

Abstract
Objective. To examine the 2-year disease course in patients with undifferentiated arthritis (UA) focusing on fulfillment of the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) rheumatoid arthritis (RA) classification criteria.
Methods. Data were provided by the Norwegian Very Early Arthritis Clinic study, which included patients presenting with ≥ 1 swollen joint of ≤ 16 weeks’ duration. UA was defined as patients not fulfilling the 2010 ACR/EULAR RA criteria and who did not have a clinical diagnosis other than RA at baseline. The main outcome was fulfillment of the 2010 RA criteria. Secondary outcomes were disease-modifying antirheumatic drug (DMARD) use, resolution of synovitis without use of DMARD during followup, and final clinical diagnosis.
Results. We included 477 patients with UA of whom 47 fulfilled the 2010 ACR/EULAR RA criteria during followup (UA-RA) and 430 did not (UA–non-RA). Of the UA-RA patients, 70% fulfilled the criteria within the first 6 months. UA-RA patients were older, more often positive for rheumatoid factor and anticitrullinated protein antibodies, female, and ever smokers, and they more often presented with polyarticular arthritis, small joint involvement, and a swollen shoulder joint. During followup, 53% of UA-RA patients vs 13% of UA-non-RA patients used DMARD (p < 0.001). Overall, 71% of patients with UA achieved absence of clinical synovitis at final followup without use of DMARD. The most frequent final clinical diagnosis was UA (61%).
Conclusion. Only 9.8% of patients with UA fulfilled the 2010 RA criteria during 2-year followup. Small joint involvement and swollen shoulder joint were among the factors associated with RA development. In two-thirds of patients with UA, the arthritis resolved without use of DMARD.
A challenge in the care of patients with inflammatory arthritis is that the symptoms and clinical findings at presentation are often nonspecific, and thus it is not possible to make a diagnosis at presentation for all patients. In such cases the term undifferentiated arthritis (UA) is often used. However, there is no consensus on exactly how to define concepts such as early arthritis and UA, which makes it difficult to compare the characteristics of different patient cohorts. This may explain why the proportion of patients denoted UA in early arthritis cohort studies has ranged from 23% to 81%, with most reporting a proportion around 30%1. Studies have shown that about one-third of all patients with UA eventually will progress to rheumatoid arthritis (RA), while about 40%–50% will experience self-limiting disease1. However, these estimates are uncertain and influenced by the study setting2.
To ensure that those who may benefit from early intervention receive appropriate treatment, as well as to prevent overtreatment, the ability to identify the patients with UA who will progress to RA is important.
The main reason for developing the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) RA classification criteria (2010 RA criteria) was to facilitate early identification of patients with RA3. A consequence of the new criteria might be that the group of patients defined as UA has milder symptoms and more heterogeneous disease compared to patients with UA defined by the 1987 ACR criteria4,5. Nonetheless, not all patients who are subsequently diagnosed with RA fulfill the 2010 RA criteria at presentation. Krabben, et al, observed that 24% of patients with UA not identified by the 2010 RA criteria at baseline fulfilled the 1987 ACR criteria during the first year of followup6. Limited data are available on how many of the patients not fulfilling the 2010 RA criteria at presentation do so during followup7,8, and more knowledge is needed about the factors predicting transition from early UA to RA according to the 2010 RA criteria9.
The purpose of our study was to examine the 2-year disease course in patients with very early UA according to the 2010 RA criteria, with the main outcome being subsequent fulfillment of the 2010 RA criteria, and secondary outcomes being use of disease-modifying antirheumatic drug (DMARD), resolution of clinical synovitis without use of DMARD during followup, and final clinical diagnosis.
MATERIALS AND METHODS
Setting
The current analyses were based on data from The Norwegian Very Early Arthritis Clinic (NOR-VEAC) study, a prospective observational study with 6 participating hospitals in the southeastern part of Norway. Patients were included between 2004 and 2010. The purpose was to examine the disease course in patients with very early inflammatory arthritis, i.e., ≤ 16 weeks. The cohort included 1118 patients (age 18–75 yrs) presenting with at least 1 clinically swollen joint. Patients with joint swelling due to trauma, osteoarthritis (OA), crystal arthritis, or septic arthritis were excluded. Patients were followed for 2 years with study visits at baseline and after 3, 6, 12, and 24 months. Referral from primary care physicians was by telephone or letter, and patients referred to the early arthritis clinic study were guaranteed a consultation at their local rheumatology department within 14 days.
Written informed consent was obtained from all participants. The study was approved by the Regional Ethics Committee of Southern Norway (562-04173/143-07-04173) and the Data Inspectorate.
Data collection
The comprehensive data collection has been described in detail elsewhere10. It included demographics, disease characteristics, comorbidities, use of medication, 68 swollen joint counts (including hip joints if the investigator suspected arthritis) and 28 tender joint counts (68-SJC and 28-TJC, respectively), erythrocyte sedimentation rate (ESR; mm/h), C-reactive protein (CRP; mg/l) and a range of patient-reported outcome measures. We applied the ACR Board of Directors and the EULAR Executive Committee’s definition of large and small joints3. We calculated the 28-joint Disease Activity Score (DAS28) based on 28-SJC, 28-TJC, patient global visual analog scale (VAS), and ESR11.
Serum was frozen and stored at −70°C and used to analyze anticitrullinated protein antibodies (ACPA; Inova Diagnostics) and anticyclic citrullinated peptide antibodies (anti-CCP2; Phadia), and IgM and IgA rheumatoid factor (RF; in-house ELISA). Cutoffs for ACPA positivity according to Inova Diagnostics and Phadia were defined as ≥ 25 U/ml and ≥ 10 U/ml, respectively, and RF IgM and IgA ELISA positivity were defined as ≥ 25 U/ml. For application of the 2010 ACR/EULAR classification criteria, an elevated CRP was defined as CRP ≥ 4 mg/l, and the corresponding cutoffs for ESR were ≥ 12 mm/h for men and > 17 mm/h for women (the national user manual for clinical biochemistry was used to determine these cutoffs).
Patient selection and outcomes
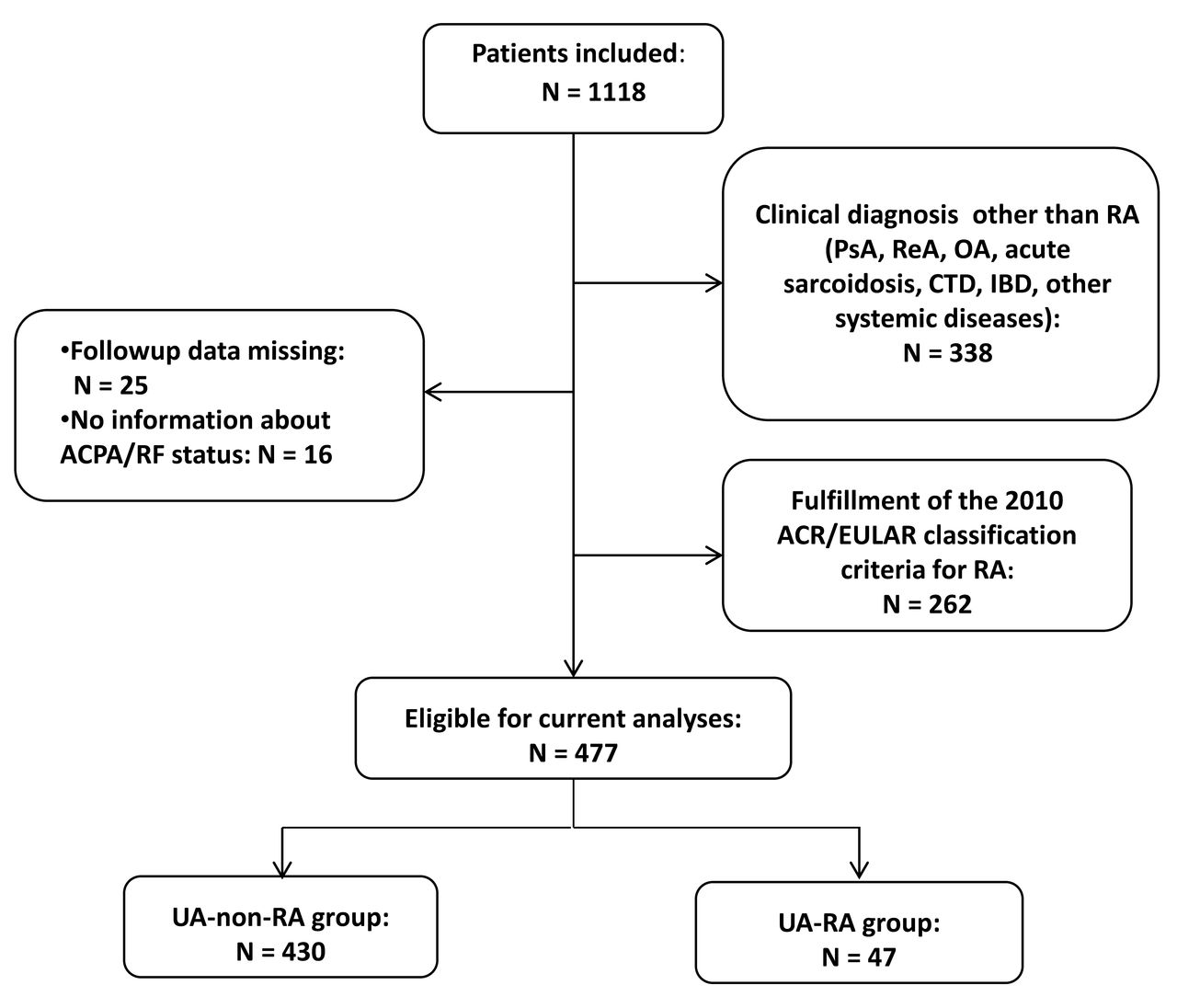
A flowchart of the selection of patients for the current study is shown in Figure 1. Excluded from the current analyses were patients with a baseline clinical diagnosis of a rheumatic disease other than RA, those who fulfilled the 2010 RA criteria at baseline, and patients without followup data. Patients who did not attend the scheduled study visits received a telephone call from a study nurse. One of the main reasons for not returning for assessment was having no symptoms of arthritis, and these patients were defined as having absence of clinical synovitis at their last contact with the rheumatology department. Persistent arthritis was defined as having 1 or more swollen joints at last followup, using DMARD during followup, and/or a final clinical diagnosis of RA.

Flowchart of patients eligible for current analyses. PsA: psoriatic arthritis; RA: rheumatoid arthritis; ReA: reactive arthritis; OA: osteoarthritis; CTD: connective tissue disease; IBD: inflammatory bowel disease; UA: undifferentiated arthritis; UA-non-RA group: patients not fulfilling the 2010 ACR/EULAR RA classification criteria during followup; UA-RA group: patients fulfilling the 2010 ACR/EULAR RA classification criteria during followup; ACR: American College of Rheumatology; EULAR: European League Against Rheumatism; ACPA: anticitrullinated protein antibodies; RF: rheumatoid factor.
The 2010 RA criteria were retrospectively applied at baseline and at followup visits. According to the criteria, patients with a score < 6 points could have their status reassessed, and the criteria might be fulfilled (cumulatively) with time3. We added the condition of at least 1 swollen joint at a given study visit for the criteria to be applied. The rate of seroconversion for RF and ACPA in early inflammatory arthritis patients is low12. In a sub-sample of patients from the NOR-VEAC study, only 1.8% changed status from seronegative to seropositive during 2 years of followup13,14. Thus, only baseline levels of ACPA and RF (assessed by either IgA or IgM) were used for application of the criteria in the current study.
The main outcome of our study was fulfillment of the 2010 RA criteria during 2 years of followup. Based on this, we defined 2 separate groups: patients with UA who later fulfilled the criteria during followup (UA-RA group) and those who did not (UA–non-RA group). The secondary outcomes were use of DMARD during followup, resolution of clinical synovitis by the final followup visit without ever using DMARD, and the final clinical diagnosis made by the treating rheumatologist. Clinical diagnoses were based on the World Health Organization International Classification of Diseases, 10th revision.
Statistical analysis
For continuous measures, means with SD were calculated for variables that were normally distributed, and medians with 25 and 75 percentiles for variables that were not. Independent samples t test, Mann-Whitney U test, and chi-square test were used as appropriate to compare baseline characteristics between groups of patients. Logistic regression analysis was performed with the main outcome, i.e., fulfillment of the 2010 RA criteria during followup, as the dependent variable and baseline variables as covariates. Because of limited statistical power (few patients in the UA-RA group), a limited number of covariates were selected for multivariable modeling, based on results from univariable analysis and clinical reasoning (sex, age, smoking, swollen shoulder joint, seropositivity, and joint involvement). The predictive performance of the logistic regression analyses was assessed by determining the area under the receiver-operator characteristic curve (AUC). Statistical tests were 2-sided, and p values below 0.05 were considered statistically significant. IBM SPSS Statistics Version 21 was used for the statistical analyses.
RESULTS
Patient characteristics
In total, 477 patients who were denoted UA at baseline were included (Figure 1). Baseline characteristics are shown in Table 1. The median duration of joint swelling was only 29 days, and 25% of the patients had disease duration < 10 days. Two-year followup data were obtained for 67.1% of the patients. Forty-three patients (9.0%) had their last followup visit done by telephone call from a nurse. There were 157 patients lost to followup. Eighty of these patients (51.0%) dropped out of the study because they were “feeling healthy,” and they had shorter disease duration, were more often male, and presented as monoarthritis. The remaining 77 patients (71 in the UA–non-RA group vs 6 in the UA-RA group) had no 2-year data; however, all of these patients had 1 followup visit or more after baseline. The reasons for loss to followup were the patient’s decision (n = 10/n = 0), the center lost contact with the patient (n = 16/n = 2), the patient had logistical issues or died (n = 8/n = 1), or the patient got another diagnosis (n = 24/n = 3); for some, the reason remains unknown (n = 13/n = 0). There were no major differences between the UA patients with complete 2-year followup data (n = 320) and the overall group of patients with UA (n = 477). However, 41 of the 320 patients with 2-year data (12.8%) fulfilled the 2010 RA criteria during followup compared to 9.8% of all 477 patients (Supplementary Table 1, available with the online version of this article). The 2010 RA criteria were fulfilled by 47 of 477 patients (9.8%) during followup in the UA-RA group, whereas 430 patients did not fulfill the criteria in the UA–non-RA group. Seventy percent of the patients fulfilling the criteria did so within the first 6 months of the study, and 89.4% within the first year. The UA-RA patients were older, more often RF-positive and ACPA-positive, female, and ever smokers, and had a higher DAS28 at baseline (Table 1). Further, the UA-RA group more frequently presented with small joint involvement, swollen shoulder joint, and polyarthritis. Occurrence of joint swelling in the remaining joints was equally distributed between the 2 groups. Over half of the UA–non-RA patients presented with monoarthritis. Duration of joint swelling was longer in the UA-RA group. CRP levels were similar across groups, while median ESR tended to be higher among UA-RA patients (p = 0.06).
Comparisons of baseline characteristics between UA-non-RA and UA-RA patients.
Treatment with DMARD and systemic glucocorticoids
Overall, 81 of 477 patients with UA (17.0%) received DMARD treatment during followup. Methotrexate (MTX) monotherapy was prescribed in 50 patients, sulfasalazine (SSZ) in 14, leflunomide and hydroxychloroquine in 1 patient each, and combinations of conventional synthetic DMARD in 11. Six patients received biologic DMARD, given in combination with either MTX or SSZ (3 patients in the UA-RA group and 3 patients in the UA–non-RA group). The 3 patients in the UA–non-RA group were ACPA- and RF-negative, had the final clinical diagnoses ankylosing spondylitis, seronegative RA, or UA, and were treated with etanercept. During followup, 162 patients (34.0%) were treated with systemic glucocorticoids (oral or intramuscular). There was a statistically significant difference in both DMARD and systemic glucocorticoid use between the patients with UA-RA and the UA–non-RA patients, 53.2% versus 13.0% (p < 0.001) and 59.6% versus 31.2% (p < 0.001), respectively.
Absence of clinical synovitis
In total, 338 patients (70.9%) achieved absence of clinical synovitis at their final followup visit without ever using DMARD, including 12 patients (25.5%) in the UA-RA group and 326 patients (75.8%) in the UA–non-RA group (p < 0.001). The remaining 139 patients were defined as having persistent arthritis, either because of the presence of 1 or more swollen joints at last followup (n = 55), use of DMARD during followup (n = 81), and/or a final clinical diagnosis of RA (n = 3).
Final clinical diagnosis
UA was the most frequent final clinical diagnosis made by the treating rheumatologist, occurring in 291 of 477 patients (61.0%). Thirty-eight patients (8.0%) were diagnosed with RA, of whom 24 were RF-negative and ACPA-negative. Reactive arthritis was the second most frequent final clinical diagnosis, made in 9.0% of the patients. The distribution of final clinical diagnoses is shown in Figure 2.

Distribution of final clinical diagnosis in 477 patients presenting with undifferentiated arthritis (UA) at baseline. RA: rheumatoid arthritis; ReA: reactive arthritis; PsA: psoriatic arthritis; OA: osteoarthritis; Other: acute sarcoidosis, IBD, CTD, crystal arthritis, SpA arthropathy, orthopedic diseases, and other systemic diseases; UA-non-RA: UA patients not fulfilling the 2010 ACR/EULAR RA classification criteria during followup; UA-RA: UA patients fulfilling the 2010 ACR/EULAR RA classification criteria during followup; CTD: connective tissue disease; IBD: inflammatory bowel disease; SpA: spondyloarthritis; ACR: American College of Rheumatology; EULAR: European League Against Rheumatism.
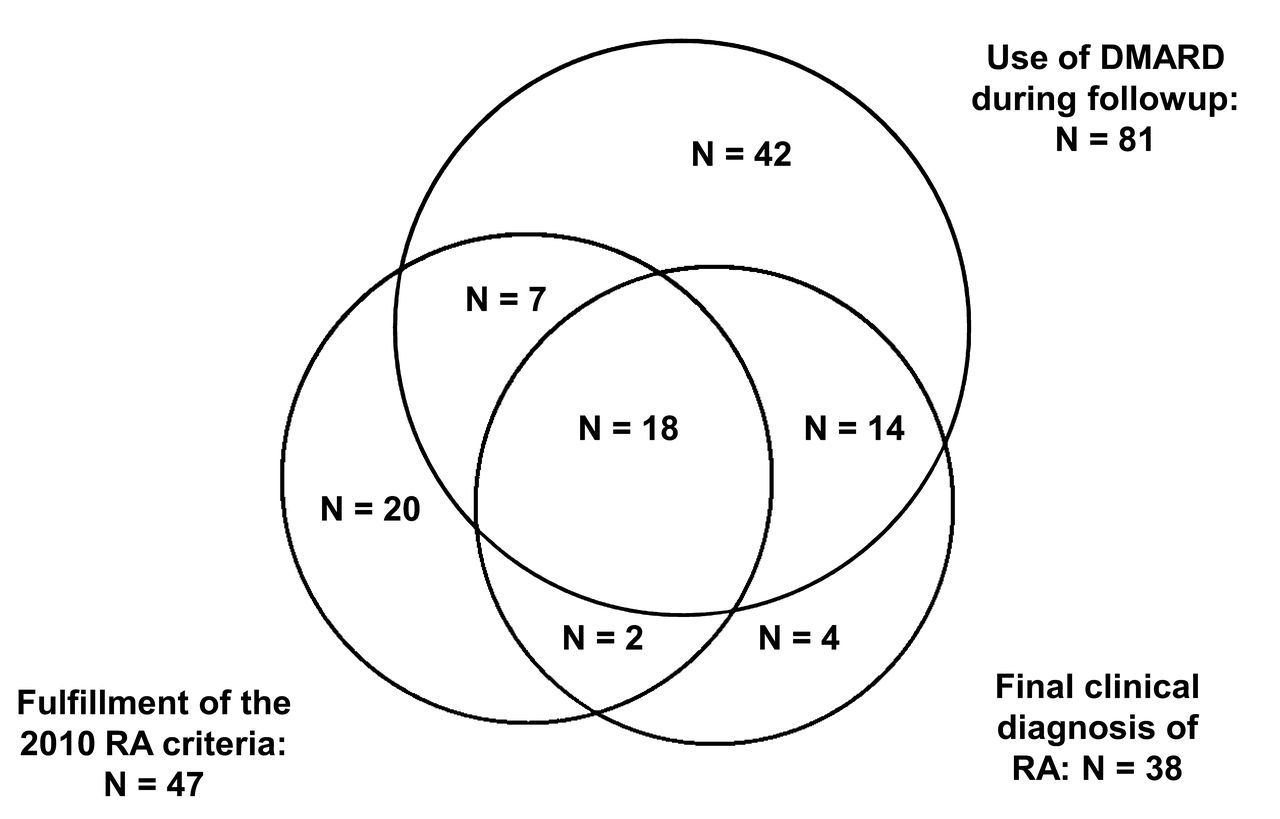
Eighteen of the 38 patients (47.4%) with final clinical diagnosis of RA did not fulfill the 2010 RA criteria during followup, and all these patients were ACPA-negative and RF-negative. Hence, none of these 18 patients got the highest possible joint score (5 points) according to the criteria set. Figure 3 shows the relationship between fulfillment of the 2010 ACR/EULAR classification criteria for RA, the use of DMARD during followup, and a final clinical diagnosis of RA.

The relationship between the main outcomes in 477 patients with undifferentiated arthritis at baseline. DMARD: disease-modifying antirheumatic drug; RA: rheumatoid arthritis.
Logistic regression analyses
We tested 2 multivariable logistic regression models with fulfillment of the 2010 RA criteria during followup as the dependent variable: one including age, sex, small joint involvement, RF/ACPA status, and swollen shoulder as covariates, and the other including age, sex, RF/ACPA status, and joint involvement pattern at baseline (mono-, oligo-, or polyarticular). The results are shown in Table 2. The 95% CI were generally wide because of limited statistical power. All variables included in the multivariable logistic regression models were independent predictors of fulfillment of the 2010 RA criteria during followup. Both models discriminated well between UA-RA and UA–non-RA patients with AUC above 0.8 (Table 2). We also performed logistic regression analyses with final clinical diagnosis of RA as the dependent variable (Supplementary Table 2, available with the online version of this article). Most of the variables that predicted fulfillment of the 2010 RA criteria were also predictive for the outcome of clinical RA, except for age and sex.
Uni- and multivariable logistic analyses with fulfillment of the 2010 RA criteria as the outcome.
DISCUSSION
The major novelty of our study is the focus on a large number of patients with very early arthritis, i.e., duration ≤ 16 weeks after onset of joint swelling. Only 9.8% of all the patients who presented with UA of ≤ 16 weeks fulfilled the 2010 ACR/EULAR classification criteria for RA during 2 years of followup. This observation differs from previous studies, which have found that, depending on the inclusion criteria, 17%–32% of patients with UA progress to RA2,15,16. Possible reasons for the discrepancy between our results and these numbers include the admittance of patients with monoarthritis in the current study, and also that most of the previous studies used the 1987 criteria to define RA17. Further, our study focused on arthritis of ≤ 16 weeks’ duration, which is shorter than most other early arthritis cohorts from the period before the implementation of the 2010 RA criteria and the new treatment recommendations for RA. Therefore, the median duration of joint swelling differed from other early arthritis cohorts18,19. The difference in duration was not statistically significantly different between the UA-RA and UA–non-RA groups, but numerically longer in the former group. If our inclusion criteria had allowed for longer duration of joint swelling, the proportion being defined as UA-RA might have been higher, because RA often has an insidious onset20. Over two-thirds of patients in the UA-RA group were classified as RA during the first 6 months, and nearly 90% within the first year, similar to what has been previously reported by others2.
In line with earlier studies18, the patients with UA-RA were older, more often female, ever smokers, presented with small joint involvement and polyarthritis, and had a higher DAS28 at baseline. Three previous studies of patients with UA not identified by the 2010 RA criteria at baseline showed that neither ACPA nor the Leiden prediction rule could accurately predict fulfillment of the 1987 RA criteria during followup9. The explanation was that ACPA and the majority of variables composing the prediction rule are also included in the 2010 RA criteria. However, in our study, in which fulfillment of the 2010 RA criteria was the main outcome, patients with UA-RA were also more frequently ACPA-and/or RF-positive at baseline.
Interestingly, having a swollen shoulder joint was associated with fulfilling the 2010 RA criteria and final clinical diagnosis of RA both in univariable and multivariable analyses. This finding is surprising and needs to be confirmed. Determining a swollen shoulder joint can be difficult for clinicians, and this should be taken into consideration when interpreting this result. Some authors have reported an association between involvement of large joints and a destructive course in patients with early RA21,22.
Because many studies have proven that early treatment of RA improves longterm outcomes, the question has arisen of whether treatment in the stage of UA may be even more beneficial23,24. Because only 17% of the patients with UA were treated with DMARD, it is difficult to answer this question based on our study. As expected, there was a significant difference between the patients with UA-RA and the UA–non-RA patients regarding DMARD use and treatment with systemic glucocorticoids during followup. Wevers-de Boer, et al performed a systematic literature review to investigate whether early initiation of DMARD was beneficial for patients with UA2. They found several observational studies indicating that disease outcomes improve if treatment is started within 6 months after symptom onset25,26,27, and that some trials suggest that a biological agent may slow progression to RA in patients with UA. However, few randomized placebo-controlled trials have been done to answer the question of whether early treatment in patients with UA is beneficial and which is the best treatment. More than two-thirds of all our patients with UA achieved absence of clinical synovitis at final followup visit without ever using DMARD. This proportion is somewhat higher than in previous Early Arthritis Cohort studies, which have found rates of self-limiting disease between 20% and 60%1,18. We assume that rheumatologists at the participating hospitals in our study were treating patients with early arthritis according to the recommendations at that time, and the low percentage of patients treated with DMARD is again heavily influenced by the inclusion criteria.
The current study is based on data collected before the 2010 RA criteria were implemented in clinical practice. This may explain why > 50% of the patients who fulfilled the criteria did not receive a final clinical diagnosis of RA from the treating rheumatologist. Presently, there is no gold standard for a clinical diagnosis of RA3. Even though classification criteria are intended to create well-defined and homogeneous cohorts of patients for research, the 1987 ACR criteria for RA have become an accepted reference standard for the diagnosis of RA. It is likely that the diagnostic process was influenced by the 1987 ACR criteria, which have been criticized for lack of sensitivity in early RA28. This may have led to more patients receiving the final clinical diagnosis of UA or reactive arthritis than RA. More patients with RA were identified by the 2010 ACR/EULAR classification criteria than by clinical diagnosis, demonstrating the ability of the new criteria to identify patients with RA at an earlier stage of the disease, which was the main objective of the ACR/EULAR task force when developing the new criteria3.
On the other hand, nearly half of the patients with the final clinical diagnosis of RA did not fulfill the criteria during followup, and all of these patients were ACPA- and RF-negative. One explanation could be that being ACPA-and/or RF-positive yields 2 or 3 criteria points (depending on the levels), while patients who are seronegative are required to have > 10 involved joints, and either positive CRP/ESR or duration ≥ 6 weeks to fulfill the criteria3. Even though the development of the new classification criteria results in an increased prevalence of classifiable RA in the early arthritis clinics29, it may be difficult for patients with negative ACPA and RF status to fulfill the new criteria, especially in the early stages of the disease30,31.
Our study has some limitations, one of them being patients not attending followup assessments. The most common reason for this was that patients felt healthy and had no joint symptoms. Another limitation is the small sample size in the UA-RA group, reducing the strength of statistical comparisons with the UA–non-RA group. In addition, we cannot be sure that all patients with synovitis due to OA were excluded from the study, as it may be difficult in some cases to distinguish OA from inflammatory arthritis.
Clinicians should have a broad focus on various arthritic diseases when seeing patients with recent-onset joint swelling and be aware that the majority of patients with recent-onset UA do not develop RA. These observations are also important to avoid overtreatment of patients who are likely to have a self-limiting arthritic disease.
Few patients with UA fulfilled the 2010 ACR/EULAR classification criteria for RA during followup in our study. This confirms the ability of the new criteria to identify patients with RA at an earlier stage of the disease. In addition to established predictors such as female sex, seropositivity, and small joint involvement, presentation with swollen shoulder joint was associated with later fulfillment of the criteria. This study also showed that it may be difficult for patients with negative ACPA and RF status to fulfill the criteria in the early stages of the disease, and that < 1 in 6 patients with UA needed DMARD for their arthritis to resolve over 2 years.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors thank the patients for participating in the study, the doctors and nurses at each center for data collection, and the laboratory at the Department of Immunology and Transfusion Medicine, Ullevål University Hospital, for performing the analyses of IgM RF, IgA RF, and anti-CCP2.
Footnotes
Supported by a grant from the South-Eastern Norway Regional Health Authority and the Department of Research and Innovation, Østfold Hospital. The Norwegian Very Early Arthritis Clinic study was funded by the Norwegian Foundation for Health and Rehabilitation and the South-Eastern Norway Regional Health Authority.
- Accepted for publication October 27, 2016.








{kind=link}
{kind=link}
{kind=link}