

Abstract
Objective. To examine the clinical and ultrasonographic (US) outcomes of reducing methotrexate (MTX) dosage upon initiating adalimumab (ADA) in MTX-inadequate responders with moderately to severely active rheumatoid arthritis (RA).
Methods. MUSICA (NCT01185288) was a double-blind, randomized, parallel-arm study of 309 patients with RA receiving MTX ≥ 15 mg/week for ≥ 12 weeks before screening. Patients were randomized to high dosage (20 mg/week) or low dosage (7.5 mg/week) MTX; all patients received 40 mg open-label ADA every other week for 24 weeks. The primary endpoint was Week 24 mean 28-joint Disease Activity Score based on C-reactive protein (DAS28-CRP) to test for noninferiority of low-dosage MTX using a 15% margin. US images were scored using a 10-joint semiquantitative system incorporating OMERACT definitions for pathology, assessing synovial hypertrophy, vascularity, and bony erosions.
Results. Rapid improvement in clinical indices was observed in both groups after addition of ADA. The difference in mean DAS28-CRP (0.37, 95% CI 0.07–0.66) comparing low-dosage (4.12, 95% CI 3.88–4.34) versus high-dosage MTX (3.75, 95% CI 3.52–3.97) was statistically significant and non-inferiority was not met. Statistically significant differences were not detected for most clinical, functional, and US outcomes. Pharmacokinetic and safety profiles were similar.
Conclusion. In MUSICA, Week 24 mean DAS28-CRP, the primary endpoint, did not meet non-inferiority for the low-dosage MTX group. Although the differences between the 2 MTX dosage groups were small, our study findings did not support routine MTX reduction in MTX inadequate responders initiating ADA.
It is recommended that patients with moderately or severely active rheumatoid arthritis (RA) initiate treatment with synthetic disease-modifying antirheumatic drugs (DMARD) to prevent disease progression and inflammatory destruction of joints1,2. Methotrexate (MTX) is the most commonly prescribed first-line DMARD with proven effectiveness and safety3,4; however, about two-thirds of patients may need more active therapy to achieve disease control5,6. Inadequate responders (IR) can enhance treatment response by adding a conventional synthetic DMARD or switching to combination treatment with a biologic, such as the anti-tumor necrosis factor (TNF) agent adalimumab (ADA)7,8.
While some patients achieve disease control when co-treated with ADA + MTX7,9,10, the required dosage of MTX is unclear. Whether MTX-IR patients initiating combination therapy with a TNF inhibitor require continued high-dosage MTX (≥ 15 mg/week) remains unaddressed.
Another aspect of patient care is the practicality of ultrasonography (US) in assessing disease activity. Radiographic evidence of joint disease may lag behind clinical disease11 and is not present in 70% of patients with RA at diagnosis12. US is more sensitive than conventional radiographs and clinical examinations at detecting joint changes13,14 and has detected active synovitis in patients in clinical remission or low disease activity (LDA)15,16. However, US remains a novel technique for many rheumatologists in North America. There is no international standard scoring system for quantifying or monitoring of RA disease activity by US, although validation is progressing11,17.
The purpose of the MUSICA trial was to examine the efficacy of high-dosage (20 mg/week) or low-dosage (7.5 mg/week) MTX in combination with ADA [40 mg every other week (eow)] in MTX-IR patients. MUSICA was the first large, randomized controlled trial to use US to assess joint disease in patients with RA over time, examining synovial hypertrophy, vascularity, and bony erosions.
MATERIALS AND METHODS
Patients
Adults ≥ 18 years of age diagnosed with RA per the 1987 revised American College of Rheumatology (ACR) classification criteria18 were included. Patients from 47 sites in the United States and Puerto Rico had to meet the inclusion criteria and none of the exclusion criteria at the screening and baseline visits, except the requirement for ≥ 5 tender joints out of 68, and ≥ 5 swollen joints out of 66, which could be met at either visit. Patients must have had 28-joint count Disease Activity Score (DAS28) based on C-reactive protein (CRP) ≥ 3.2 at baseline, been treated with MTX ≥ 15 mg/week (orally and/or injectable) for ≥ 12 weeks before screening, and discontinued all other DMARD ≥ 4 weeks before baseline; leflunomide must have been discontinued ≥ 24 weeks before baseline, or actively chelated with cholestyramine treatment before enrollment. Up to 10% of the patients could have used 1 prior biologic-DMARD, including abatacept, anakinra, certolizumab, etanercept (ETN), golimumab (GOL), infliximab (IFX), or tocilizumab (TCZ); otherwise, patients were biologic-naive. Patients exposed to ADA were excluded.
Study design
MUSICA (NCT01185288) was a 24-week, phase IV, multicenter, double-blind, randomized, parallel-arm study assessing the efficacy (noninferiority) of low-dosage MTX compared to maintaining high-dosage MTX treatment upon addition of ADA. The study included 2 treatment groups: 20 mg/week oral MTX (high-dosage MTX), or 7.5 mg/week oral MTX (low-dosage MTX). All patients received open-label (40 mg eow) subcutaneous ADA. At baseline, patients were centrally randomized 1:1 to the treatment groups and stratified by prior MTX dosage (15, 17.5, or ≥ 20 mg/week); all consented to participate in optional pharmacogenetic analysis. Only stratification of prior MTX dosage was included in the final analysis for all efficacy endpoints. Patients provided informed consent and the study was conducted in accordance with the protocol, International Conference on Harmonization, and ethical principles from the Declaration of Helsinki.
Sample size
Per historical clinical trial data with combination ADA + MTX treatment, the mean DAS28-CRP is 3.6 with SD of 1.1, and the mean change from baseline in DAS28-CRP is −2.15 with SD of 1.1 at Week 24. It was assumed that high-dosage and low-dosage MTX groups have mean DAS28-CRP of 3.6 and 3.75 at Week 24, respectively, in MUSICA. The rationale for choosing 15% as the noninferiority margin was to associate 15% of high-dosage MTX Week 24 DAS28-CRP value of 3.6 (i.e., 0.15 × 3.6 = 0.54) with a clinically acceptable diminished treatment effect of 25% of the change from the baseline (i.e., 0.25 × 2.15 = 0.54). With an additional assumption of SD of 1.2 for both groups, a total of 300 patients would be required to establish noninferiority with 80% power and a 2-sided level of significance of 0.05.
US imaging
US imaging by sponsor-trained sonographers was performed at baseline and weeks 4, 8, 12, 16, 20, and 24 to assess inflammation at the wrist, metacarpophalangeal (MCP) joints 2, 3, 5, and metatarsophalangeal (MTP) joint 5. Images from baseline and Week 24 (or discontinued patient’s last visit) were scored by 2 of 4 independent, US-experienced rheumatologists blinded to image order and treatment group; images at intervening visits were scored by 1 of 4 rheumatologists. Bilateral images based on dorsal midline imaging of the wrist, dorsal and volar imaging of MCP joints, and dorsal imaging of MTP5 were scored using a 4-grade semiquantitative scale19,20 for synovial hypertrophy and vascularity. Presence of bony erosions was assessed dichotomously using previously mentioned images in addition to lateral imaging of MCP2, medial imaging of MCP5, and plantar and lateral images of MTP5; wrists were not scored for bony erosion.
Efficacy and safety variables
Efficacy and safety outcomes were assessed, and blood samples for studies of ADA pharmacokinetics were collected before drug dosing at baseline and weeks 4, 8, 12, 16, 20, and 24. The primary endpoint was Week 24 mean DAS28-CRP. Secondary endpoints with a noninferiority margin of 15% included Week 24 proportion of patients achieving synovial vascularity improvement ≥ 30% measured by Power Doppler, ACR50, ACR70, and clinically meaningful improvement in physical function [change from baseline ≤ −0.22 in the Health Assessment Questionnaire Disability Index (HAQ-DI)]. Exploratory analyses assessed the proportion of patients achieving clinical LDA and remission by DAS28-CRP (< 3.2 and < 2.6, respectively), Simplified Disease Activity Index (SDAI; ≤ 11 and ≤ 3.3, respectively), and Clinical Disease Activity Index (CDAI; ≤ 10 and ≤ 2.8, respectively). The proportion of patients achieving ACR20/50/70 response, ΔHAQ-DI ≤ −0.22, and HAQ-DI < 0.5 were compared between treatment groups. Synovial hypertrophy, synovial vascularity, bony erosions, tender joint count (TJC), swollen joint count (SJC), physician’s global assessment (PGA), and patient’s global assessment (PtGA) of disease activity and pain were measured.
Adverse events (AE) were reported by system organ class and Medical Dictionary for Drug Regulatory Activities (MedDRA v15.1) preferred terms, including 18 prespecified AE attributed to MTX toxicity (described in the MTX label), assessed at each study visit.
Statistical analyses
Noninferiority was assessed using the 2-sided 95% CI of the difference between the low-dosage and high-dosage MTX groups, based on the least squared means from the ANCOVA with baseline value, treatment group, and prior MTX dosage included in the model for continuous endpoints, and the Cochran-Haenszel-Mantel test after adjusting for prior MTX dosage for categorical endpoints. For the primary efficacy endpoint, noninferiority of low-dosage MTX could be claimed if the upper limit of the CI (for the difference in Week 24 mean DAS28-CRP) was less than the non-inferiority margin (15%) of the Week 24 high-dosage mean score. Last observation carried forward (LOCF) was used to account for missing data. The primary endpoint was also examined using observed data and multiple imputation for sensitivity analyses. Secondary endpoints were also examined using observed data and nonresponder imputation (NRI) for sensitivity analyses. There was no multiplicity adjustment for testing the noninferiority of the secondary endpoints. The averaged value from 2 independent, blinded readers was used to score synovial hypertrophy, synovial vascularity, and bony erosion at baseline and Week 24, or early termination visit. The value from a single reader was used for visits at weeks 4 to 20 (data not shown).
For additional exploratory analyses, the low-dosage MTX group was assessed to determine whether it was inferior to the high-dosage MTX group in some efficacy endpoints. Safety analyses included data from all patients who received ≥ 1 dose of the study drug. Fisher’s exact test was performed for proportions of patients with AE; Poisson regression with offset of patient years (PY) was performed for number of AE per 100 PY.
RESULTS
Patient disposition
Patients with moderately to severely active RA were enrolled and randomized into 2 treatment groups: low-dosage (7.5 mg/week, n = 154) or high-dosage (20 mg/week, n = 155) MTX plus open-label ADA. Out of 393 screened subjects, 84 did not fulfill inclusion and/or met exclusion criteria. The eligible 309 patients were randomized at 1 of 47 sites (median of 6 patients per site, 1–18 patients per site). Similar numbers of patients within each treatment group completed the study, with 274/309 patients (88.7%) overall completing 24 weeks of treatment (Figure 1). AE, withdrawn consent, and loss to followup accounted for the majority of discontinuations, and were similar in number between groups. The first patient’s first visit occurred on September 13, 2010, and the last patient’s last visit occurred on January 31, 2013. Mean drug compliance was 96.9% and 98.4% for MTX and ADA, respectively.

Patient flow. Primary reasons for discontinuation are listed. aOne patient each with noncompliance with medications and study visits, per investigator discretion, failed inclusion criteria, and 2 patients with lack of efficacy. bOne patient delayed first dose of study drug for 2 weeks and completed the Week 24 efficacy assessment at Week 22 after first study drug dose, therefore, categorized as a Week 20 completer. ADA: adalimumab; MTX: methotrexate; AE: adverse events.
Baseline demographics and disease characteristics
The average age of patients was 54.8 years, with mean baseline disease duration of 5.3 years and a mean duration of MTX treatment prior to the study of 1.5 years. Disease activity was high at baseline with a mean DAS28-CRP of 5.8, SDAI 42.4, and CDAI 40.9, and substantial evidence of joint disease (i.e., elevated TJC, SJC, and synovial hypertrophy scores; Table 1). Overall, the 2 treatment groups were evenly matched, with no statistically significant differences in patient demographics or disease characteristics.
Patient demographics and baseline disease characteristics. Data are mean ± SD unless indicated otherwise.
Patients were MTX-IR with different prior dosages of MTX; 151 patients (48.9%) were taking a prior stable MTX dosage of 15 mg/week, 40 patients (12.9%) were taking 17.5 mg/week, and 118 patients (38.2%) were taking ≥ 20 mg/week. Importantly, these patients were evenly randomized to the 2 treatment groups according to the stratification protocol. Prior biologic DMARD exposure was reported in 17 patients (5.5%; 7 ETN, 5 IFX, 3 GOL, 1 certolizumab, and 1 TCZ). Previous exposure to 1 synthetic DMARD other than MTX was reported in 25 patients (8.1%); 5 (1.6%) received 2 synthetic DMARD.
Noninferiority assessment
LOCF was used to impute for 57 of 309 patients who were missing DAS28-CRP at Week 24. After 24 weeks, the low-dosage MTX group’s mean DAS28-CRP (95% CI) was 4.12 (3.88–4.34), representing a change from baseline of −1.67 (−1.89 to −1.45). In comparison, the high-dosage MTX group’s mean DAS28-CRP (95% CI) of 3.75 (3.52–3.97) was statistically lower (p = 0.014) and the mean change from baseline was −2.06 (−2.28 to −1.84). Although the difference of 0.37 in Week 24 mean DAS28-CRP was within the 15% non-inferiority margin of 0.56 (15% of Week 24 high-dosage mean score 3.75), noninferiority of low-dosage MTX, the primary endpoint, could not be claimed because the upper limit of the 95% CI (0.07–0.66) was greater than the noninferiority margin of 0.56 (Figure 2). Additionally, the Week 24 95% CI of the difference excluded 0.
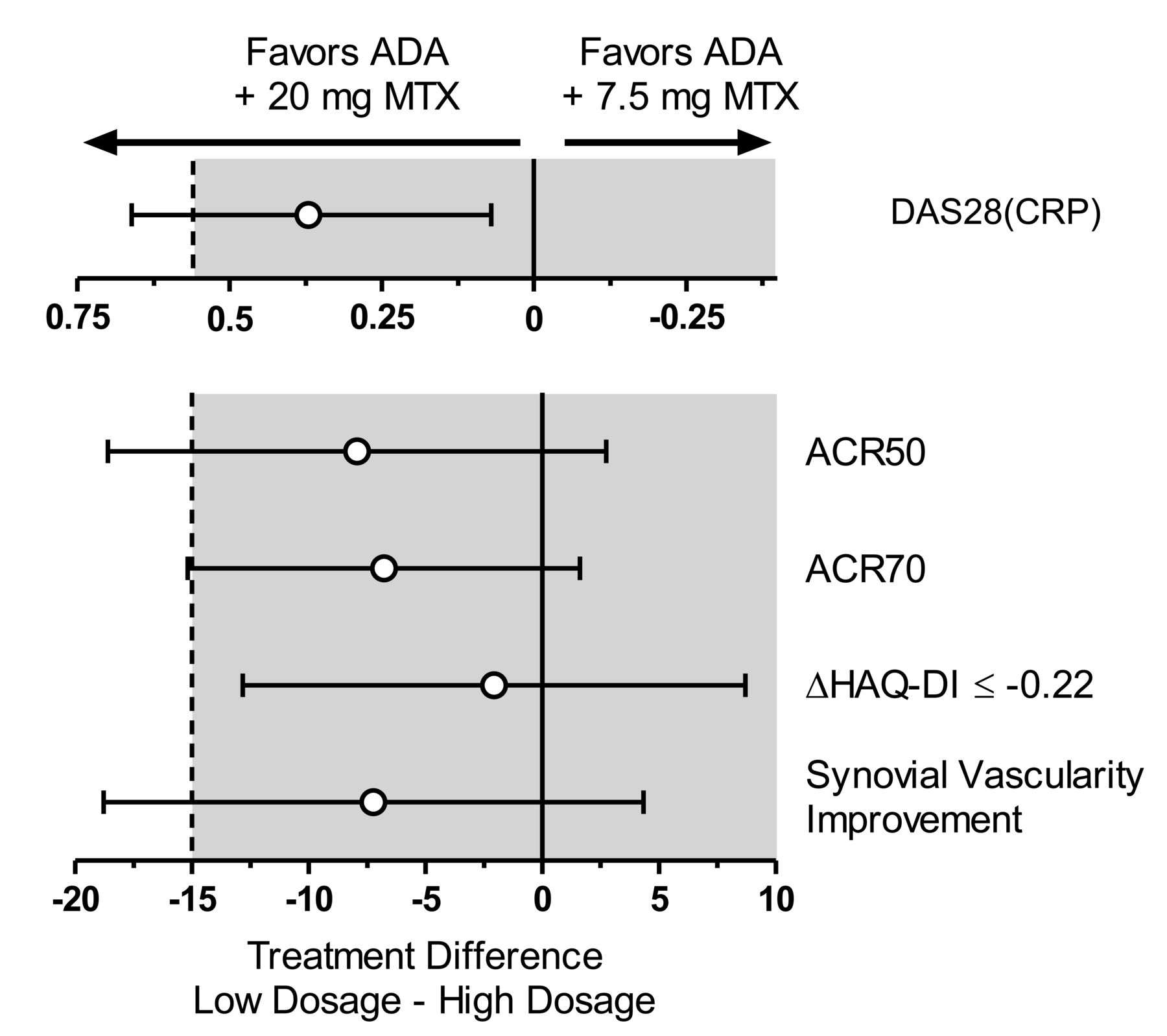
Assessment of low-dosage MTX + ADA noninferiority compared to high-dosage MTX + ADA after 24 weeks. The difference in mean DAS28-CRP between low- and high-dosage MTX groups, and differences in proportions of patients achieving ACR50, ACR70, clinically meaningful differences in physical function, and synovial vascularity improvement (> 30%) are plotted with the difference 95% CI. The dashed line represents the noninferiority margin. ADA: adalimumab; MTX: methotrexate; DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein; ACR: American College of Rheumatology; HAQ-DI: Health Assessment Questionnaire–Disability Index.
The low-dosage MTX group was noninferior to the high-dosage MTX group for the proportion of patients achieving clinically meaningful improvement in physical function, a secondary endpoint (Figure 2). The additional secondary endpoints, including the proportion of patients achieving ACR50, ACR70, and synovial vascularity improvement > 30%, did not meet noninferiority because the 95% CI of the differences crossed the noninferiority margin (Figure 2).
Additional exploratory efficacy assessments
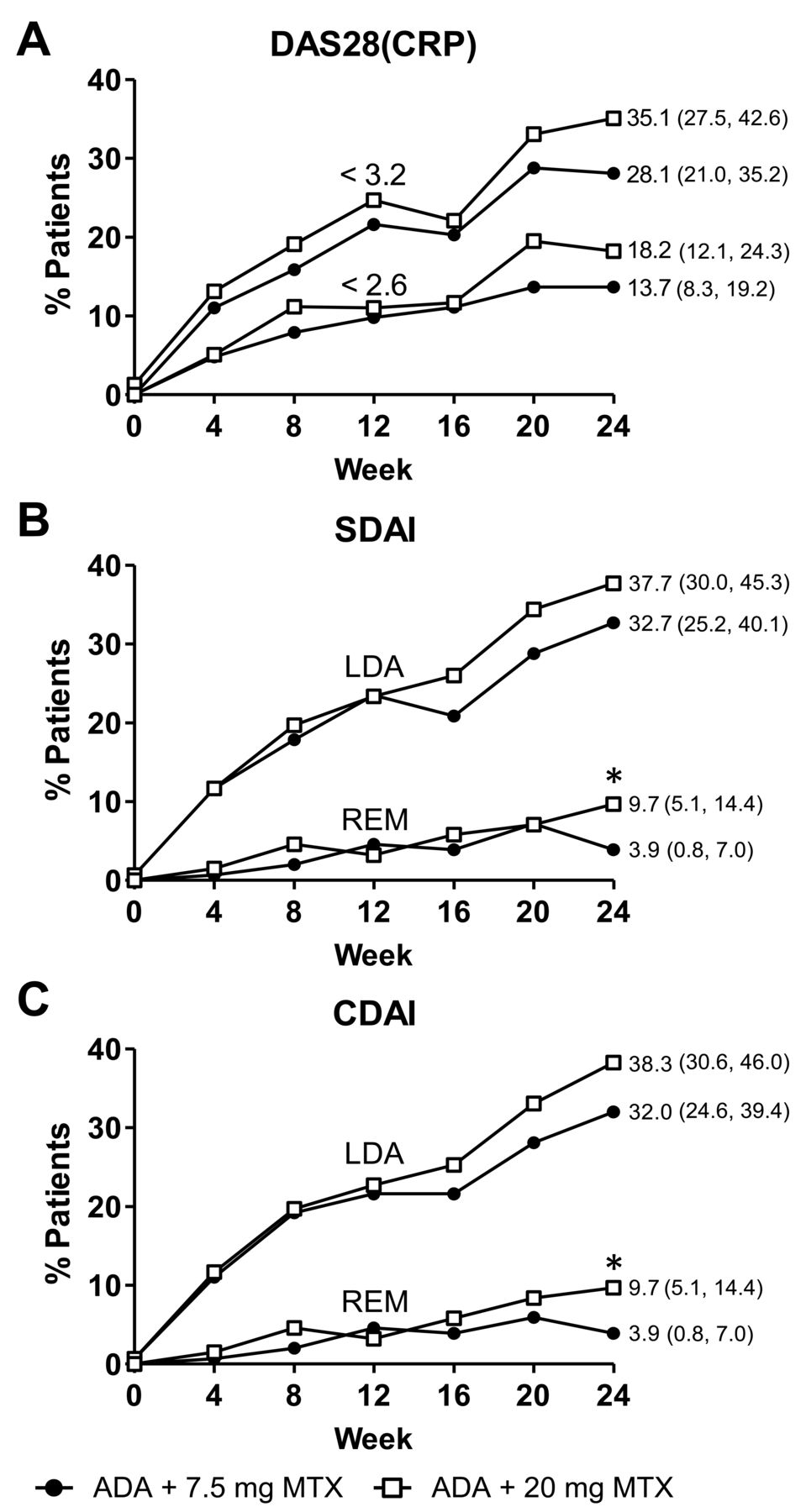
Generally, clinical disease activity measured by DAS28-CRP, SDAI, and CDAI trended together over time in the proportion of patients achieving LDA and remission based on LOCF (Figure 3). At Week 24, a numerically lower proportion of patients in the low-dosage MTX group compared to the high-dosage MTX group achieved LDA (LOCF, 28.1–32.7% vs 35.1–38.3%); the differences between the groups were not statistically significant at Week 24 by all 3 disease activity indices (secondary outcomes). Proportions were still increasing at Week 24. Sensitivity analyses (NRI) revealed small differences in the proportions of patients achieving LDA when comparing low-dosage (26.6–31.2%) versus high-dosage (31.0–33.5%) MTX groups. By LOCF, 21/153 (13.7%) and 28/154 (18.2%) of patients in the low-dosage and high-dosage MTX groups, respectively, achieved DAS28-CRP remission (p = 0.306); 6/153 (3.9%) and 15/154 (9.7%) achieved SDAI remission or CDAI remission (p = 0.049). Using sensitivity analyses (NRI) at Week 24, 21/154 (13.6%) and 24/155 (15.5%) in the low-dosage and high-dosage MTX groups, respectively, achieved DAS 28-CRP remission (p = 0.629); 6/154 (3.9%) and 13/155 (8.4%) achieved SDAI remission and CDAI remission (p = 0.100). Statistically significant differences in the proportion of patients remaining in high disease activity at Week 24 were observed, as measured by DAS28-CRP (26.1% vs 16.2%; p = 0.036), SDAI (31.4% vs 20.8%; p = 0.037), and CDAI (35.9% vs 24.0%; p = 0.025) comparing the low-dosage versus high-dosage MTX groups, respectively.

Clinical efficacy after 24 weeks of open-label ADA in combination with 7.5 or 20 mg/week MTX. A. Proportion of patients over time achieving DAS28-CRP < 3.2 and < 2.6. B. Proportion of patients over time achieving SDAI LDA and remission. C. Proportion of patients over time achieving CDAI LDA and remission. LOCF data are presented. * Denotes statistical significance at the 0.05 level. DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein; SDAI: Simplified Disease Activity Index; LDA: low disease activity; REM: remission; CDAI: Clinical Disease Activity Index; ADA: adalimumab; MTX: methotrexate; LOCF: last observation carried forward.
ACR responses at Week 24 numerically favored the high-dosage group. In the low-dosage and high-dosage MTX groups, respectively, 57% and 61.7% of patients achieved ACR20 (p = 0.395); 29.8% and 37.7% achieved ACR50 (p = 0.145); 13.2% and 20.1% achieved ACR70 (p = 0.114; Figure 4A). Nearly two-thirds of all patients had clinically meaningful improvement in physical function. A similar proportion of patients in the low-dosage versus high-dosage MTX group achieved ΔHAQ-DI ≤ −0.22 (63.6 vs 65.6%, p = 0.707) and HAQ-DI < 0.5 (31.4 vs 32.9%, p = 0.792; Figure 4B). Week 24 improvements in synovial vascularity, measured by either the proportion of patients with > 30% improvement (p = 0.221) or mean change from baseline in Power Doppler score (p = 0.779), were not statistically different between treatment groups (Figure 4C and Figure 4D). By Week 24, 45.5% and 52.4% of patients in the low-dosage and high-dosage MTX groups showed an improvement in synovial vascularity (Figure 4C). Synovial inflammation and presence of bony erosions showed comparable improvements regardless of MTX dosage (p > 0.05; Figure 4D).

Clinical, functional, and ultrasonographic efficacy, and ADA pharmacokinetics after 24 weeks of open-label ADA in combination with different doses of MTX. A. Proportion of patients achieving ACR20/50/70 response. B. Clinically meaningful change in physical function (ΔHAQ-DI ≤ −0.22) and normal function (HAQ-DI < 0.5). C. Synovial vascularity improvement > 30%. D. Mean changes from baseline in synovial hypertrophy, synovial vascularity, and bony erosions. E. ADA serum trough concentrations over time. Ultrasonographic scores for baseline and Week 24, or early termination visit, were the average of scores from 2 raters. ACR: American College of Rheumatology; HAQ-DI: Health Assessment Questionnaire–Disability Index; ADA: adalimumab; MTX: methotrexate.
Improvements in other secondary efficacy outcomes, including TJC, SJC, PGA, PtGA, pain, and CRP were comparable between treatment groups over time (Supplementary Figure 1, available online at jrheum.org); only differences in Week 24 mean SJC and PGA were statistically significant.
ADA pharmacokinetics
Pharmacokinetic analyses revealed slightly higher mean ADA concentrations in the high-dosage MTX group, with separation from the low-dosage MTX group beginning at about Week 8 and maintained throughout the study (Figure 4E). Week 24 ADA mean serum concentrations for patients in the high-dosage MTX group averaged 8.6 ± 5.2 µg/ml compared to 7.1 ± 6.2 µg/ml for patients in the low-dosage MTX group. ADA serum concentrations observed in the treatment groups were comparable or above those observed in patients naive to MTX treatment.
Safety assessments
AE were reported by 195/309 patients (63.1%), with similar numbers in both groups. Interestingly, more events per 100 PY were observed in the low-dosage MTX group for some AE (Table 2). Serious, severe, and infectious AE occurred in a slightly larger percentage of patients within the high-dosage MTX group; no serious infections occurred within the low-dosage MTX group. Five patients, all within the high-dosage MTX group, experienced 7 serious infections. One patient, receiving concomitant prednisone, reported 3 infections (soft tissue abscess, staphylococcal infection, and septic shock) all occurring on study Day 72; the patient remained in the study until completion. Two patients discontinued owing to serious infections: 1 experienced a moderate case of pneumonia (Day 36, persisting for 22 days); another receiving concomitant prednisone experienced an ophthalmic herpes zoster infection 7 days after last dosing of study drug (Day 142) that persisted for 11 days. One patient each experienced pneumonia Legionella (Day 24, receiving concomitant prednisone) and cellulitis (Day 14); both remained in the study. Two patients reported malignancy; 1 patient in the low-dosage MTX group reported a severe bile duct cancer and 1 patient in the high-dosage MTX group reported mild squamous cell carcinoma of the skin. No new safety signals pertaining to opportunistic infections, tuberculosis, or deaths were recorded in MUSICA.
Safety results following 24 weeks of treatment.
The most commonly reported AE were nausea, upper respiratory tract infection, urinary tract infection, dizziness, and headache. The only AE distinctly different between treatment groups was injection site reaction events/100 PY, which were more prevalent in the low-dosage MTX group (36.1 events/100 PY vs 4.3 events/100 PY), although all 25 events were recorded in only 6/154 low-dosage MTX patients.
Known MTX-related toxicity AE were assessed at each study visit (Table 2). Excessive fatigue and/or malaise and abnormal hair loss were interestingly more prevalent in the low-dosage MTX group (investigator-assessed). Both treatment groups had similar laboratory test and vital sign results. No new safety signals were observed.
DISCUSSION
MUSICA was the first study, to our knowledge, to investigate MTX-dosage reduction in MTX-IR patients with RA initiating biologic combination therapy, and the first randomized, blinded ADA study to assess rheumatoid-specific inflammation in patients by US. Although clinically significant improvements in disease activity were observed for both MTX dosage groups, noninferiority of low-dosage MTX + ADA was not statistically met for the primary endpoint, and a statistically significant difference of 0.37 (95% CI: 0.07–0.66) in mean Week 24 DAS28-CRP was observed for the low- vs high-dosage MTX group. Noninferiority of low dosage MTX + ADA was not met for 3/4 secondary endpoints. While many individual efficacy variables did not show statistically significant differences between treatment groups, they were not powered to detect differences.
Addition of ADA to MTX-IR resulted in increased ACR responses, and a marked improvement in physical function, after 24 weeks (mean ΔHAQ-DI = −0.5), similar to reports from previous ADA trials in patients with longstanding RA9,21. Sensitivity analyses using observed data and NRI confirmed that differences between treatment groups were small, and generally smaller than when analyzed by LOCF. By US, nearly half of all patients showed improved synovial inflammation at 24 weeks compared to baseline.
Minor differences in mean ADA serum concentrations between the 2 groups were observed as early as Week 8 and up to Week 24 (7.1 ± 6.2 and 8.6 ± 5.2 for the low-dosage and high-dosage MTX groups, respectively). These concentrations were consistent with the ability to achieve therapeutic response22,23, and in agreement with DAS28-CRP and ACR responses over time. MTX is known to reduce ADA clearance by 29% and 44% after single and multiple doses, respectively22,24. The small ADA concentration difference may be due to the stability of polyglutamated MTX25 from pretrial exposure. The effect of different doses of MTX on steady-state ADA pharmacokinetics, evaluated in a parallel study of treatment-naive patients, resulted in similar ADA concentrations when co-administered with 10 or 20 mg MTX and slightly lower concentrations when co-administered with 2.5 and 5 mg MTX23. The presence of anti-ADA antibodies (AAA) has been shown to affect ADA pharmacokinetics and efficacy26. Levels of AAA have been demonstrated to be lower in patients receiving higher concomitant MTX dose27. In MUSICA, the overall incidence of AAA was low28 and therefore unlikely to have had a meaningful effect on ADA pharmacokinetics/efficacy.
Serious, severe, and infectious AE were slightly more prevalent in the high-dosage group. Interestingly, more AE/100 PY were observed in the low-dosage group, possibly as a result of disease flaring after MTX reduction. More patients in this group reported arthritis and RA as an AE29,30. Among MTX toxicity-related AE, abnormal hair loss and excessive fatigue and/or malaise were more prevalent among the low-dosage group.
The MUSICA results suggest that lowering the dose of concomitant MTX to 7.5 mg/week from ≥ 15 mg/week upon initiating ADA may reduce the degree of clinical response when compared to steady or slightly increased MTX. Patients were receiving 15, 17.5, or ≥ 20 mg/week MTX prior to study entry. Patients taking prior 15 mg/week MTX (n = 151, 48.9%) who were randomized to the 7.5 mg/week arm had a dose reduction of 7.5 mg/week MTX. However, patients taking higher prior MTX doses (17.5 to ≥ 20 mg/week) who were randomized to the 7.5 mg/week arm experienced a larger MTX dose reduction (10–14.5 mg/week). Patients who had a smaller reduction in MTX had better clinical responses than those who experienced a larger reduction in MTX (Supplementary Figure 2, available online at jrheum.org). The study treatment duration may limit accurate interpretation because the proportions of patients achieving clinical LDA and remission measured by DAS28-CRP, SDAI, and CDAI were still increasing at Week 24, suggesting that longer treatment duration may have continued to reduce disease activity. One study design limitation was the relatively large noninferiority margin of 15% for ACR50 and ACR70, which showed proportions of responders < 40% at Week 24.
Other trials have investigated MTX dosage reduction after combination treatment or achievement of a target disease state31,32. In the CAMEO trial, ETN monotherapy was noninferior to ETN + MTX only for patients in LDA31. In an open-label extension trial33, clinical response was maintained upon an MTX dosage-reduction (mean 17.5 to 11 mg/week) or discontinuation, following 3 months of ETN + MTX. In MUSICA, the MTX dosage reductions upon ADA initiation were often larger, and patients had active RA. Noninferiority was not met for the mean DAS28-CRP for low- vs high-dosage MTX, and patients who decreased concomitant MTX had a slightly reduced degree of clinical response compared to those taking steady or slightly increased MTX. Overall, these data do not support MTX dosage reductions in patients initiating ADA. However, in a proportion of patients who may need to reduce MTX because of toxicity, much of the clinical efficacy of combination therapy may still be retained, especially if dosage reductions of MTX are modest.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
Medical writing support was provided by Douglas E. Dylla, PhD, and Naina Barretto, PhD, both full-time employees of AbbVie Inc.
Footnotes
AbbVie Inc. sponsored the study (NCT01185288), contributed to its design, participated in the collection, analysis, and interpretation of the data, and in the writing, reviewing, and approval of the final manuscript. GSK is a consultant for AbbVie Inc. AME has received research grants and served as a speaker for AbbVie Inc. SLG is an employee of AbbVie and owns stock. SL is a former employee of AbbVie and owns stock options. JK and HK are full-time employees of AbbVie and own stock or stock options.
Full Release Article. For details see Reprints/Permissions at jrheum.org
- Accepted for publication April 19, 2016.
Free online via JRheum Full Release option








{kind=link}
{kind=link}
{kind=link}
{kind=link}