

Abstract
Objective. Vitamin D deficiency, which is common among elderly people, has been linked to muscle weakness. In patients with knee osteoarthritis (OA), the association between muscle strength and serum 25-hydroxy Vitamin D [25(OH)D] level has not been studied comprehensively. The aim of our study was to examine the association between serum 25(OH)D level and muscle strength in patients with knee OA.
Methods. Data of the Amsterdam Osteoarthritis cohort from 319 participants with knee OA were used in a cross-sectional study. Serum 25(OH)D level (nmol/l) was measured by a competitive electrochemiluminescence method. Muscle strength (nm/kg) of the upper leg was measured isokinetically. Univariable and multivariable linear regression analyses were used to calculate the association between serum 25(OH)D level and muscle strength.
Results. Serum 25(OH)D level was significantly associated with muscle strength (B = 0.036, 95% CI 0.017–0.054, p < 0.001), adjusted for season of blood collection. After adding body mass index (BMI) to the model, this association was no longer significant (B = 0.011, 95% CI −0.007 to 0.029, p = 0.214). Alcohol consumption, number of comorbidities, and sex were subsequently added and changed the model slightly. Without BMI, this model showed a significant association between serum 25(OH)D level and muscle strength (B = 0.029, 95% CI 0.014–0.043, p < 0.001).
Conclusion. The observed association between a low serum 25(OH)D level and muscle weakness in patients with knee OA is attenuated by BMI. Further studies are needed to explain the associations among Vitamin D level, muscle strength, and adiposity in patients with knee OA.
Muscle weakness is a well-established risk factor for activity limitations in patients with knee osteoarthritis (OA)1,2. Determinants of muscle weakness in patients with knee OA include knee pain, disuse, aging, and low-grade inflammation3. In addition, vitamin D deficiency has been linked to muscle weakness because of its direct and indirect effects on muscle cells4. The main source of vitamin D is ultraviolet radiation (UV), which synthesizes pre-vitamin D in the skin. Bound to the vitamin D binding protein, pre-vitamin D is transported to the liver where it is hydroxylated into 25(OH)D. Serum 25(OH)D level is generally measured to assess vitamin D status5.
The relationship between serum 25(OH)D level and muscle strength in patients with knee OA has been studied only once, to our knowledge6. This relatively small study, containing 56 participants younger than 60 years with knee OA and muscle weakness, showed that participants with vitamin D deficiency (< 50 nmol/l) had significantly lower quadriceps strength compared to participants with a non-deficient serum 25(OH)D level. Vitamin D deficiency has also been related to pain and radiological progression in patients with knee OA7,8,9, although no effect of supplementation could be detected on these outcomes10.
The observed relationship between vitamin D and muscle strength in knee OA is in line with several observational studies in general populations. A recent systematic review demonstrated that vitamin D deficiency, or hypovitaminosis D, was consistently associated with decrease in muscle function and performance and increase in disability in all ages except for very old individuals11. As to the effect of vitamin D supplementation on muscle strength, there is evidence from a systematic review and metaanalysis that vitamin D supplementation has a small positive effect on muscle strength12. Subgroup analysis showed a greater effect of vitamin D supplementation in subjects with a baseline serum 25(OH)D level below 30 nmol/l.
Evidence for the role of vitamin D on muscle strength is accumulating, but studies in patients with knee OA are scarce. Because muscle weakness is common in knee OA and of clinical importance, optimizing muscle strength is a focus of rehabilitation in these patients. The association between vitamin D and muscle strength in this population should be clarified to reveal whether low serum 25(OH)D level is a determinant of muscle strength that could be targeted. We hypothesized that a low level of serum 25(OH)D (≤ 50 nmol/l)13,14,15 is associated with muscle weakness in patients with knee OA.
The aim of our present study was to examine the cross-sectional association between serum 25(OH)D level and muscle strength in patients with knee OA in a large cohort, taking possible confounders into account.
MATERIALS AND METHODS
Study sample
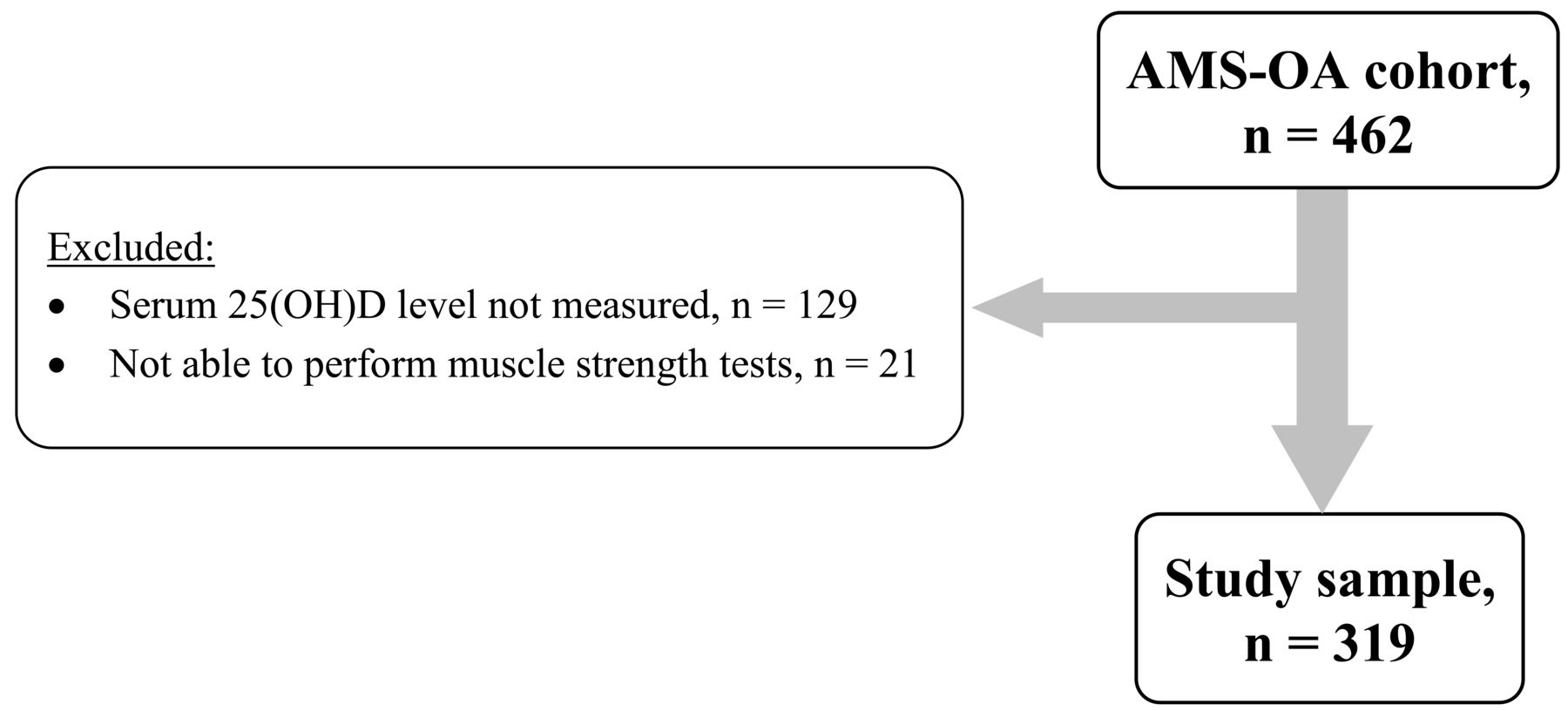
Data were collected from the Amsterdam Osteoarthritis cohort, made up of participants with a clinical diagnosis of OA of the knee and/or hip according to the American College of Rheumatology criteria16 and who have been referred to an outpatient rehabilitation center (Reade, Centre for Rehabilitation and Rheumatology; Amsterdam, the Netherlands). Participants with OA of the knee and complete data of serum 25(OH)D level and muscle strength were included in our present study (Figure 1). Exclusion criteria were total knee replacement or presence of rheumatoid arthritis or any other inflammatory arthritis (i.e., septic arthritis, crystal arthropathy/gout, or spondyloarthropathy). Patients were assessed by rheumatologists, radiologists, and rehabilitation physicians. Rheumatologists established the diagnosis of knee OA and checked the exclusion criteria. Radiologists scored the radiographs of the knee, and rehabilitation physicians assessed the patients on functioning. Demographic, radiographic, biomechanical, clinical, and psychosocial factors related to OA were assessed at the baseline visit to the rehabilitation center. Each participant provided written informed consent according to the declaration of Helsinki. The study was approved by the Medical Ethical Institutional Review Board of Reade. The sample for this study comprises patients recruited between January 2009 and June 2013.

Scheme showing the total study sample and the exclusion of patients with knee osteoarthritis. AMS-OA: Amsterdam Osteoarthritis; 25(OH)D: 25-hydroxy vitamin D.
Measurements
In non-fasting blood samples collected by venapuncture, 25-hydroxy vitamin D was measured. The serum was centrifuged and stored at −20°C. The blood samples were analyzed by a Roche Cobas-6000 analyzer [COBAS 25(OH)D total] using a competitive electrochemiluminescence method to measure serum 25(OH)D level. The interassay coefficient of variation was < 6%. The 25(OH)D was released from its binding plasma protein and afterward 25(OH)D was incubated with 25(OH)D binding protein labeled with ruthenium, creating a complex with 25(OH)D and ruthenylated vitamin D binding protein17. The level of 25(OH)D in nmol/l was used for analyses.
Muscle strength
Muscle strength was tested using an isokinetic dynamometer (EnKnee, Enraf-Nonius), which measured extension and flexion of the knee at 60°/s18. The participants performed 12 repetitions in total: 3 repetitions per leg for knee extension and 3 repetitions per leg for knee flexion. The average of knee flexor strength and knee extensor strength of both legs was used in the analyses, representing upper leg muscle strength2. Average muscle strength of both legs was used because we hypothesized vitamin D deficiency would affect muscle strength in both legs and because the correlation between muscle strength of the right and left leg was high (r > 0.75). Muscle strength was adjusted for body weight (nm/kg).
Potential confounders
Based on previous studies investigating the relationship between serum 25(OH)D level and muscle strength in older adults19,20,21,22,23,24,25, the following potential confounders were considered relevant: season of blood collection, age, sex, body mass index (BMI), smoking habits, alcohol consumption, creatinine level, and number of comorbidities. Season of blood collection was dichotomized into summer (April–September) and winter (October–March)5,13,23. Age was calculated from date of birth at the start of inclusion. BMI was calculated as body mass in kg divided by the square of height in meters (kg/m2). Information on current smoking was assessed by a questionnaire and was reported as “yes” or “no.” Alcohol consumption was also assessed by a questionnaire and was classified into “never,” “ ≤ 8 consumptions per week,” and “ > 8 consumptions per week.” Creatinine level (in μmol/l) was measured by a Roche Cobas-6000 analyzer. The Cumulative Illness Rating Scale was used to collect information about the presence of chronic diseases. This rating scale gathers information related to 13 body systems that can each be scored from 0 (none) to 4 (very severe). The number of body systems on which a patient scored 2 or higher was calculated and used in analyses.
Specific for the knee OA population, the following additional confounders were considered26,27: erythrocyte sedimentation rate (ESR; in mm/h) and C-reactive protein (CRP; in mg/l). ESR values were determined by the standard Westergren method28. The rate at which red blood cells sedimented in 1 h was measured and reported in mm/h. ESR was used as a dichotomized variable (≤ 20 mm/h and > 20 mm/h)26. CRP was analyzed using turbidimetric immunoassay with CRPLX test kits29 and was dichotomized (≤ 3 mg/l and > 3 mg/l)26.
Other variables
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) subscales of pain and physical functioning were used descriptively. The WOMAC is a self-administered questionnaire to assess pain, stiffness, and physical function in patients with hip and/or knee OA30,31. WOMAC pain subscale was scored from 0 to 20 and WOMAC physical function subscale was scored from 0 to 68; higher scores represent more pain or activity limitations, respectively. Severity of radiological damage [Kellgren-Lawrence scale (KL)] was also assessed and used descriptively in our study. Radiographs of the tibiofemoral (medial and lateral) joints were made using a weight-bearing posterior-anterior view, semiflexed (7°–10°) according to Buckland-Wright, et al32. The radiographic features (joint space narrowing, osteophyte formation, sclerosis, cysts) within the tibiofemoral joints were scored according to the Osteoarthritis Research Society International atlas in KL grades33. Scoring of the KL grades was in 5 categories (0–4). Grade 0 represents no osteoarthritic features while grade 4 represents severe joint space narrowing, large osteophyte formation, sclerosis, and cysts.
Statistical analyses
Baseline characteristics for continuous variables [age, BMI, creatinine level, WOMAC physical functioning and pain subscales, muscle strength, and serum 25(OH)D level] were checked for normal distribution and reported as mean, SD, and min/max scores. Categorical variables (sex, season, smoking habits, alcohol consumption, no. comorbidities, ESR, CRP, and KL grade) were reported as percentages. Deficiency was labeled as a serum 25(OH)D level ≤ 50 nmol/l13,14,15, and chi-squared tests and independent t tests were used to compare the patients with deficient levels and those without. To assess the association between muscle strength and serum 25(OH)D level, univariable linear regression analysis was performed. Muscle strength was used as a continuous variable whereas serum 25(OH)D level was used both continuously (10-unit change) and dichotomously (deficient vs non-deficient). The reported regression coefficients (B) represent the change in muscle strength by each 10-unit change of serum 25(OH)D level and the difference in muscle strength of being deficient vs being nondeficient, respectively. Also, the standardized regression coefficient (β) was reported, to assess the effect of various variables on this association in a standardized unit. In multivariable regression analyses, potential confounders were added stepwise into the model. First, season of blood collection was added to the model and was left in the model when testing other potential confounding variables. Variables that changed the regression coefficient (B) of serum 25(OH)D level by more than 10% were considered confounders. Interactions between age and serum 25(OH)D level and BMI and serum 25(OH)D level were considered plausible and were therefore tested. For this purpose, age was dichotomized into ≤ 60 vs > 60 years and BMI into ≤ 30 vs > 30 kg/m2.
The same analyses were repeated using 75 nmol/l instead of 50 nmol/l as cutoff value for vitamin D deficiency13,14,15, as well as analyses with extension and flexion strength separately. Data were analyzed using SPSS version 22. A p value ≤ 0.05 was considered significant.
RESULTS
The study sample comprised 319 participants (66.5% women) with a mean age of 60.5 (± 8.3) years (range 33–78 yrs). Table 1 shows the characteristics of the total sample, the deficient group [serum 25(OH)D level ≤ 50 nmol/l], and the non-deficient group [serum 25(OH)D level > 50 nmol/l]. Overall, the mean serum 25(OH)D level was 60.8 (± 24.6) nmol/l (range 8–135), with 36.1% of the participants being deficient according to the cutoff point of ≤ 50 nmol/l. Using a higher cutoff point (75 nmol/l)13, deficiency was observed in 72.7% of the participants. Compared to the participants with a serum 25(OH)D level > 50 nmol/l, participants with a serum 25(OH)D level < 50 nmol/l showed lower muscle strength (p = 0.008), higher BMI (p < 0.001), higher ESR (p = 0.011), higher CRP (p < 0.001), and worse physical functioning (p = 0.028). In addition, 25(OH)D deficiency was more common in the winter season than in the summer season. Excluded participants [because of unknown serum 25(OH)D level (n = 129) and absence of data on muscle strength (n = 21); pain (n = 3), lack of strength (n = 10), and unknown (n = 8)] had a higher mean age (p = 0.002), worse physical functioning (p = 0.002), and higher pain scores (p = 0.043).
Description of the characteristics of the total study sample and the differences of characteristics between deficient and nondeficient serum 25(OH)D levels in patients with knee osteoarthritis. Data are mean ± SD (min–max) unless otherwise specified.
Table 2 shows the results of the univariable and multivariable linear regression analyses. Serum 25(OH)D level was significantly associated with muscle strength (B = 0.032, 95% CI 0.014–0.050, p < 0.001) in univariable analysis. Muscle strength remained significantly associated with serum 25(OH)D level after adjusting for season of blood collection (B = 0.036, 95% CI 0.017–0.054, p < 0.001; Model 1). When adding BMI to this model, the association between serum 25(OH)D level and muscle strength was no longer significant (B = 0.011, 95% CI −0.007 to 0.029, p = 0.214; Model 2). Model 3, adjusted for season of blood collection, BMI, alcohol consumption, number of comorbidities, and sex, was slightly different from Model 2 (B = 0.013, 95% CI −0.002 to 0.027, p = 0.083). In Model 4, the same confounding factors as in Model 3 were incorporated, except for BMI. This model showed a significant association between serum 25(OH)D level and muscle strength (B = 0.029, 95% CI 0.014–0.043, p < 0.001). Age, smoking habits, serum creatinine, ESR, and CRP did not change the regression coefficient > 10% in this model and were therefore omitted from the model. Higher BMI was associated with lower serum 25(OH)D levels (standardized β −0.340, p < 0.001) and lower muscle strength (standardized β−0.448, p < 0.001). No interaction effect between serum 25(OH)D level and age or serum 25(OH)D level and BMI was observed.
Results of the regression analyses of serum 25(OH)D level on upper leg muscle strength, adjusted for potential confounders.
Analyses with 75 nmol/l, instead of 50 nmol/l, as a cutoff value for vitamin D deficiency, as well as analyses with extension and flexion strength separately showed similar results. Further, the frequency of missing data was not different between vitamin D deficient and vitamin D non-deficient participants (Table 1). Univariable and multivariable linear regression analyses using data from participants who had no missing data (n = 293) gave similar results (data not shown).
DISCUSSION
Our present study was the first, to our knowledge, to investigate the relationship between serum 25(OH)D level and upper leg strength in a large sample of patients with knee OA. A statistically significant association between a low serum 25(OH)D level and muscle weakness was found. However, this association was attenuated by BMI.
The observed association between serum 25(OH)D level and muscle strength is in line with the relatively small study by Barker, et al6. Compared to that study, a larger sample of patients with knee OA was included in our present study. Further, in contrast to the study of Barker, et al, the association between serum 25(OH)D level and muscle strength was adjusted for several potential confounding factors. Our results showed that the difference between muscle strength in the deficient and nondeficient group was 0.12 nm/kg, indicating a 15% higher muscle strength in the nondeficient group compared to the deficient group. In exercise trials in knee OA, an average increase in muscle strength of 17% was found, which led to improvements in daily functioning34. We therefore believe that the difference in muscle strength between these groups is of clinical relevance.
Interestingly, BMI strongly affected the association between serum 25(OH)D level and muscle strength and the association was no longer significant when BMI was incorporated into the model. This may be explained by the established association between BMI and muscle strength in knee OA35 and the finding that a reduction in BMI by weight loss resulted in higher muscle strength36. This suggests that BMI has a strong influence on muscle strength, particular in patients with knee OA who have a high BMI (our study sample), which may be the result of fatty infiltration of muscle tissue. Moreover, it is known that 25(OH)D is stored in adipose tissue, because of its lipophilic character37,38. More adipose tissue could consequently result in lower levels of 25(OH)D in serum. In that way, BMI could act as a preceding factor in this association, instead of a confounding factor, causing overcorrection of the model. In future research, stratifying by BMI in the analyses should be encouraged. Other causes for the effect of BMI could be that obese patients may be exposed to sunshine less frequently, owing to limited mobility or clothing habits, or that 25(OH)D production and metabolism are altered in obesity37,38. Further studies are needed to investigate the influence of various factors39, including BMI, on 25(OH)D.
Some limitations of our study have to be considered. First, a cross-sectional study design was used and a causal relationship cannot be established. For causal relationships, an experimental study design is needed. Second, no outdoor activity variable was available in our data. In patients with knee OA, muscle weakness may reduce outdoor activities, which may affect the 25(OH)D level (shortage in UV-exposure) resulting in a lower serum 25(OH)D level. Third, muscle strength was adjusted for body weight (nm/kg). Because muscle strength was adjusted for body weight and BMI was added as a confounding factor into the model, body weight was corrected twice in the model. Because of this double correction, the regression analyses were repeated with muscle strength in Newton meter, showing similar results (data not shown). Further, the majority of the participants excluded because of absence of data on muscle strength (n = 21) had vitamin D deficiency. If these participants were included, this could have increased the between-group difference in muscle strength. Finally, the serum 25(OH)D level was measured by a Roche Cobas-6000 analyzer. Janssen, et al40 compared several methods — including the Roche Cobas analyzer — with the gold standard (ID–LC–MS/MS) to measure 25(OH)D level in serum. Overall, the Roche Cobas analyzer showed no significant differences in serum 25(OH)D level measured compared to the gold standard. On the other hand, at increasing levels of serum 25(OH)D, it showed an increasing measurement error. Therefore, this method of measuring serum 25(OH)D level could have affected the vitamin D status measured in our study. However, the average serum 25(OH)D level of our study sample was similar to serum 25(OH)D levels presented in other studies in the same age group in Western Europe37,39,41,42.
Because muscle strength is a risk factor for activity limitation in patients with knee OA1,2, it is important to increase the effectiveness of muscle strengthening exercises in patients with knee OA. According to our results, serum 25(OH)D level could be a factor affecting muscle strength and could therefore be of additive value in the management of patients with knee OA.
The observed association between a low serum 25(OH)D level and muscle weakness in patients with knee OA is attenuated by BMI. Further studies are needed to explain the associations between muscle strength, 25(OH)D, and adiposity in patients with knee OA.
Acknowledgment
We gratefully acknowledge S. Romviel, M. Steenbergen, M. Crins, I. Schaffers, and S. Webster for collecting data.
- Accepted for publication April 8, 2016.








{kind=link}