

Giant cell arteritis (GCA) is the most common vasculitis in Western countries among individuals 50 years and older1. This medium and large-vessel granulomatous vasculitis typically affects the extracranial branches of the carotid artery1. Common features of the disease such as headache or jaw claudication are the result of vasculitic involvement of arteries derived from the external carotid artery. However, visual manifestations, including visual loss — the most feared complications of this vasculitis — are generally due to the arteritic damage affecting the ophthalmic branches of the internal carotid artery2.
The most common ophthalmic manifestation of GCA is anterior ischemic optic neuropathy, which is caused by interruption of blood flow in the posterior ciliary arteries to the optic nerve head. The clinical picture is described as sudden painless loss of vision3. Visual loss may present as a mist in all or part of the visual field and evolve within 24 to 48 hours to total blindness. Unilateral visual loss may be initially unnoticed by the patient until, by chance, the unaffected eye is covered. One eye is affected first, but involvement of the other eye in untreated patients may occur 1 to 10 days after the initial event4. In the acute phase of anterior ischemic optic neuropathy, the optic disc is pale and swollen, but the retina is almost normal. Afterward, optic nerve atrophy associated with optic disc cupping is observed. Less commonly, visual loss is caused by central retinal artery occlusion, ischemic retrobulbar neuropathy or occipital infarction in the context of a stroke involving the vertebrobasilar territory2. When the arteritic process involves the central retinal artery leading to retinal stroke, the retina is damaged primarily and it appears greyish and swollen, and a contrasting red zone can be observed in the macula, the so-called “cherry red spot.”
In this issue of The Journal, Saleh, et al report data on visual complications in biopsy-proven GCA patients from the area of Skåne, the southernmost administrative county of Sweden5.
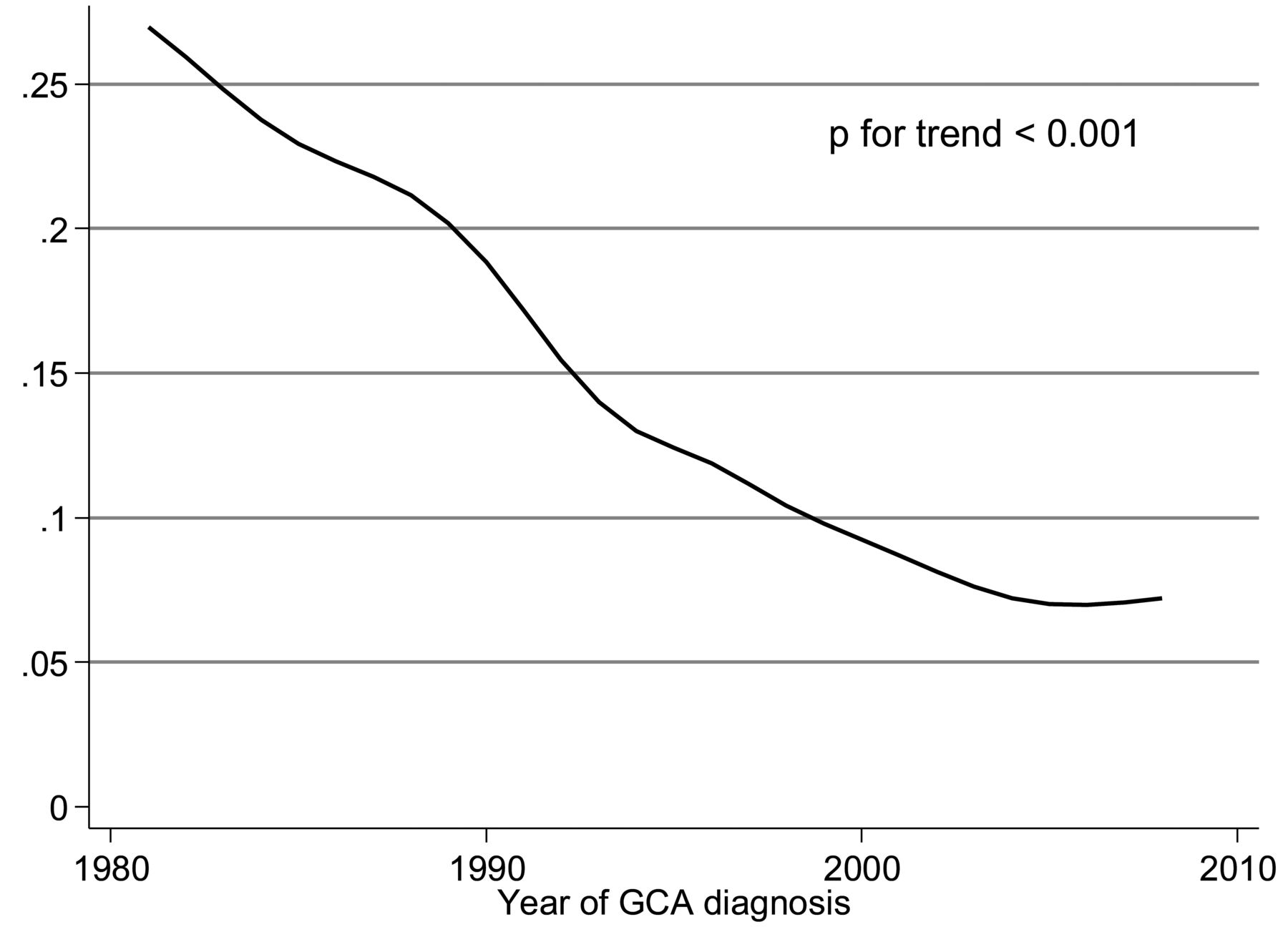
The incidence rate of visual complications in this population-based study was 3 times higher in patients with biopsy-proven GCA than in reference people without GCA from the background population5. However, the frequency of visual ischemic complications, in particular visual loss, was lower than that reported in former population-based studies. In the area of Skåne, visual complications occurred in 10% of the patients with biopsy-proven GCA (85 of 840 cases). Only 18 (21%) of the 85 patients who had visual complications experienced complete visual loss5. It means that in the whole series of 840 patients with GCA, the frequency of permanent visual loss was 2%. Population-based studies published in the last decade described a higher frequency of visual complications6,7. In this regard, visual manifestations developed in 41 (30.1%), and partial or total visual loss in 26 (19.1%) of 136 patients with biopsy-proven GCA diagnosed in Reggio Emilia (Italy) between 1986 and 20026. Visual ischemic manifestations and irreversible visual loss were observed in 57 (22.4%) and 32 (12.5%) of the 255 biopsy-proven GCA cases diagnosed in Lugo (northwest Spain) between 1981 and 20057. It was noteworthy that a negative trend, manifested by a statistically significant progressive decline in the number of patients with visual ischemic manifestations over the 25-year period of study, was observed in Lugo7. A progressive decrease in the number of patients with biopsy-proven GCA who had irreversible visual loss was also found over the same period of study7. Because of that, a significant trend for decline in the frequency of permanent visual loss was also observed7. Figure 1 displays the decreasing trend in the proportion of patients with GCA having permanent visual loss in Lugo from 1981 to 2008. In accordance with Saleh, et al5, we feel that higher physician awareness of GCA may be a plausible explanation for the decrease in the frequency of visual ischemic complications in general, and specifically of permanent visual loss in different parts of the world.
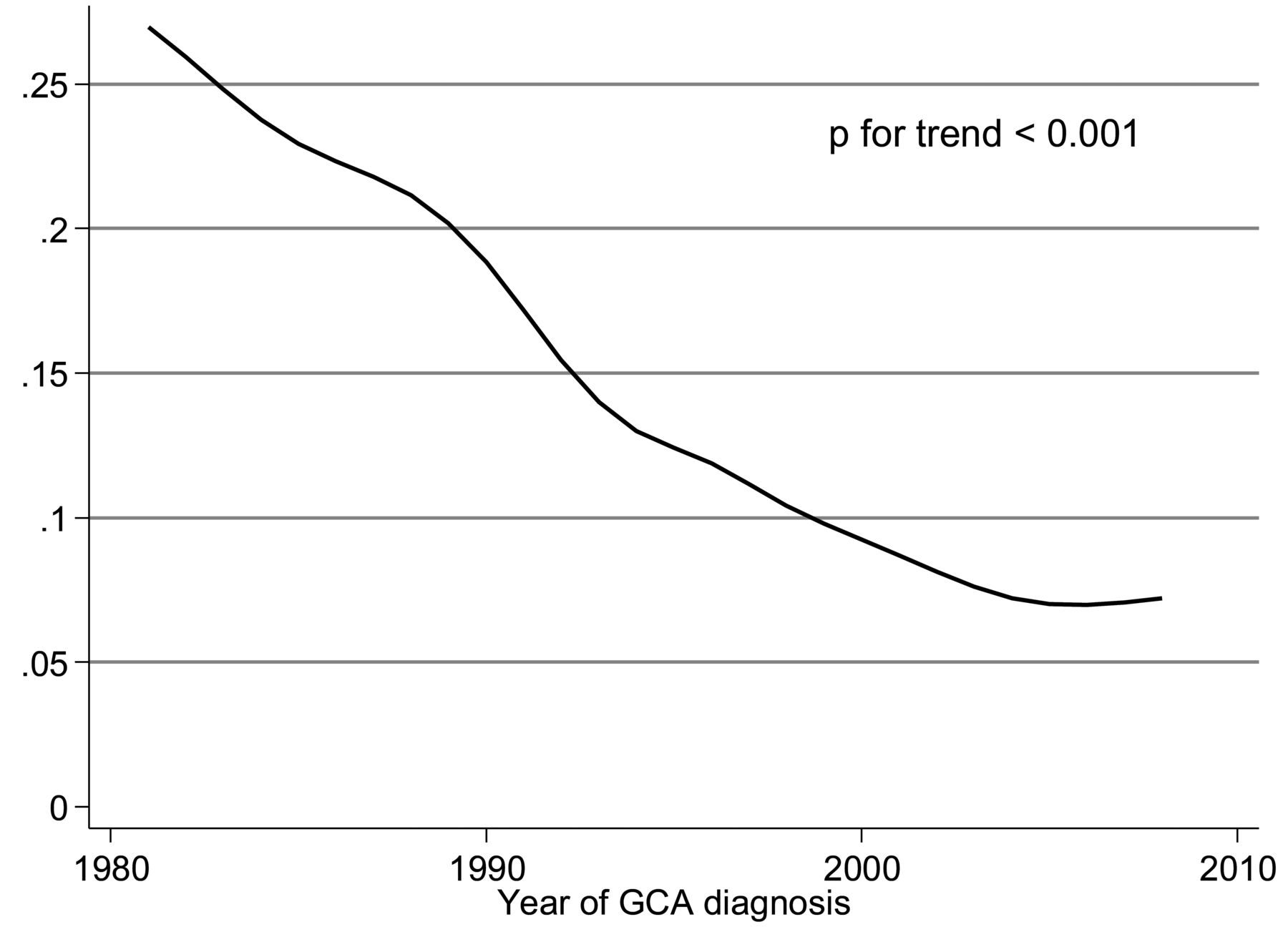
Frequency of permanent visual loss in patients with biopsy-proven GCA from Lugo (northwest Spain) on reappraisal. There was a decreasing trend in the proportion of patients with GCA with permanent visual loss in the Lugo cohort from 1981 to 2008. Results were smoothed using local spline functions. GCA: giant cell arteritis.
A second point of interest addressed by Saleh, et al was the potential influence of predisposing factors for visual ischemic complications in GCA5. Traditional cardiovascular risk factors, in particular the presence of hypertension (HTN) before the onset of the vasculitis, were previously reported to be risk factors for severe ischemic complications in patients with biopsy-proven GCA8. In keeping with that, Saleh, et al disclosed an association between antihypertensive therapies, in particular with β-adrenergic inhibitors, at the time of disease diagnosis and the development of visual complications in biopsy-proven GCA in southern Sweden5. The association may be the result of a confounding by indication effect. Antihypertensive drugs were more commonly given to patients who had an underlying vascular disease before the onset of GCA5. Therefore, the presence of arteriopathy due to HTN could predispose to more severe ischemic events including visual complications of GCA.
Southern Swedish patients with GCA who experienced visual complications had significantly lower C-reactive protein (CRP) levels at disease diagnosis than those without visual complications5. However, to our surprise, no association between erythrocyte sedimentation rate (ESR) and ischemic events was found in this population5. It sounds odd because we observed high correlations among ESR, CRP, hemoglobin, and platelet count in biopsy-proven GCA cases from northwest Spain9. In this region, ESR levels at the time of disease diagnosis were predictors of irreversible visual loss10. An increased risk of visual ischemic manifestations and especially of permanent visual loss was observed in Lugo patients presenting with an ESR ranging between 70 and 100 mm/h10. In agreement with our findings, Salvarani, et al reported ESR values at diagnosis that were significantly lower in patients with biopsy-proven GCA from Reggio Emilia who had permanent visual loss6. By multivariate logistic regression, the absence of high levels of ESR (> 96 mm/h) at the time of disease diagnosis was the best predictor for development of permanent visual loss6. A recent study of this group also indicates that, besides calcifications at temporal artery biopsy, lower CRP values are also predictors for development of permanent visual loss11. Cid, et al also found that the mean ESR was significantly reduced in their patients with irreversible cranial ischemic complications compared with the rest of the patients with biopsy-proven GCA12. The same group provided data supporting the idea that inflammation-induced angiogenic activity could counteract the risk of ischemic complications in patients with GCA13. Patients with a strong systemic inflammatory response had elevated tissue expression of proinflammatory cytokines interleukin (IL)-1β, tumor necrosis factor-α, and IL-613. On the other hand, Weyand, et al demonstrated that temporal artery biopsy specimens from GCA patients with visual ischemic complications express high amounts of interferon (IFN)-γ mRNA14. This cytokine plays an important role in the process of luminal obstruction and in the development of ischemic manifestations of GCA. According to these authors, IFN-γ may dictate the functional properties of other cell populations in the vascular infiltrates and guide the response-to-injury reaction of the artery15.
As pointed out by Saleh, et al, genetic variations may also modulate the risk of visual ischemic complications in patients with GCA5. A large-scale genetic analysis has recently confirmed a strong contribution of the HLA-class II region to GCA susceptibility16. Interestingly, an association of HLA-class II-DRB1*04 with visual complications was reported2,17. Genetic variants associated with high IFN-γ expression18 and others associated with lower expression of the angiogenic vascular endothelial growth factor19 have also been reported to predispose to severe ischemic complications in patients with GCA.
Another issue that deserves further investigation is whether the frequency of visual ischemic manifestations, and therefore the visual outcome, is different in patients with biopsy-proven GCA from that observed in biopsy-negative patients diagnosed with GCA according to well-established classification criteria. A population-based study suggested that the prevalence of severe ischemic complications, including permanent visual loss, may be reduced in biopsy-negative patients when compared with those in whom the diagnosis was confirmed by a positive temporal artery biopsy20.
A final issue is the importance of early onset of therapy to reduce the risk of visual loss in GCA. High-dose corticosteroid therapy must be given to patients presenting with amaurosis fugax because an episode of transient visual loss constitutes the best clinical predictor of irreversible visual loss2. Nevertheless, regardless of the presence of alarm signals, prompt treatment with at least 40 mg/prednisone/day should be prescribed to patients in whom GCA is suspected. A delay in the onset of treatment may have ominous consequences because few patients treated with corticosteroids, either orally or with high-dose methylprednisolone pulses, recover vision once that visual loss is established2.
The study conducted by Saleh, et al supports the claim that, although there is decline in the frequency of visual ischemic complications of GCA, these complications still constitute the leading cause of disability in patients with this vasculitis. The role of HTN prior to the onset of GCA, the degree of inflammatory burden at the time of diagnosis, and the genetic component in the risk of permanent visual loss in patients with GCA warrant further investigation.








{kind=link}