

Abstract
Objective. Capillaroscopic abnormalities are predictive of future digital ulcers (DU). Our aim was to investigate whether functional digital vascular disease (thermographically assessed) is also associated with future DU.
Methods. A retrospective case note review of patients with systemic sclerosis (SSc) undergoing thermography and who were followed for up to about 3 years.
Results. There were 138 patients (equal mixture of normal/abnormal thermography). Patients with abnormal thermography were more likely to develop DU (clinician-observed and/or patient-reported, OR 2.84, p = 0.021), including multiple episodes, and more likely to die (OR 5.42, p = 0.050).
Conclusion. Abnormal thermography is associated with DU and disease severity in patients with SSc.
Digital ulcers (DU) are a serious manifestation of the underlying vascular disease in patients with systemic sclerosis (SSc)1. Around half of patients with SSc report previous DU, often occurring early in the course of the disease2,3. DU can be exquisitely painful and can reduce hand and global function (including occupation)4.
Thermographic abnormalities have been reported to enable the distinction between patients with primary (idiopathic) and secondary (e.g., SSc-related) Raynaud phenomenon (RP)5. Examples of normal and abnormal thermograms are depicted in Figure 1. Several authors have proposed that capillaroscopic change (assessing microvascular structure) is predictive of future DU6,7,8,9,10. Against this background, our aim was to investigate whether functional digital vascular disease (as assessed by thermography) is also associated with future DU.
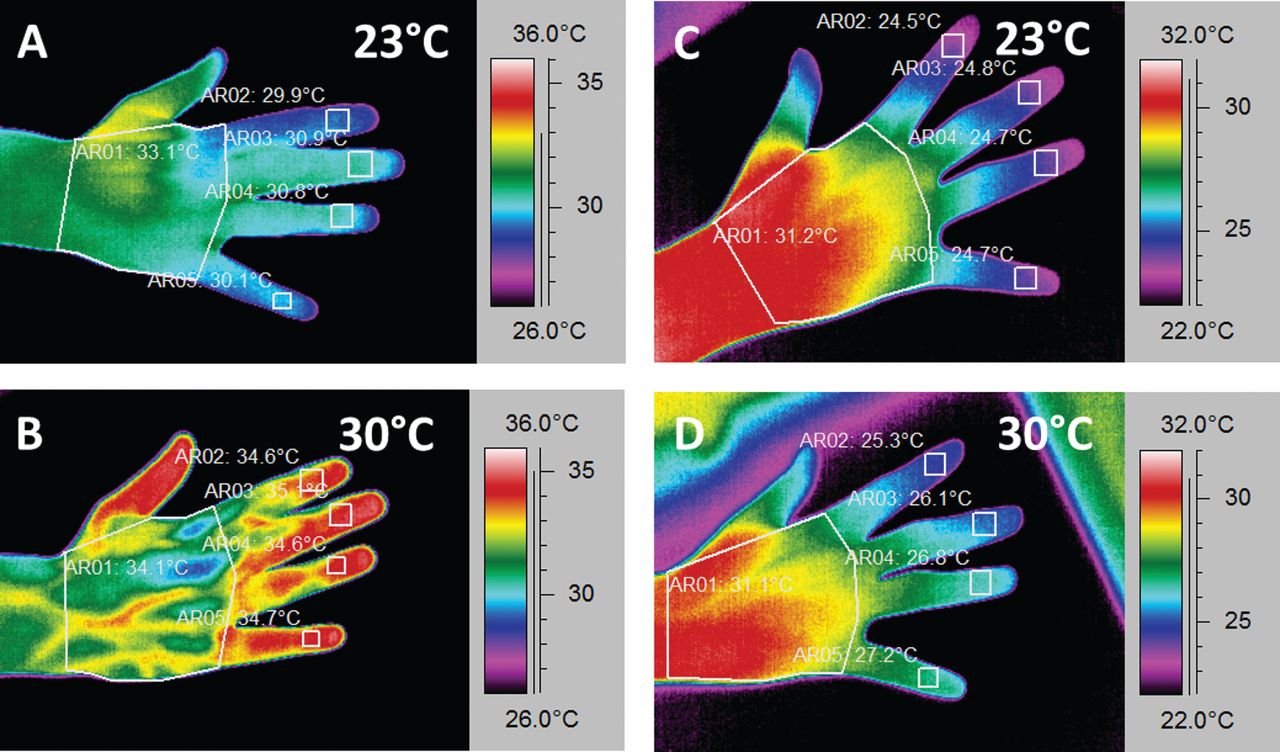
Normal (A, B) and abnormal (C, D) thermograms. For a thermogram to be defined as “abnormal,” at 30°C there is a persistent temperature (> 1°C) gradient (fingertip cooler than dorsum of the hand) along at least 1 of the fingers (D). The temperature of the dorsum of the hand in Panel D is 31.1°C.
MATERIALS AND METHODS
Data collection
Ours was a retrospective study based upon the case note review of all patients with SSc who underwent thermography at a tertiary referral center for SSc (with a particular interest in digital vascular disease) over a 5-year period between January 1, 2005, and December 31, 2009 (by an observer unaware of the thermography findings). Patients were categorized into limited (lcSSc) or diffuse cutaneous SSc (dcSSc) on the basis of the extent of skin involvement11. The study had National Health Service (NHS) research and development approval from Salford Royal NHS Foundation Trust. Written patient consent was not necessary because we used only previously collected, nonidentifiable information obtained during routine clinical practice within the confines of the direct healthcare team. The study was sponsored by the University of Manchester.
Thermography
At Salford Royal NHS Foundation Trust, thermography is part of the routine assessment at a patient’s first visit when a diagnosis of SSc is either made or suspected. Patients were requested not to smoke or to consume any caffeine-containing beverage for at least 4 h before attendance. After a period of initial acclimatization (at 23°C for 20 min) in a climate-controlled room, thermographic images (Agema 570 Elite, FLIR Systems Ltd.) were taken of the dorsal aspect of both hands. The hands were then immersed (wearing latex gloves) into water (15°C) for 1 min. Immediately after this (and with removal of the gloves), thermographic data of the dorsal aspect of the hands were obtained. If a temperature difference (of > 1°C) existed between 1 (or more) of the fingertips and dorsum of the hand, then the room temperature was elevated to 30°C for a further 20 min, with repeat imaging at the end of this period. Abnormal thermography was defined as a temperature gradient between 1 or more of the fingertips and the dorsum of the hand of > 1°C (fingers cooler than dorsum) at 30°C5. Baseline patient demographics and disease characteristics were documented.
DU documentation
DU episodes and indicators of severity were documented for up to 3 years post-thermography. DU “episodes” were either recorded as clinician-observed and/or patient-reported (the latter included DU which were present only in the interim between interaction with healthcare professionals — to have included only “clinician-observed” ulcers would have underestimated ulcer frequency by omitting these DU). Each DU “episode” (including the occurrence of multiple DU simultaneously) was considered temporally distinct from the next DU “episode” (i.e., clinician-observed or patient-reported healing between episodes). Indicators of DU severity: intravenous prostanoid therapy (given for DU disease only), surgical debridement, and digital amputation were also documented. Loss to followup and death were also recorded.
Statistical analysis
Logistic regression was performed with ulcer status (any ulceration on any finger in the followup period) as a binary outcome variable and this was performed with (1) any ulceration (clinician-observed and/or patient-reported) and (2) only clinician-observed ulceration as the outcome variable. Adjustment was made for prognostic variables: smoking status, disease subtype, autoantibody status (anticentromere and anti-Scl-70), age, and disease duration (as defined as time from the first non-RP manifestation). The number of ulceration episodes was included as the outcome in a Poisson regression model, which adjusted for differences in followup time. Because of the small number of DU complications, multivariable analysis was not possible. We present frequency data for these outcomes (including clinician-observed and/or patient-reported DU). All statistical analyses on the data were performed using STATA version 13.
RESULTS
Patient characteristics
There were 138 patients included in our analysis: 69 patients with normal and 69 with abnormal thermography (those with abnormal thermography were randomly selected from 90 patients during the time period using a computer-generated list). Patients’ baseline demographics and clinical characteristics are summarized in Table 1. All the included patients in our study had RP. Followup time in the normal and abnormal thermography groups were similar [mean (SD) 2.6 (0.9) and 2.8 (0.6) yrs, respectively; Table 1]. DU severity outcome was not available for 1 patient who developed DU in the normal thermography group.
Baseline patient demographics, DU occurrence and severity, and death or loss to followup post-thermography. Values are mean (SD) unless otherwise specified.
Occurrence of DU and number of episodes
Patients with abnormal compared with normal thermography were more likely to develop future DU (Table 1). For clinician-observed and/or patient-reported, the adjusted OR was 2.84 (95% CI 1.17–6.86, p = 0.021), whereas for clinician-observed alone, the OR was 1.79 (95% CI 0.70–4.55, p = 0.224). After adjusting for other variables and followup time using Poisson regression, the DU rate ratio (abnormal vs normal thermography) was 2.85 (95% CI 1.61–5.04, p < 0.001), denoting an estimated increase in the rate of observed or reported DU episodes of around 3 times for patients with abnormal thermography.
DU severity
Of those patients developing DU, patients with abnormal (compared with normal) thermography had a relatively higher frequency of surgical debridement, with similar intravenous prostanoid use, and with only 1 case of digital amputation in the normal thermography group (Table 1).
Loss to followup and death
Patients with abnormal (compared with normal thermography) were substantially more likely to die (OR 5.42, 95% CI 1.00–29.40, p = 0.050; Table 1). Patients with abnormal thermography were also more likely to be lost to followup (death or loss to followup, although this did not reach statistical significance; OR 2.32, 95% CI 0.84–6.40, p = 0.104; Table 1).
DISCUSSION
Patients with abnormal (compared with normal) thermography were significantly more likely to develop future DU, including multiple episodes, post-thermography. In addition, there is a suggestion that DU severity was greater in the abnormal thermography group, with a greater frequency of surgical debridements performed (although this should be interpreted with caution because there was only a small number of patients who required surgical intervention). Patients with abnormal thermography were more likely to be receiving treatment for RP at the time of thermography, which might suggest that they had more severe digital vascular disease, although this, too has to be interpreted in the context of a retrospective study.
Several authors have proposed different predictors of DU, including capillaroscopic abnormalities, in patients with SSc6,7,8,9,10. Smith, et al described a scoring system to predict DU within 6 months using 3 variables (number of capillaries in the middle finger of the dominant hand, DU count, and the presence or absence of critical digital ischemia) with positive and negative predictive values of 54.9% and 83.8%, respectively9. Future research is warranted to investigate the added prognostic benefit in predicting future DU from the addition of thermographic abnormalities. Relevant to this is Blaise, et al’s12 study suggesting that in patients with SSc, digital thermal hyperemia pattern (another index of vascular function) is predictive of DU.
An unexpected important finding of our study was that patients with abnormal thermography were significantly more likely to die within the followup period of up to 3 years. It was not the intention of our study to investigate the cause of death post-thermography and therefore these data were not available. It is increasingly recognized that DU are a biomarker of disease severity consisting of internal organ involvement in patients with SSc, including in early disease13,14. In addition, there have been recent reports that patients with RP (compared to without) have higher mortality15,16, particularly (at least in female patients) if the nailfold capillaries are abnormal16. Thermographic abnormalities should be further analyzed because these may represent a novel, noninvasive biomarker of disease severity, allowing the identification of patients with a particularly poor prognosis. We used the definition of abnormal thermography (“the dorsal distal difference”) as proposed by Clark, et al17; however, other thermographic definitions have been proposed in the assessment of RP and these should also be analyzed in future research.
Our study has a number of limitations, most of which are due to its retrospective design. To reduce any possible bias, the person collecting the data from review of patients’ medical records was unaware of the result of the thermography. We minimized the effect of differences between what rheumatologists and patients define as a DU by collecting both clinician-observed and patient-reported DU. If abnormal thermography is associated with more severe disease, then there is the possibility of a detection bias (i.e., patients with more severe disease are more likely to interact with healthcare professionals, increasing the likelihood of DU detection). In relation to patient-reported ulceration, patients with more severe disease may be more likely to report complications, resulting in recall bias. These factors may cause the relationship between abnormal thermography and ulceration to be overstated. Prospective studies should include a more robust scheme of DU measurement. Both loss to followup and death were greater in the abnormal thermography group; therefore, this may have resulted in the relative underestimation of DU in the abnormal thermography group. Future research is warranted to investigate the added benefit of thermography in addition to clinical features of severe digital vascular disease (e.g., history of DU), including in those patients with early disease who may already have thermographic abnormalities, but who because of their short disease duration are less likely to have developed ischemic complications. In addition, it is worth noting regarding the excess deaths observed (and therefore the possible underestimating of DU detection) that the proportion of patients with dcSSc (often associated with a more severe disease course and worse prognosis than lcSSc) was similar between the 2 groups.
Patients with abnormal thermography were significantly more likely to develop future DU (including multiple episodes) and abnormal thermography was associated with more severe digital vascular disease. In addition, patients with abnormal thermography were more likely to die. Future research including prospective studies is warranted to investigate thermography, a noninvasive imaging technique, as a prognostic marker of future DU and as a biomarker of digital vascular disease activity and/or severity in patients with SSc.
- Accepted for publication April 20, 2016.








{kind=link}