
Abstract
Objective. We evaluated the whole-spine computed tomography (CT) findings in patients with synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome to improve our understanding of this rare disease.
Methods. Whole-spine CT images obtained in 69 patients with SAPHO were reviewed. For each individual, a total of 25 vertebrae were evaluated for the distribution of affected vertebrae, CT manifestations of vertebral lesions, symmetry and location of distribution of the lesions on vertebrae, involvement pattern, and narrowing of adjacent intervertebral disc space. Paravertebral ligamentous ossifications, apophyseal joint disorders, and costovertebral joint disorders were also evaluated.
Results. All the 69 patients with SAPHO exhibited abnormalities on whole-spine CT. Sixty-four had vertebral lesions, 52 had paravertebral ossifications, and 47 had both. The vertebral lesions were observed in 441 vertebrae, with a predilection for thoracic spine. The lesions exhibited a mixture of cortical erosion, reactive osteosclerosis of surrounding cancellous bone, and syndesmophyte. They may be confined to the vertebral corner (65.1%) or be extensive, involving the endplate (34.9%). Corner lesions could start in any part of the epiphyseal ring. The lesions were asymmetrically distributed. The affected vertebrae were more consecutively involved in a “kissing” appearance (78.2%). Intervertebral disc spaces were usually normal or mildly narrowed. There were 320 foci of paravertebral ossifications observed, with a predilection for the supraspinous ligament. Paravertebral ossifications were delicate and segmental. Ossifications throughout annulus fibrosis and apophyseal joint were not observed.
Conclusion. Our investigation of the distributional, morphological features and the involvement pattern of spinal lesions in patients with SAPHO demonstrated distinct CT characteristics.
- SAPHO SYNDROME
- DIAGNOSIS
- COMPUTED TOMOGRAPHY
- SPONDYLOARTHRITIS
SAPHO is the acronym for the synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome. Chamot, et al first described a version of it in 19871. It is an evolving concept for unifying several idiopathic dermatological and osteoarthritic disorders2,3. The characteristic dermatological disorders of SAPHO syndrome primarily include palmoplantar pustulosis [PPP; sometimes with concurrent psoriasis vulgaris (PV)] and severe acne (SA; including acne conglobata, acne fulminans, and hidradenitis suppurativa)4. The osteoarthritic abnormalities include mainly synovitis, hyperostosis, and osteitis. The anterior chest wall (ACW), including mainly sternocostal, sternoclavicular, and manubriosternal joints, is the most frequently involved site, followed by the spine and the sacroiliac joints5. Peripheral osteoarthritic involvement may coexist6. Cutaneous lesions may precede, coincide with, or appear after the osteoarthritic disorders5,7. In the absence of cutaneous lesions, osteoarthritic abnormalities may be of great importance for the diagnosis.
Imaging examinations may contribute enormously in demonstrating osteoarthritic disorders in patients with SAPHO, thus facilitating an early diagnosis in time. The classic “bull’s head sign” on 99mTc-MDP bony scintigraphy, which results from the tracer uptake of affected bilateral sternocostal joints, bilateral first sternoclavicular joints, and manubriosternal joint in patients with SAPHO, has been widely accepted and understood. Spinal involvement in SAPHO syndrome has been described3,5,8–17. However, most of those publications are case reports or retrospective studies, with imaging examinations only on clinically symptomatic sites, and the distribution has not been systematically defined3,5,8–17,18–27. Multiplanar computed tomography (CT) has unique advantages over radiographs and bone scintigraphy in demonstrating spinal lesions and their extent through its multiplanar reconstructions and high resolution. To our best knowledge, there has not been a thorough review of whole-spine CT findings in patients with spinal involvement. In our study, we evaluated the whole-spine CT findings in patients with SAPHO syndrome. An overall insight of the extent and CT features of the spinal lesions may give us a relatively comprehensive understanding of SAPHO syndrome.
MATERIALS AND METHODS
Study population
The Institutional Review Board of the Peking Union Medical College Hospital approved this study (research ethics board approval number: ZS-944). Enrollment criteria of our study included the following: (1) ACW involvement diagnosed by 99mTc-MDP bony scintigraphy, (2) characteristic PPP as the only cutaneous manifestation, and (3) a history of or current pain on at least 1 spine level. SAPHO is a unifying concept with unknown etiology. Although the dermatological disorders in SAPHO include PPP, SA, and PV, it remains unclear whether osteoarthritic disorders associated with PPP, SA, and PV are identical. Therefore, we did not include SA and PV in our enrollment criteria. We focused on the most typical subtype of SAPHO syndrome to present its whole-spine CT findings. Between December 2014 and February 2016, a total of 69 patients with SAPHO who fulfilled our enrollment criteria were eventually selected into our study. Informed patient consents were obtained in all the subjects.
The whole-spine CT examinations were prospectively performed in our patients for disease evaluation at the department of radiology in our hospital. Demographic data and clinical features were recorded. Laboratory evaluations including erythrocyte sedimentation rate (ESR), high-sensitivity C-reactive protein (hsCRP), rheumatoid factor (RF), and HLA-B27 were measured within 3 days of CT examination.
CT examinations and reconstructions
The whole-spine CT images (from skull base to the distal coccyx) were obtained in all the subjects using the Toshiba Aquillion ONE 320-detector CT. Relevant examination protocols were presented as follows: tube voltage 120 kV, thickness 2 mm, window width 2000 HU, and window level 400 HU. Sagittal and coronal reconstructions based on the axial images were obtained along the physiological curve of the cervical, thoracic, lumbar, and sacral spine, respectively (thickness 2 mm, window width 2000 HU, window level 400 HU).
Images analysis
A total of 25 vertebrae (from the first cervical vertebra to sacrum) were evaluated for each individual. Two radiologists analyzed the images independently, and the discrepancies were reached to consensus after discussion. The following abnormalities for vertebral lesions were evaluated: distribution on spinal level of affected vertebrae, CT manifestations of vertebral lesions, symmetry and location of the distribution of the lesions on vertebrae, and involvement pattern and narrowing of adjacent intervertebral disc space. Ossifications of paravertebral ligamentous attachments were evaluated and recorded. Apophyseal joint disorders and costovertebral joint disorders were also noted.
CT manifestations were mainly evaluated for cortical bone erosions, sclerosis of the cancellous bone, and syndesmophytes. Syndesmophytes were defined as bone formation associated with vertebral erosive lesions, which extended across the margin of the intervertebral disc. They were vertical and connective to the vertebral edges. Symmetry of the distribution of the lesions on vertebrae was evaluated on coronal reconstructive CT images. Locations of the lesions on vertebrae were evaluated for involving the vertebral corner or the endplate based on a combination of sagittal, coronal, and axial images. Involvement pattern of the affected vertebrae were evaluated as adjacent on both sides of a disc space or isolated. Severe narrowing of adjacent intervertebral disc space was defined as less than one-third the height of adjacent intervertebral disc height.
Paravertebral ligamentous ossification began at a distance from the vertebral body and intervertebral disc.
Apophyseal joint disorders and costovertebral joint disorders included the following: poorly defined bony erosions, reactive subchondral bone formation, joint space narrowing, osseous fusion, and capsular ossification.
RESULTS
Demographic and clinical characteristics
There were 69 patients with SAPHO (55 women and 14 men) included in our study. The mean age at diagnosis was 45.7 years and the mean age at symptom onset was 41.5 years. The mean disease duration was 3.9 years. PPP preceded the onset of osteoarticular lesions in 55.1% of the patients, was concomitant in 23.2%, and appeared after osteoarticular symptoms in 21.7%. None of our patients were diagnosed with inflammatory bowel disease (IBD). The ESR (normal range 0–20 mm/h) and hsCRP (normal range 0–3 mg/l) were increased in 71.0% and 78.3% of patients, respectively. None of our patients were RF-positive. Only 1.4% of our patients were HLA-B27–positive. The details are provided in Table 1.
Demographic and clinical characteristics of the 69 patients with SAPHO in our study. Values are the no. patients/total no. patients (%) unless otherwise indicated; only positive associations are expressed.
Whole-spine CT findings
All the 69 patients with SAPHO exhibited some abnormalities on whole-spine CT. Sixty-four out of the 69 patients had vertebral lesions, 52 had paravertebral ossifications, and 47 had both. No apophyseal joint disorders and costovertebral joint disorders were observed. Therefore, whole-spine CT abnormalities of patients with SAPHO in our study could be classified into 2 categories: vertebral lesions and paravertebral ligamentous ossifications (Figure 1, Figure 2, and Figure 3).

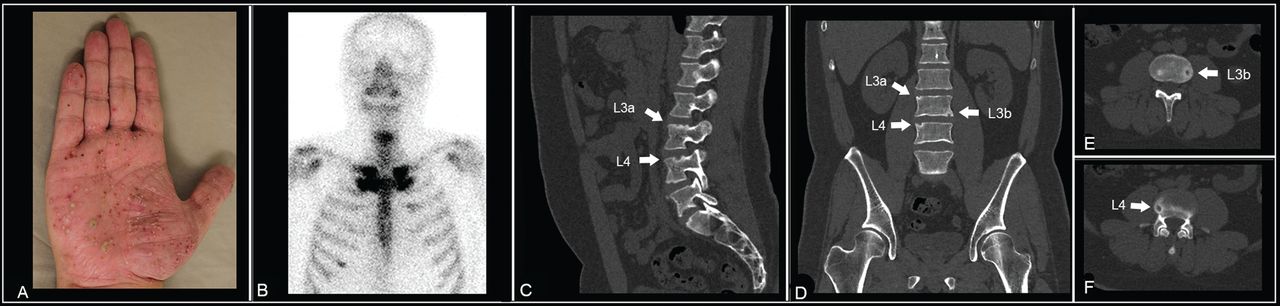
Clinical and multiplanar CT images of a 36-year-old male patient with SAPHO (with a disease duration of 1.3 yrs) showed dermatological and osteoarthritic lesions. (A–B) Pustules and red papules on the palm as well as “bull’s head sign” on 99mTc-MDP bony scintigraphy were shown. (C–F) Sagittal, coronal, and axial CT images of the lumbar spine clearly depicted the asymmetrically distributed lesions involved in a separate pattern (arrows). The lesions were confined to the vertebral corners and manifested as cortical erosions and osteosclerosis in surrounding cancellous bone. CT: computed tomography; SAPHO: synovitis, acne, pustulosis, hyperostosis, and osteitis (syndrome).
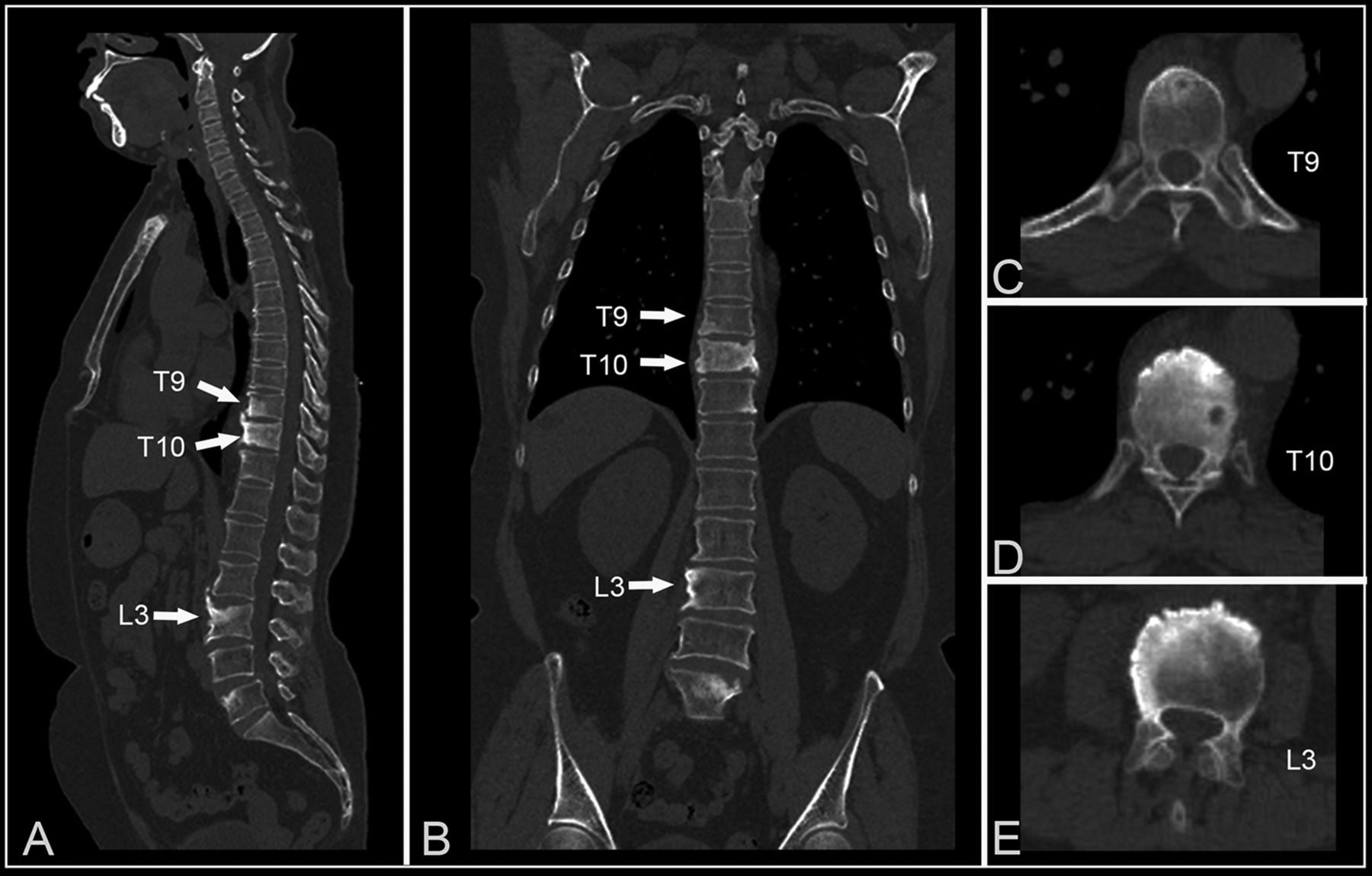
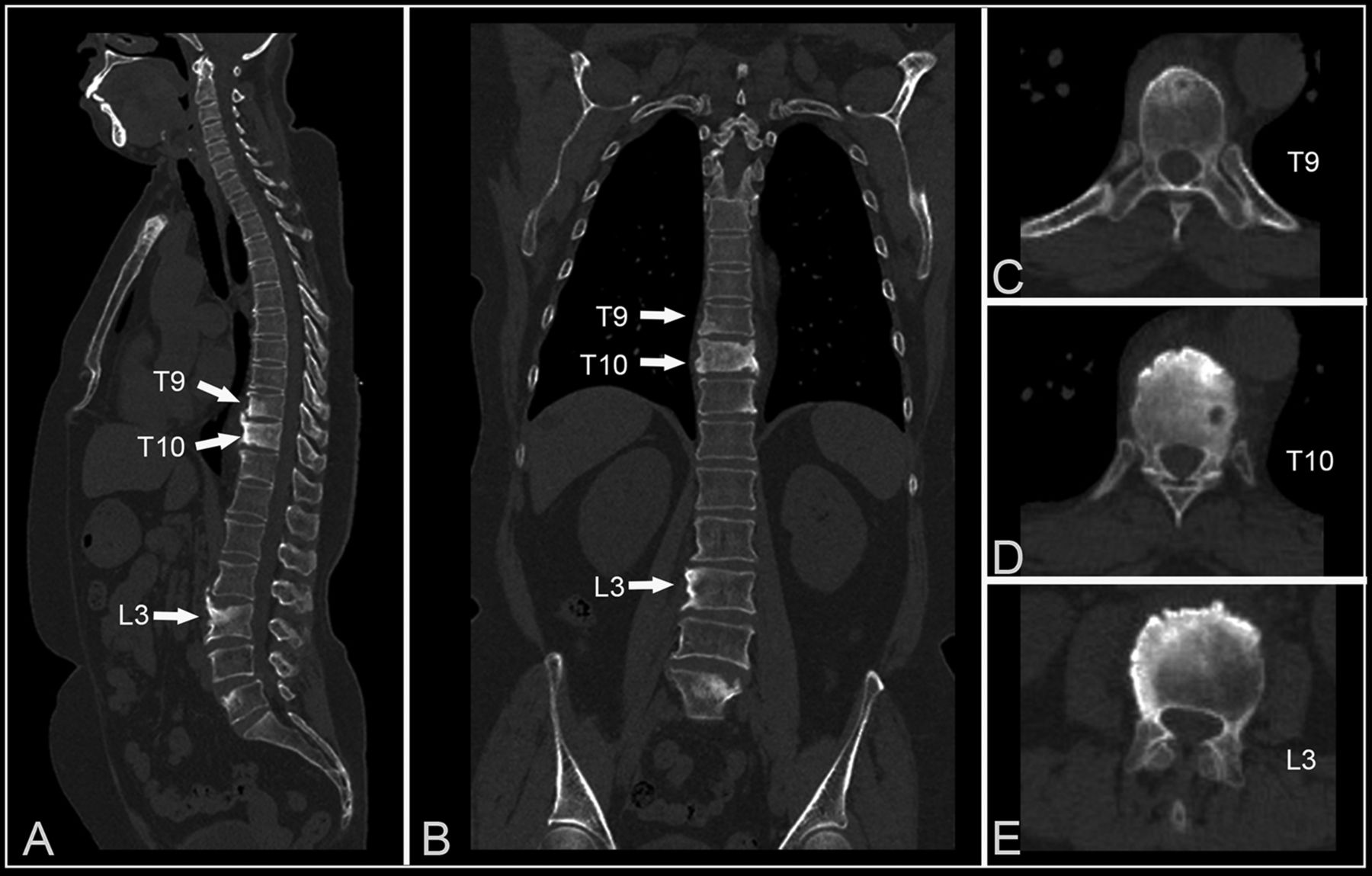
Clinical and multiplanar CT images of a 50-year-old female patient with SAPHO (with a disease duration of 4.1 yrs) showed osteoarthritic lesions. Spinal disorders were shown in (A) sagittal, (B) coronal, and (C–E) axial CT images. Multiple vertebrae were affected by the lesions, which involved both vertebral corners and endplates in a consecutive pattern. The lesions manifested as cortical erosions and osteosclerosis in surrounding cancellous bone, with the formation of coarse syndesmophyte. CT: computed tomography; SAPHO: synovitis, acne, pustulosis, hyperostosis, and osteitis (syndrome).
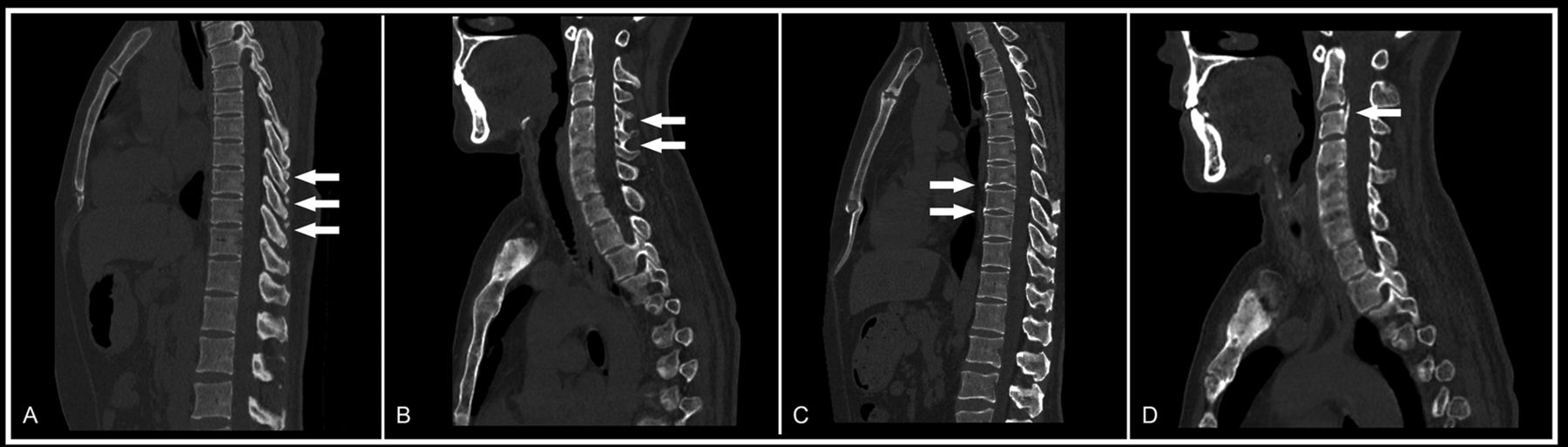
Shown are ossifications of (A) the supraspinous ligament (arrows), (B) the interspinous ligament (arrows), (C) the anterior longitudinal ligament (arrows), and (D) the posterior longitudinal ligament (arrow).
Vertebral lesions
Overall, 441 vertebrae were involved in the 64 patients. Among these vertebrae, the cervical spine was involved in 15.2% (67/441), the thoracic spine in 39.9% (176/441), the lumbar spine in 36.7% (162/441), and the sacrum in 8.2% (36/441; Figure 4A).

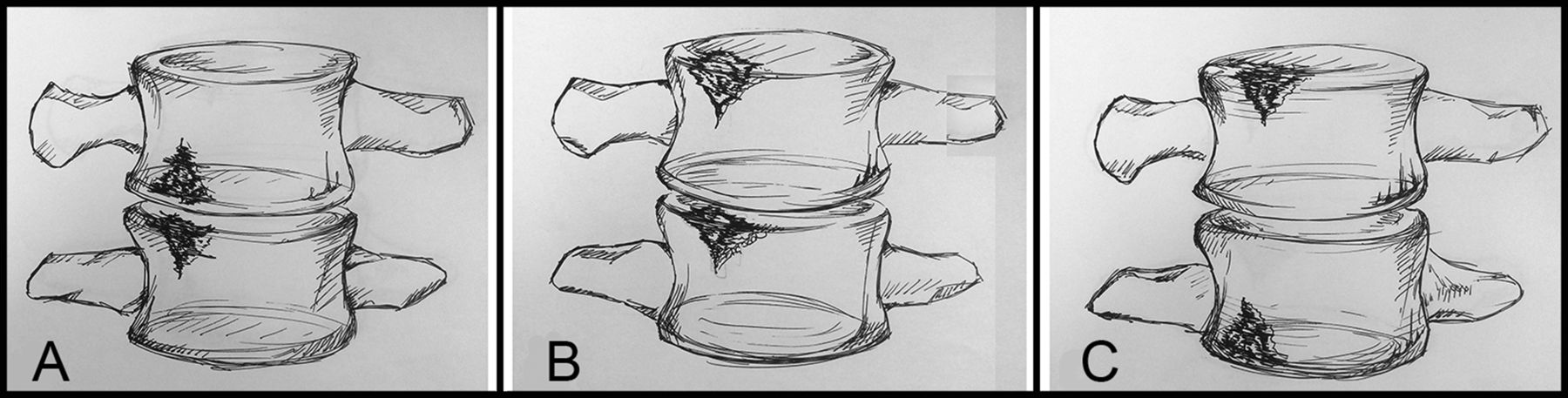
(A) Of the 64 patients with SAPHO who exhibited vertebral lesions, 441 vertebrae were affected. (B) Schematic diagram showing a vertebral lesion confined to the vertebral corner. (C) Schematic diagram showing a vertebral lesion involving in both the vertebral corner and endplate. SAPHO: synovitis, acne, pustulosis, hyperostosis, and osteitis (syndrome).
We found that patients with SAPHO exhibited a mixture of several common CT features, which included focal cortical erosion, reactive osteosclerosis of surrounding cancellous bone, and syndesmophytes. While all these lesions were distributed asymmetrically (Figure 1 and Figure 2), 65.1% (287/441) of the vertebrae were affected by lesions that were confined to the vertebral corner (Figure 4B), and 34.9% (154/441) by lesions involving both a vertebral corner and the adjacent endplate (Figure 4C). Corner lesions could start in any part of the epiphyseal ring of the vertebral endplate. As for the involvement pattern, 78.2% (345/441) of the affected vertebrae were adjacent on both sides of a disc space as a “kissing” appearance (Figure 5A) and 21.8% (96/441) were isolated (Figures 5B–C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic diagram for the involvement patterns of spinal lesions in SAPHO syndrome are shown. (A) The affected vertebrae were involved consecutively as a “kissing” appearance. (B–C) The affected vertebrae were involved separately. SAPHO: synovitis, acne, pustulosis, hyperostosis, and osteitis (syndrome).
Intervertebral disc spaces adjacent to affected vertebrae were usually normal or mildly narrowed (more than two-thirds the height of adjacent intervertebral disc space), except for 1 patient with 3 severely narrowed intervertebral disc spaces.
Paravertebral ligamentous ossifications
Overall, 320 foci of ligamentous ossifications were observed in 52 out of the 69 patients. Forty-seven out of these 52 patients had associated vertebral lesions, while 5 had only paravertebral ossifications. Of the paravertebral ossifications, 63.4% (203/320) involved the supraspinous ligament, 31.6% (101/320) the anterior longitudinal ligament, 3.4% (11/320) the interspinous ligament, and 1.6% (5/320) the posterior longitudinal ligament.
On CT images, the ossifications of the paravertebral ligaments were delicate and segmental (Figure 3).
DISCUSSION
In our study, we evaluated the whole-spine CT findings in 69 patients with SAPHO syndrome. Our demographic data were not meaningful for epidemiologic studies; however, it confirmed the currently established saying that SAPHO is a syndrome mainly affecting middle-aged adults with a female predominance12,13,18–27,28,29. ESR and hsCRP were also elevated in our patients, as previously reported13,23,25,30. Our results also confirmed the lack of association of RF and HLA–B27 antigen21,22,23,27, the latter of which was present in 90% and 56% of the ankylosing spondylitis (AS) and axial psoriatic arthritis populations, respectively21,31.
Because of its high spatial resolution and 3-D capabilities with multiplanar reconstructions, whole-spine CT allows the depiction of early vertebral lesions in any spinal segment. It was reported that spinal lesions had a slight predilection for either the lumbar spine (Laredo, et al10) or the cervical spine (Takigawa, et al13). In contrast, our study found that the thoracic spine was the most frequently involved spinal segment, with a prevalence of 39.9%. This should be explained by the segmental spinal imaging examinations in previous retrospective studies10,13, in which only the painful spinal segment was imaged and the asymptomatic spinal segment was neglected, which resulted in a lower prevalence. The whole-spine CT examination in our study could provide an overall assessment of the whole spine and detect asymptomatic lesions ignored by patients.
In our study, patients with SAPHO exhibited a mixture of several common CT features: focal cortical erosion, surrounding reactive osteosclerosis, and subsequent nonmarginal syndesmophytes. However, the vertebral corner, the characteristic location of SAPHO syndrome, could be a useful diagnostic clue.
Many challenges remain regarding how to interpret the spinal lesions in SAPHO syndrome. Only 8 articles emphasizing this aspect were found in Medline, consisting of 4 retrospective studies with 8–19 cases and 8 review articles3,5,9,10,12,13,14,32. Earwaker and Cotten proposed in their review article that the nonspecific spondylodiscitis, which originated from vertebral body and spread to the intervertebral disc, may be the initial manifestation of spinal lesions in SAPHO syndrome3. However, Laredo, et al said in their retrospective study of 12 patients that inflammatory enthesitis that resulted in corner lesions with subsequent local spread to surrounding endplate and intervertebral disc may be the pathological process10. In our study, the results that all the endplate lesions were accompanied by corner lesions without clear boundary, highly agreed with the theory of Laredo, et al that focal lesion of the vertebral corner was the trigger of the pathogenic process10. However, in contrast with the anterior and posterior corner locations of spinal lesions described by Laredo, et al, our results showed that the corner lesions could start in any part of the epiphyseal ring of the vertebral endplate. Therefore, we speculated that the corner lesions were disorders at the junction of the outer fibers of the annulus fibrosis and vertebral epiphyseal ring. Anatomically, the outer fibers of the annulus fibrosis could be further classified into Sharpey’s fiber and outer annulus fibers33. Based on this, 2 theories regarding the pathology were proposed: (1) inflammatory enthesitis and (2) reactive osteitis elicited by slow microorganism infection. For the first hypothesis, in agreement with Laredo, et al, the insertion of Sharpey’s fiber on vertebral epiphyseal ring was a structure defined as enthesis, and inflammatory enthesitis was considered10. For the latter, a poor blood circulation in the special anatomical site, which may result in a susceptibility to infection, could be suspected. Unfortunately, no biopsy of spinal lesions at different stages had been performed and further investigations are still needed to validate our hypotheses.
Our study found that lesions involved several adjacent vertebrae on both sides of a disc space in a “kissing” appearance with a percentage of 78.2% (Figure 5A). This was similar to the semicircular pattern of contiguous vertebral body involvement with a percentage of 63% in the study performed by McGauvran, et al11. This finding is suggestive of a local spread of the lesions.
The paravertebral ligamentous ossifications mostly occurred on the supraspinous ligament with a prevalence of 63.4%. As shown in Figure 3, the lesions in our patients were moderate and segmental, located away from vertebral lesions and intervertebral disc, which were different from nonmarginal syndesmophytes or enthesophytes described in previous literature32. This new observation may result from the higher resolution of multiplanar CT and the overall extent of the whole spine. Such findings may also indicate that the vertebral disorders could contribute to a higher incidence of paravertebral ligamentous ossifications.
Because of the complex CT manifestations described above, many diseases should be taken into consideration for differential diagnosis. When lesions involved adjacent vertebrae, infectious diseases were strongly considered. However, in patients with SAPHO, more than 2 adjacent endplates were usually involved, and intervening disc spaces were usually preserved or only mildly narrowed. Also, paravertebral abscesses were missing in patients with SAPHO. Involvement of multiple vertebrae with a mixed, lytic, and sclerotic appearance suggested the diagnoses of vertebral metastases or bone marrow disorders such as lymphoma and multiple myeloma34. In such instances, the vertebral corner, which was the characteristic location of SAPHO syndrome, could be a valuable clue for differentiation. Axial spondyloarthritis may exhibit several CT findings of SAPHO syndrome including enthesitis, spondylodiscitis, and paravertebral ossifications. However, the corner lesions in AS were associated with the formation of delicate and marginal syndesmophytes subsequently. Also, the paravertebral ligamentous ossifications in AS were diffuse, and occurred predominantly on the posterior ligament35,36. Finally, degenerative changes should also be taken into consideration with respect to the older age of patients. In contrast with the predominance on thoracic spine in SAPHO, the spinal degeneration usually occurred at the cervical and lumbar spine, with obvious disc space narrowing. However, in some cases, it may be difficult to distinguish degenerative disc disease with occasional flares of endplate inflammation and spinal involvement in patients with SAPHO.
There were some limitations to our study. First, the patients with SAPHO in our study had both PPP and ACW involvement, as well as past or current pain on at least 1 spine level. We also excluded cases diagnosed with chronic recurrent multifocal osteomyelitis and IBD. The enrollment criteria resulted in the absence of cases with other cutaneous manifestations (SA and PV), cases without ACW involvement, and cases with negative spinal symptoms. However, SAPHO syndrome was an evolving concept for unifying several idiopathic dermatological and osteoarthritic disorders with unknown etiology2,3. Therefore, we selected the typical subtype from our SAPHO cohort37 to clarify the spinal disorders associated with SAPHO syndrome more clearly. The second shortage was the lack of control group in our study, because the diagnostic value of the CT findings must be tested in a series of patients with either vertebral SAPHO syndrome and other spinal disorders such as vertebral infection, degenerative disease, metastatic disease, and bone marrow diseases. Further, sacroiliac joint involvement was not discussed in our study. Finally, the exposure to a relatively high radiation of the whole-spine CT examination should also be taken in consideration.
Our investigation of the distributional, morphological features and the involvement pattern demonstrated the distinct CT characteristics of spinal lesions in patients with SAPHO. The location of vertebral corner and “kissing” involvement pattern may be conceived as new diagnostic signs for SAPHO. They may be involved in the process of diagnosis and differential diagnosis. Further studies are still needed to get a better understanding of the rare disease.
Acknowledgment
The authors thank all the patients with synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome involved in this study. We also thank the National Natural Science Foundation of China for supporting this study.
Footnotes
Supported by grants from the National Natural Science Foundation of China (81271545), the Scientific Research Foundation for the Returned Overseas Chinese Scholars, and the Science and Technology Foundation for the Selected Returned Overseas Chinese Scholars.
- Accepted for publication January 13, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.