
Abstract
Objective. We used the 28-joint Disease Activity Score (DAS28) and the European League Against Rheumatism Sjögren’s Syndrome Disease Activity Index (ESSDAI) articular domain to assess the effect of rituximab (RTX) and abatacept (ABA) on articular involvement in primary Sjögren syndrome (pSS).
Methods. Patients with pSS treated with RTX (n = 18) or ABA (n = 13) and having a DAS28 erythrocyte sedimentation rate (ESR)/C-reactive protein (CRP) level ≥ 3.2 at baseline were selected. Generalized estimating equations were used to analyze the DAS28 and ESSDAI articular domain over time.
Results. In the RTX group, DAS28-ESR/CRP decreased significantly up to 48 weeks. In the ABA group, DAS28-ESR/CRP decreased significantly up to 24 weeks. DAS28 correlated significantly with ESSDAI articular domain.
Conclusion. DAS28 is useful to evaluate the effect of biologicals on articular involvement in patients with pSS.
- PRIMARY SJÖGREN SYNDROME
- ARTICULAR INVOLVEMENT
- 28-JOINT DISEASE ACTIVITY SCORE
- ESSDAI ARTICULAR DOMAIN
- BIOLOGICALS
Arthralgia and arthritis are common features of disease activity in patients with primary Sjögren syndrome (pSS), with prevalence rates of 45%–50% and 15%–35%, respectively1,2.
In a large cohort study of 921 Spanish patients, articular involvement was found to be the most prevalent extraglandular manifestation of pSS3.
The Disease Activity Score of 28 joints (DAS28) has been developed and validated to monitor disease activity including swollen joint count (SJC) and tender joint count (TJC) in patients with rheumatoid arthritis (RA)4. Although the DAS28 is validated for RA only, it is also used in other autoimmune diseases5. Patients with pSS with articular involvement could benefit from the therapies used in patients with RA. Therefore, it is clinically relevant to have a disease activity index that can be used in both diseases, to compare treatment effects.
The European League Against Rheumatism Sjögren’s Syndrome Disease Activity Index (ESSDAI) has been developed and validated to measure systemic disease activity in patients with pSS6. The ESSDAI includes 12 domains, of which the articular domain is based on arthralgia in combination with morning stiffness and on the SJC from DAS28, but includes only 3 activity levels7.
In our study, we used the DAS28 and ESSDAI articular domain to assess the effect of rituximab (RTX) and abatacept (ABA) treatment on articular involvement in patients with pSS.
MATERIALS AND METHODS
Patients with pSS who received either RTX or ABA within our previously reported prospective open-label studies8,9 were selected based on DAS28–erythrocyte sedimentation rate (ESR)/C-reactive protein (CRP) ≥ 3.2 at baseline, to allow assessment of improvement in disease activity after treatment. Of the 28 patients treated with RTX (1000 mg, days 1 and 15)8, 18 had baseline DAS28-ESR ≥ 3.2, and 11 patients had DAS28-CRP ≥ 3.2. These patients were evaluated at baseline and at weeks 16, 24, 36, 48, and 60 after treatment. Of the 15 patients treated with ABA (infusions ∼10 mg/kg of body weight, days 1, 15, and 29 and every 4 weeks thereafter)9, 13 had baseline DAS28-ESR ≥ 3.2, and 11 DAS28-CRP ≥ 3.2. These patients were evaluated at baseline and at weeks 4, 12, 24 (while taking treatment), and 36 and 48 weeks (while not taking treatment).
The patients with pSS with DAS28-ESR/CRP < 3.2 at baseline were excluded from this analysis because those patients had no articular involvement at baseline and thus could not show improvement from RTX or ABA treatment (of note: none of those patients developed articular involvement when receiving RTX or ABA treatment).
All patients fulfilled the revised American-European Consensus Group criteria for pSS10 and were negative for anticitrullinated protein antibodies.
At all visits, the number of swollen joints (SJC; range 0–28), number of tender joints (TJC; range 0–28), ESR, CRP, and patient visual analog scale (VAS) regarding general health were routinely recorded to calculate the DAS28-ESR and DAS28-CRP.
The articular domain of the ESSDAI (range 0–3) was scored as 0 (no activity: absence of currently active articular involvement); 1 (low activity: arthralgias in hands, wrists, ankles, and feet accompanied by morning stiffness > 30 min); 2 (moderate activity: 1–5 synovitis of 28 SJC); or 3 (high activity: ≥ 6 synovitis of 28 SJC)6,7.
For this study, ethics board approval was not required.
Statistical analysis
Generalized estimating equations (GEE) were used to analyze the DAS28-ESR, DAS28 components, and ESSDAI articular domain over time within both treatment groups. In the RTX group, followup data up to 60 weeks were used to assess change over time compared to baseline. In the ABA group, on-treatment data up to Week 24 were used to assess change over time compared to the baseline and off-treatment data up to Week 48 that were used to assess change over time compared to Week 24. Further, the correlation between DAS28 and the ESSDAI articular domain over time was analyzed using GEE.
Internal responsiveness analysis was performed for DAS28-ESR at Week 24 in both RTX and ABA treatment groups using standardized response mean (SRM) as described by Husted, et al11. SRM was calculated as the mean change in score between baseline and Week 24 divided by the SD of the change in score. SRM < 0.5 was considered small, 0.5–0.8 moderate, and > 0.8 large12,13.
The same methodology was used to perform the additional analysis of DAS28-CRP in the RTX (n = 11) and ABA (n = 11) treatment groups. Statistical analysis was performed with IBM SPSS Statistics 20 (SPSS). P < 0.05 was considered statistically significant.
RESULTS
At baseline, the median DAS28-ESR scores were 3.7 [interquartile range (IQR) 3.4–5.0] and 4.5 (IQR 3.9–5.9) in the selected patients from the RTX and ABA treatment studies, respectively. Patients’ baseline characteristics are shown in Supplementary Table 1, available with the online version of this article.
In the RTX group, no patients were taking additional disease-modifying antirheumatic drug therapy during the study period. In the ABA group, 2 patients were briefly treated with prednisolone because of photosensitivity of the skin. One of them had to start with hydroxychloroquine to control the skin manifestations.
Following RTX treatment, DAS28-ESR decreased significantly up to 48 weeks and had returned to baseline values at Week 60 (Figure 1A). In ABA-treated patients, DAS28-ESR decreased significantly up to 24 weeks and had returned to baseline values at Week 36 (Figure 1B). Comparable results were found for DAS28-CRP (Figure 1C and 1D). The decrease of disease activity assessed with SJC and TJC was significant over time in both RTX and ABA treatment groups, with maximum effect at Week 24 (Figure 2).
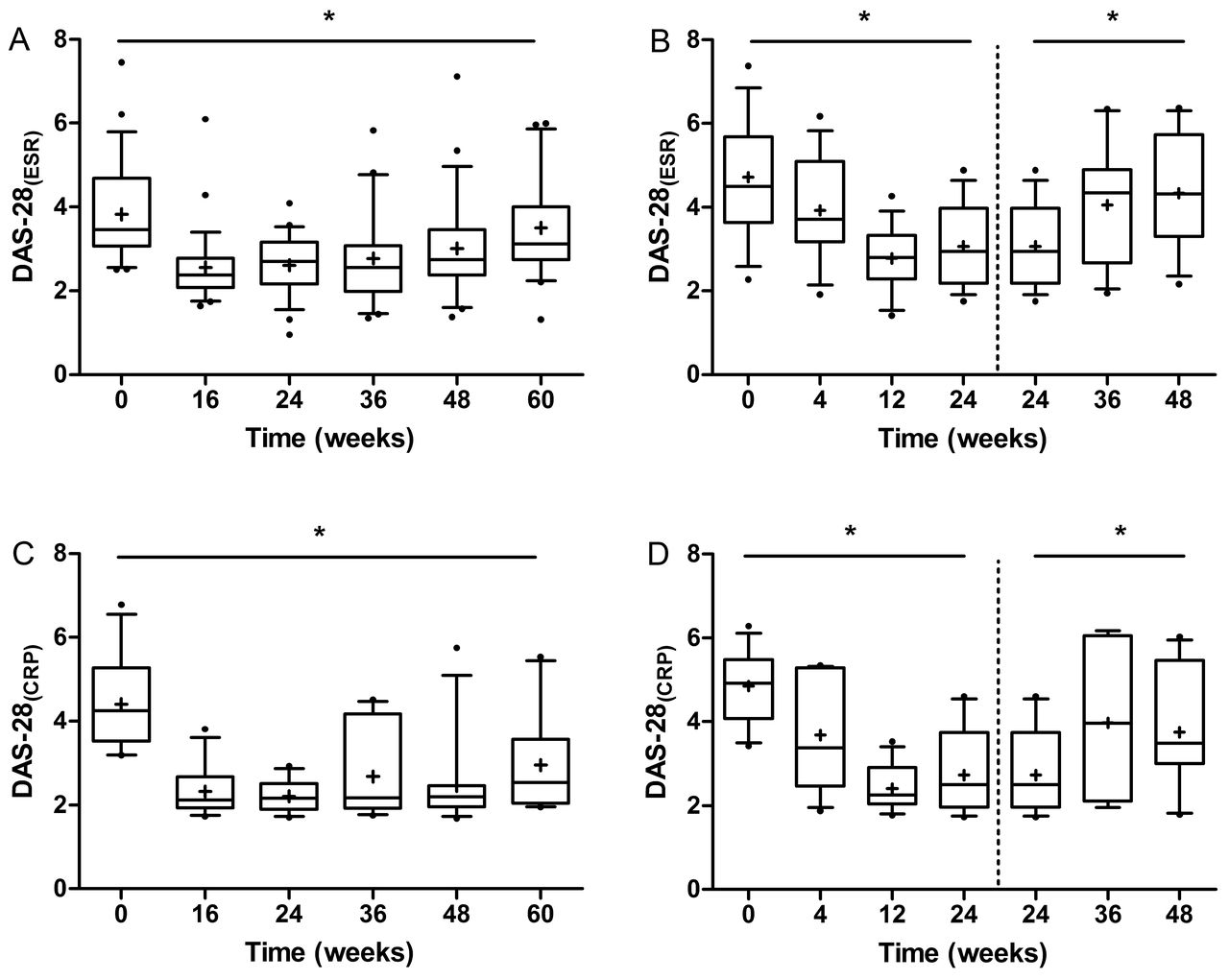
Changes over time of DAS28-ESR in patients with either RTX (A; n = 18) or ABA (B; n = 13) treatment and of DAS28-CRP with either RTX (C; n = 11) or ABA (D; n = 11) treatment. Boxes indicate medians with interquartile ranges; plus signs indicate means; whiskers indicate 1.5 × the interquartile distances. Small dots indicate outliers. * p < 0.05. DAS28: 28-joint Disease Activity Score; ESR: erythrocyte sedimentation rate; RTX: rituximab; ABA: abatacept; CRP: C-reactive protein.

{kind=link}
{kind=link}
Changes over time of TJC and SJC counts in patients with either RTX (A and B; n = 18) or ABA (C and D; n = 13) treatment. Boxes indicate medians with interquartile ranges; plus signs indicate means; whiskers indicate 1.5 × the interquartile distances. Small dots indicate outliers. * p < 0.05. TJC: tender joint count; SJC: swollen joint count; RTX: rituximab; ABA: abatacept.
Regarding the other components of the DAS28, ESR showed a significant decrease over time in the RTX group, again with maximum effect at Week 24. In the ABA group, there was no significant decrease of ESR over time. VAS general health decreased significantly over time until Week 60 in the RTX group, whereas no significant change over time was found for VAS general health in the ABA group.
The articular domain of the ESSDAI decreased significantly over time with maximum effect at Week 24 in both treatment groups (Table 1). The proportion of patients with ESSDAI articular domain score ≥ 1 decreased significantly from 38.9% at baseline to 5.6% at Week 24 after RTX treatment and from 92.4% at baseline to 23.1% at Week 24 during ABA treatment.
Proportion of patients with pSS per category of ESSDAI articular domain during treatment with rituximab (RTX; n = 18) or abatacept (ABA; n = 13). Values are presented as n (%) of patients.
During RTX or ABA treatment, there were no patients with an increase in DAS28-ESR/CRP or ESSDAI articular domain score between baseline and Week 24.
GEE analysis over time revealed that DAS28 was significantly associated with the articular domain of the ESSDAI in the RTX group [0–48 weeks: B (regression coefficient) = 1.203, p < 0.001] and in the ABA group (0–24 weeks: B = 0.942, p < 0.001; 24–48 weeks: B = 0.853, p < 0.001).
SRM for DAS28-ESR and DAS28-CRP at Week 24 versus baseline were large: 1.45 and 1.83 in the RTX group, respectively, and 1.37 and 1.81 in the ABA group.
DISCUSSION
To our knowledge, this is the first analysis using DAS28 to assess the articular involvement in patients with pSS. These patients have several clinical and laboratory characteristics that are also rather common in RA, such as arthralgia and arthritis, vasculitis, pulmonary involvement, peripheral neuropathy, and decreased complement levels. These are important components of disease activity and should be considered in the clinical assessment and followup of patients with pSS and RA. The ESSDAI is a validated tool to evaluate these systemic disease manifestations and responses to treatment in pSS. However, there is a need to assess in more detail several specific extraglandular manifestations and individual domains or groups of domains of the ESSDAI, e.g., articular involvement, to provide target therapies. It will be impossible to develop and validate new diagnostic tools for each extraglandular manifestation of pSS. Therefore, some tools used outside of pSS can be validated for clinical trials in patients with pSS. We showed that DAS28-ESR and DAS28-CRP are sensitive enough to show the effect of treatment over time with biological therapies. Therefore, we propose to use DAS28 as an additional tool to assess articular involvement in pSS in clinical trials and to extrapolate the dosages of therapeutics from RA treatment experiences to pSS, because RA is a model disease in the development of new treatments for autoimmune diseases.
It is important to mention that the improvement in articular involvement in our patients with pSS, measured by DAS28, was dependent not only on ESR/CRP or VAS global health. SJC and TJC components of DAS28 contributed most to the change over time. Moreover, the DAS28 has comparable course and significant correlation over time with the articular domain of the ESSDAI. Baseline characteristics of our 2 open-label studies were different, mainly because of differences in inclusion criteria8,9. In the RTX study we found less articular involvement than in the ABA study. Nevertheless, as in the ABA group, the decrease in articular involvement was statistically significant in the RTX group, but VAS and ESR/CRP also contributed to the decrease of DAS28 over time. Therefore, we suggest that DAS28 should be interpreted in patients with pSS in the same way as in patients with RA. Patients with pSS without arthralgia or arthritis should not be evaluated with DAS28, because DAS28 is meaningless in that setting (TJC and SJC will not be evaluated, only VAS and ESR).
The DAS28 is useful not only in patients with RA but also in patients with pSS to evaluate the effect of biological therapies on articular involvement.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
The investigator-driven studies were financially supported by Roche, Woerden, the Netherlands, and Bristol Myers Squibb, Rueil Malmaison, France, which also supplied study medication.
- Accepted for publication November 16, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.