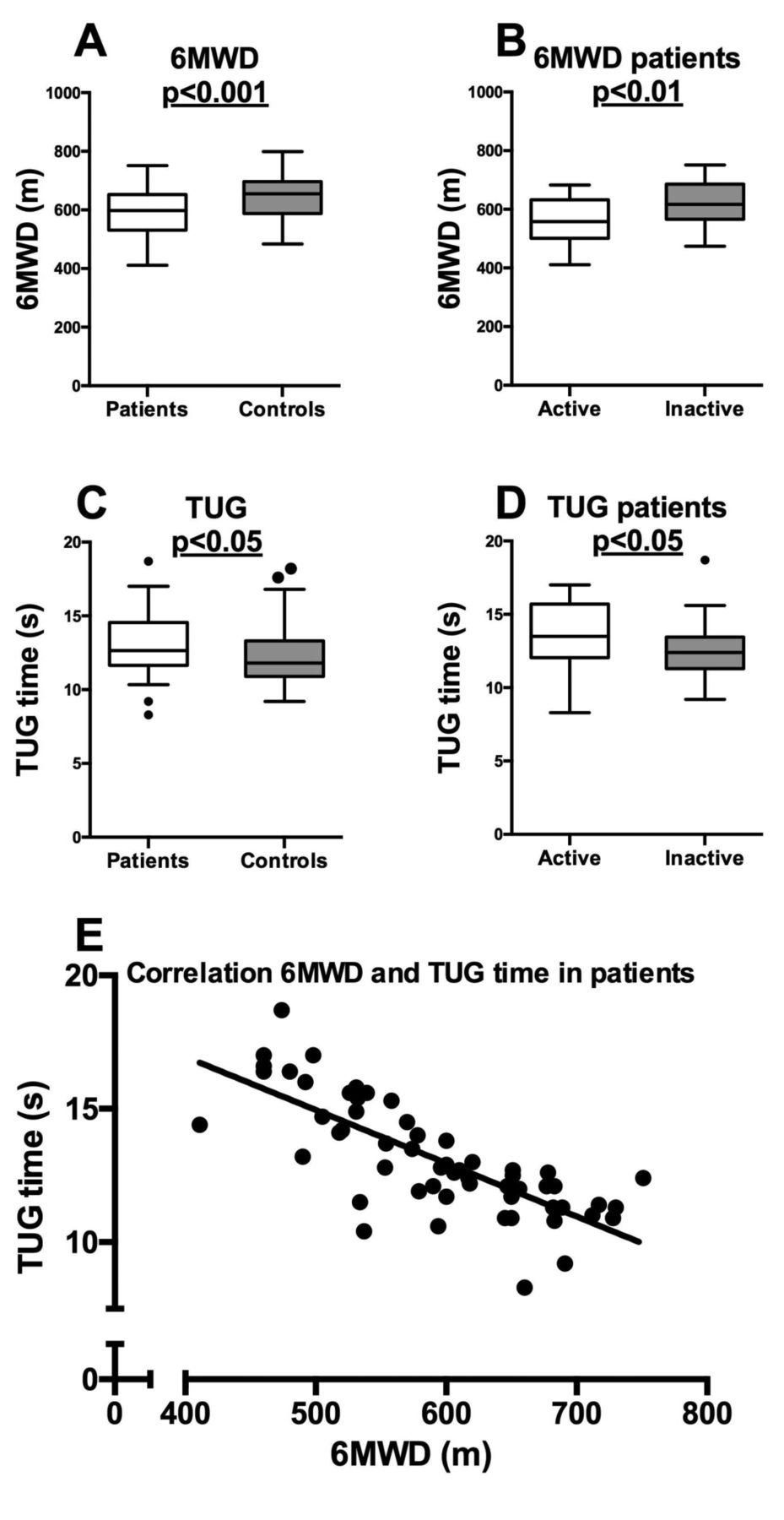
Fifty-eight patients and 59 controls completed the 6MWT and the TUG test. Patients walked a mean distance of 57 m shorter (95% CI 28–86, p < 0.001, Cohen d = 0.7) than controls (Table 2, Figure 1A), and this difference was still significant after controlling for physical activity frequency (βadj = 42.2, 95% CI 11.8–72.6, p = 0.007). The performance effort of the 6MWT was comparable in the 2 groups; there was no statistically significant difference in heart rate (bpm) directly after the test. Patients took a mean of 0.8 s (95% CI 0.1–1.5, p = 0.036, Cohen d = 0.4) more than controls to complete the TUG test (Table 2, Figure 1C). Controlling for physical activity frequency, this difference disappeared (βadj = −0.5, 95% CI −1.3–0.3, p = 0.233). One patient scored 2 on the falling tendency scale (very slightly abnormal), while all other patients and controls scored 1 (normal). There was no objective effort measure for the TUG test.

6MWD (m) and TUG test time (s) in patients and controls (A, C), in patients with active and inactive disease (B, D), and correlation between 6MWD and TUG time in patients (E). The box boundaries in A–D represent the 25th–75th percentiles, with the mean value as a horizontal line within the box. n = 29 for patients with active and inactive disease, while n = 59 for patients in total and n = 58 for controls. Correlation is presented as a scatterplot (E), with Pearson r = −0.766, p < 0.001. Regression equation for line of best fit: y = 24.94 − 0.02×. 6MWD: 6-min walk distance; TUG: timed up and go.
The 6MWT and TUG test in patients and controls. Active and Inactive refer to active and inactive disease according to the PRINTO criteria. Continuous, normally distributed variables are presented as mean (SD), while continuous, not normally distributed variables are presented as median (interquartile range).
The patient group consisted of 29 with active and 29 with inactive disease. Patients with active disease walked a mean distance of 60 m shorter (95% CI 20–100, p < 0.004, Cohen d = 0.8) than patients with inactive disease, and physical exercise as well as heart rate were not significantly different in the 2 groups (Table 2, Figure 1B). Although low, on the Borg scale patients with active disease had a higher median score than patients with inactive disease. The TUG time was mean 1.2 s longer (95% CI 0.14–2.28, p = 0.028, Cohen d = 0.6) in patients with active disease compared with those with inactive disease (Table 2, Figure 1D).
Between patients with inactive disease and controls, there was no statistically significant difference in the 6MWD (mean 26.9 m, 95% CI −8.1–62.0, p = 0.130, Cohen d = 0.3) or the TUG time (mean 0.2 s, 95% CI −0.7–1.1, p = 0.657, Cohen d = 0.1) despite 22% more controls than patients with inactive disease exercising ≥ 2–3×/week (p = 0.039). Patients with active disease walked a mean distance of 87 m shorter (95% CI 52–122, p < 0.001, Cohen d = 1.1) than controls, and used mean 1.4 s more (95% CI 0.48–2.33, p = 0.003, Cohen d = 0.7) to complete the TUG test than controls. Controlling for physical activity, both results remained significant (data not shown).
Correlations between the 6MWT, the TUG test, and disease characteristics in patients
In patients, there was a strong correlation between 6MWD and TUG time (r = −0.77, p < 0.001; Figure 1E). No significant difference between the 6MWD and TUG time was found in patients diagnosed before and after 1990 (data not shown), and no significant correlation was found between the test outcomes and disease duration (Table 3). Correlations between outcomes, general characteristics, and disease variables showed similar trends between the 6MWD and TUG time (Table 3). Regarding general characteristics, both test outcomes showed the strongest correlation with SF-36 PCS, and regarding disease-specific variables, DAS muscle and cHAQ/HAQ. In the muscle domain, both test outcomes correlated with CMAS more strongly than MMT-8, and only TUG time correlated with MRI findings. In the lung domain, both test outcomes showed the strongest correlation with HRCT pathology, while only 6MWD correlated with a low DLCO. There was no statistically significant correlation between a low DLCOc and HRCT pathology (r = −0.02, p = 0.865). In the heart domain, no statistically significant correlation was found between the test outcomes and systolic or diastolic dysfunction (long axis strain or early diastolic transmitral flow/early diastolic tissue velocity).
Correlations between 6MWD, TUG time, and general-, disease- and organ-specific variables in patients. Values are Pearson correlation coefficient unless otherwise specified.
The effect of heart, lung, and muscle dysfunction on the 6MWT and the TUG test in patients
Performing linear regression of the 6MWT and the TUG test with lung, heart, and muscle variables in patients, the best fitting model for the 6MWT accounted for 59% of the change in 6MWD (Table 4). Controlling for sex, age, weight, and height, CMAS influenced the 6MWD the most, followed by a low DLCOc and the presence of HRCT pathology. The adjustment factors height and weight also contributed. The best-fitting model for the TUG test explained 48% of the change in TUG time, and after controlling for age and sex, CMAS was the most influential variable, followed by a low FVC. Age was also significantly involved.
The effect of muscle, lung, and cardiac dysfunction on the 6MWT and TUG test in patients with JDM (n = 59), a linear, multivariable regression analysis.
DISCUSSION
In our study on submaximal functional capacity in JDM after longterm followup, we found an impaired 6MWD and TUG time in patients versus controls and in patients with active versus inactive disease, but not in patients with inactive disease versus controls. In patients, both tests correlated with disease activity and SF-36 PCS, while only the TUG test correlated with disease damage. Muscle dysfunction, followed by lung dysfunction, contributed the most to changes in the 6MWD and TUG time. To our knowledge, we are the first to assess the 6MWT and the TUG test in patients with JDM, and to study the effect of disease characteristics and organ involvement on submaximal exercise capacity in JDM.
The representativeness of our JDM cohort was earlier described in detail1 and was comparable to literature on JDM regarding incidence, female predominance, and age at disease onset33. Our controls were drawn randomly from the Norwegian National Registry and matched for age and sex with the patients, and were comparable to the patients with JDM regarding smoking habits, height, and weight. Their 6MWD and TUG time did not correlate with age or sex, which is in accordance with Norwegian 6MWT reference data for those < 50 years of age34. Excluding controls with serious heart and lung disease could be a potential bias; however, only 1 control was excluded because of this, supporting the control group’s resemblance to the general population.
For the 6MWT, our patients walked a mean distance of 57 m shorter than controls. Although small compared with other diseases, this difference is large enough to become clinically visible during everyday physical demands. This is supported by a medium to large effect size (Cohen d = 0.7). The TUG time difference of 0.8 s may reflect more uncertain clinical significance, also supported by a small to medium effect size (Cohen d = 0.4). However, both test results had medium to strong correlation with patient-reported outcomes (SF-36 PCS), adding to the clinical value of both tests. Further, while patients with inactive disease showed only small effect sizes and no statistically significant differences compared with controls, active patients walked a mean distance of 87 m shorter and took a mean 1.4 s longer TUG time. This suggests a subgroup of patients in which the 6MWT and the TUG test may be of even greater importance in clinical followup, and is supported by a strong effect size for the 6MWT (Cohen d = 1.1) and medium to strong effect size for the TUG test (Cohen d = 0.7).
Our study is based on a cross-sectional, single measurement design. Reference equations of single 6MWD measurements have been proposed, but vary significantly between protocols and study populations, making comparison difficult13. The 6MWT and TUG protocols we used differed from standardized guidelines (the American Thoracic Society guidelines for the 6MWT13 and the TUG procedure proposed by Podsiadlo and Richardson20), making the absolute 6MWD and TUG time not directly comparable with other studies. However, by using equal protocols for patients and age- and sex-matched controls, our results are valid.
Muscle dysfunction showed the greatest organ-specific influence of both the TUG test and the 6MWT. This coincides with longterm studies on muscle function in our cohort and other JDM cohorts7,12. CMAS has long been the preferred test in the functional assessment of children with JDM26,35, and it has also been applied to adults7. However, the correlation between CMAS and 6MWD was moderate (Rsp = 0.58), supporting that the measures are not redundant; while CMAS examines muscle function alone, the 6MWT assesses all body systems involved during exercise, including lung and heart function13.
After muscle dysfunction, a low DLCOc made the greatest contribution to changes in 6MWD, followed by the presence of HRCT pathology. However, HRCT pathology and a low DLCOc did not intercorrelate, and neither correlated with CMAS, height, or weight (data not shown), the other contributing variables in the regression analysis. This suggests either independent contributions of the lung findings to the 6MWT results, or underpowered statistics. Studying the same JDM cohort, we have previously shown reduced lung volumes with a normal transfer coefficient suggesting the presence of ultrastructural alveolar membrane changes or pulmonary vascular disease8. However, had there been a common vascular process in the lungs and skeletal muscle explaining both the reduced DLCOc and 6MWD, we would also expect CMAS to correlate with DLCOc. For the TUG test, only a low FVC made a significant pulmonary contribution to the TUG time. Reduced FVC may be a result of smaller lung volumes previously described; however, this is difficult to interpret directly because the TUG test involves a very short procedure not requiring much pulmonary effort.
In the cardiac domain, we found a weak univariate correlation between the 6MWD and ECG pathology; however, being a positive correlation we interpreted this as a nonlogic, coincidental finding (type I error). We have previously shown that diastolic and systolic dysfunction is more frequent in our patients with JDM compared with controls, probably because of cardiac remodeling9,10. The absence of correlations between the 6MWD or TUG time and cardiac dysfunction supports that the latter was of subclinical design. However, the echocardiographic examinations were performed with the patients at rest, and a stress-echo (performed under exercise) might have given a different result.
Other aspects such as muscle strengthening activities and fatigue may influence exercise capacity36,37, but were not measured in our study. Aerobic exercise may also influence exercise capacity38, and was reported through questionnaires as hours and frequency of exercise per week; unfortunately, not in accordance with the World Health Organization recommendations39 because the latter were published after our study was initiated. The control group exercised more frequently than the patients; however, controlling for this in statistical analyses, the 6MWD and TUG time differences persisted between all groups except TUG time between patients and controls, indicating that other factors explain the results. In our cohort, no statistically significant association was found between submaximal exercise capacity and diagnosis before/after 1990 or disease duration; further research is needed to examine whether these outcomes will improve with optimized treatment.
After longterm JDM, we found a shorter 6MWD and longer TUG time compared with controls from the general population, but this was only present in patients with active disease. In patients, both muscle and lung dysfunction influenced the 6MWD and the TUG time. Because the tests reflect activities of daily living and correlate with self-reported health status, they may be important in the followup of patients. However, longitudinal studies on individual test responses as well as thorough validation studies are needed to further evaluate this.
Acknowledgment
We thank Marite Rygg (MD, Professor, Department of Laboratory Medicine, Children’s and Women’s Health, Norwegian University of Science and Technology and St. Olav’s University Hospital, Trondheim) and Ellen Nordal (MD, PhD, University Hospital of North Norway and Department of Clinical Medicine, Arctic University of Norway, Tromsø) for help recruiting patients to this study, and Cathrine Brunborg (MSc, Oslo Center for Biostatistics and Epidemiology, Oslo University Hospital) for statistical supervision.
Footnotes
Supported by the Norwegian Extra Foundation for Health and Rehabilitation (2013/FOM5610) through the Norwegian Rheumatism Association.
- Accepted for publication February 14, 2017.








{kind=link}