

There have been a few reports that describe IgG4-related disease that manifests as myocardial ischemia because of pseudotumor around the coronary artery1. Coronary computed tomography angiography (CCTA) is reported to be a better modality than coronary angiography for pericoronary artery lesion2.
A 54-year-old man with a history of paroxysmal atrial fibrillation and dyslipidemia presented with several months’ history of exercise-induced anterior chest pain. Although physical examination, electrocardiogram, and routine blood tests were unremarkable, angina pectoris was suspected based on his medical history and symptoms. CCTA was done for a detailed evaluation of the coronary artery, which revealed extensive soft tissue mass encasing the left anterior descending artery of the heart (Figure 1A). Whole trunk computed tomography (CT) scan also disclosed soft tissue mass around the right renal pelvis and focal enlargement of pancreas head (Figure 2A and Figure 2C). Magnetic resonance cholangiopancreatography confirmed diffuse irregular narrowing of the pancreatic duct, which suggests type 2 autoimmune pancreatitis. Laboratory test showed normal C-reactive protein and elevated serum IgG4 level of 183 mg/dl (reference range < 105 mg/dl). Based on elevated serum IgG4, retroperitoneal mass, and autoimmune pancreatitis, IgG4-related pericoronary arteritis was suspected2. The patient was treated with high-dose corticosteroid, and the followup CT scan after 3 months of therapy showed marked shrinking of soft tissue mass around the coronary artery (Figure 1B) and other lesions (Figure 2B and Figure 2D). Serum IgG4 level came down to 66.9 mg/dl 4 months after starting treatment.

A. Coronary computed tomography angiography reveals soft tissue mass surrounding anterior descending coronary artery (arrow). B. Followup scan after 3 months of steroid therapy shows improvement of pericoronary lesion.
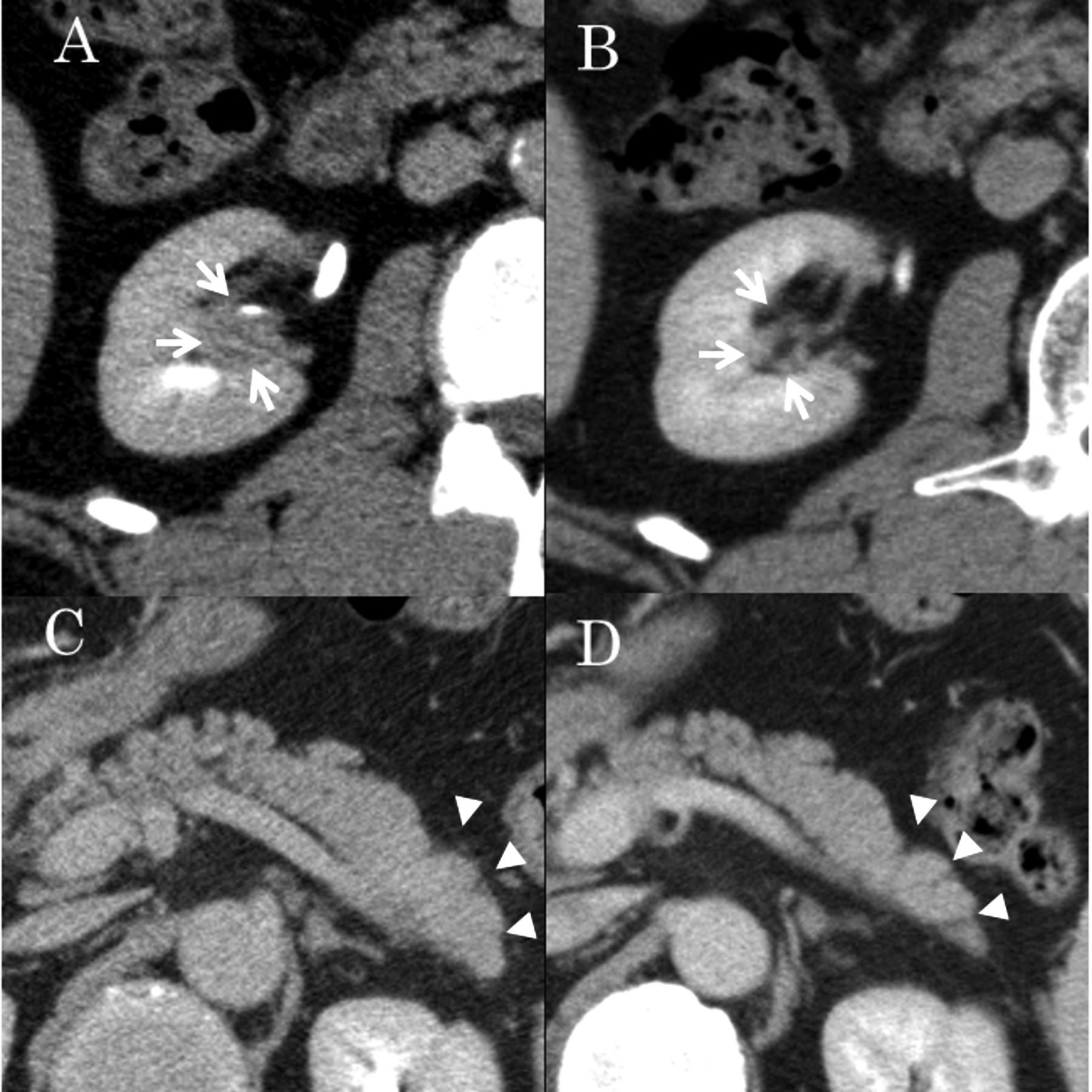
Computed tomography scan of abdomen. Soft tissue mass around right renal pelvis (A: arrow) and focal enlargement of pancreatic head (C: arrowhead) have nearly disappeared after 3 months of steroid therapy (B and D, respectively).
Appropriate imaging tests should be considered in patients with suspected IgG4-related coronary disease.
Footnotes
Ethical approval for this type of study is not required in accordance with the policy of the authors' institution.








{kind=link}
{kind=link}