

Abstract
Objective. To study the change in the modified Hand Mobility in Scleroderma (mHAMIS) test from early to advanced stages of systemic sclerosis (SSc), and the relationship between mHAMIS and skin involvement during followup.
Methods. This retrospective study includes 65 patients with baseline disease duration of ≤ 3 years who were assessed with the mHAMIS test at baseline and at 1 or 2 predefined followup points (3.1–5 yrs and 5.1–9 yrs after disease onset). Studied measures were the modified Rodnan skin score (mRSS), mRSS of the hand, serum cartilage oligomeric matrix protein, and digital vascular lesions.
Results. The mHAMIS and the mRSS hand changed synchronously during the first 5 years after disease onset (rs = 0.44, p = 0.001). In the group with high mHAMIS at baseline, both mHAMIS and mRSS hand improved significantly at the first followup (p < 0.05), and the improvement sustained during the followup in the mRSS hand. Patients with antitopoisomerase I and anti-RNA polymerase III antibodies had significantly higher mHAMIS at baseline (p = 0.003) and at the second followup (p = 0.030) compared to patients with anticentromere antibodies. Patients with digital vascular lesions at baseline had significantly higher mHAMIS during the followup (p < 0.05) compared to patients without. The mHAMIS improved significantly during the followup in patients with immunosuppressive treatment in early disease (p < 0.05), but not in patients without this treatment.
Conclusion. The mHAMIS reflects disease activity in fibrosis in early stages of SSc. In later stages it can be regarded as a measure of damage arising from fibrotic and vascular involvement, making it suitable as an endpoint in followup examinations
Systemic sclerosis (SSc; scleroderma) is an autoimmune disease characterized by microvascular injury and excessive fibrosis of the skin and internal organs1. Skin involvement is a manifest consequence of SSc, and correlates well with organ involvement2. Three phases of skin involvement can be identified: the edematous phase, with increased amounts of interstitial fluid; the indurative phase, during which collagen is deposited in the skin resulting in stiffness; and the atrophic phase, with thinning of the abnormal skin. In the atrophic phase, tautness of the skin may remain in some cases despite low or no disease activity3. Skin thickness is often determined using the modified Rodnan skin score (mRSS)4, which provides a measure of the skin involvement of the whole surface of the body. The mRSS reflects the severity of fibrotic skin involvement but it is unclear whether it can be used to assess disease activity. Further, the mRSS has some shortcomings related to interobserver variability5,6 and the inability to distinguish between skin thickness and tightness, especially in the fingers during the atrophic phase. It is, however, possible that biomarkers such as serum cartilage oligomeric matrix protein (COMP) could be used to monitor disease activity related to fibrosis7.
The hands account for only a small fraction of the total skin area of the body, but skin involvement of the hands is related to limitations in hand mobility and activities of daily life8,9,10,11,12. Because hand involvement is one of the early signs of the disease, it is important to study hand involvement separately, especially in studies on the outcome of therapy. Although the pathological processes involved in SSc are not yet fully understood, it is possible that a specific kind of treatment affects only fibrotic manifestations. If this is indeed the case, it is important to use tools that specifically measure fibrotic involvement and the functional consequences of fibrosis.
The Hand Mobility in Scleroderma (HAMIS) test13 has been used in assessment of hand function in SSc13,14. The test can be administered by professionals with special knowledge of hand function and SSc such as occupational therapists, physiotherapists, physicians, or research nurses. HAMIS consists of differently sized grips and movements evaluating mobility in fingers and wrist usually assessed in an ordinary range-of-motion test. Finger items are flexion, extension, abduction, and abduction of the thumb. Wrist items are pronation, supination, dorsal extension, and palmar flexion. Advantages of the HAMIS test are the feasibility and the high interobserver and intraobserver reliability13. The HAMIS test reflects the consequences of skin involvement, in moderate and significant correlation with mRSS in early disease. However, there is no obvious relationship between mRSS and HAMIS in advanced disease when the skin is tight but thin10,15,16. Our research group recently presented an item-reduced HAMIS test called modified HAMIS (mHAMIS). The mHAMIS is composed of 4 out of the 9 items from the original HAMIS. The items in mHAMIS are finger flexion, finger extension, finger abduction, and dorsal extension. The mHAMIS has shown significant correlations with mRSS and hand skin score, as well as the ability to discriminate between limited cutaneous SSc (lcSSc) and diffuse cutaneous SSc (dcSSc) in the first 3 years after disease onset15. These results demonstrated the mHAMIS test’s usefulness in evaluating the consequences of skin involvement in the early stages of the disease when information is needed concerning appropriate therapy, but the test’s properties in a longitudinal perspective are unclear. The aim of our present study was to examine the change of mHAMIS from early to advanced SSc, and the mHAMIS relationship with skin involvement during longterm followup.
MATERIALS AND METHODS
Subjects
All patients were included, within the context of our regular followup program, who were assessed with the mHAMIS test within the first 3 years of disease onset and at least once more during followup, and who fulfilled the American College of Rheumatology criteria for SSc17. The study group consisted of 65 patients (47 with lcSSc and 18 with dcSSc). Disease onset was defined as the time of first non-Raynaud manifestation. The relevant clinical characteristics of the patients are presented in Table 1.
Baseline characteristics of the 65 patients with systemic sclerosis. Data are n (%) unless otherwise indicated.
Study design
This longitudinal study was based on measurements between 1998 and 2011. Data were split into 2 followup points in relation to disease duration at followup: 3.1 to 5 years, and 5.1 to 9 years after disease onset. Patients may have assessments in 1 or more of these groups, and may also have multiple assessments in the same group. Therefore, to avoid possible duplication of data, the patient’s middle assessment was used in the first followup and the last assessment in the second followup.
Ethical considerations
Our study was conducted in accordance with the Declaration of Helsinki, and was approved by the Regional Ethics Committee in Lund. The patients were given verbal information on the aim of the study, and written consent was obtained.
Instruments
The patients’ skin involvement was characterized by subdivision into lcSSc and dcSSc, measurement of the mRSS total skin score based on palpation of 17 anatomic sites4, and a subscore measuring skin involvement on the fingers, the hands, and the forearms (here referred to as mRSS hand). The mRSS hand was assessed separately in both hands, giving an mRSS hand score of 0 to 18 points. Digital vascular lesions were defined as digital tip ulcerations or pitting scars. Serum COMP was measured with a commercial sandwich ELISA using 2 monoclonal antibodies directed against separate antigenic determinants (AnaMar). The detection limit is 0.1 u/l and the intraassay and interassay coefficient of variation is < 5%. Hand mobility was assessed with the mHAMIS test. Both hands were assessed separately, giving an mHAMIS score of 0 to 24 points15. These objective disease variables were assessed within the context of our regular followup program.
Statistical analysis
Because of the sample size and distribution, nonparametric analyses were used. Data were presented as median and interquartile range (IQR), and as numbers and percentages. The changes in the mHAMIS test were analyzed on an individual basis as well as on a group level. On an individual basis, a change of 6 points for mHAMIS and 5 points for mRSS hand was deemed clinically relevant. The cutoff was determined before analyzing data and was exclusively determined on the basis of our clinical experience of what is a noticeable change. We consider that a change of mHAMIS of 6 points out of 24 possible in a test involving 8 items is an obvious difference that is of value to the patient. The same argument was made for mRSS hand: 5 points out of 18 possible in a test involving 6 measuring points ought to make a difference for the patient. A difference of < 2 points in both instruments was classified as unchanged. To further investigate the change of the mHAMIS test, the subjects were divided into 2 subgroups according to the mean of the mHAMIS score at baseline: supramedian is a median value of 6 points or more, and inframedian is < 6 points. The Wilcoxon signed-rank test was used to test for differences between the baseline and the followup, and the Mann–Whitney U test was used for comparison between 2 groups. Associations between variables were analyzed using the Spearman’s correlation. P values < 0.05 were considered statistically significant.
RESULTS
Hand mobility, skin involvement, and serum COMP in a longitudinal perspective
Of the 65 patients with mHAMIS measures at baseline, 52 had been assessed a second time within 3.1 to 5 years after disease onset, and 46 of the 65 patients had been assessed within 5.1 to 9 years after disease onset. Because the assessments took place during clinical care, the time between assessments varied from patient to patient. Baseline measures were assessed in median (IQR) 1.5 (0.8–2.2) years after disease onset, the first followup was 4.1 (3.6–5.0) years after disease onset, and the second followup 6.7 (6–7.8) years after disease onset. The time between baseline and the first followup was 2.6 (1.9–3.1) years and between baseline and the second followup, 5.1 (4.3–6.6) years.
In the individual analysis we found that mHAMIS changed in about 45% of the patients at both followup points. At the first followup, a larger number of patients had improved than worsened, while the proportion was relatively similar at the second followup. The mRSS hand improved in about 43% of patients. Most of them had a clinically relevant improvement at the second followup (Figure 1).
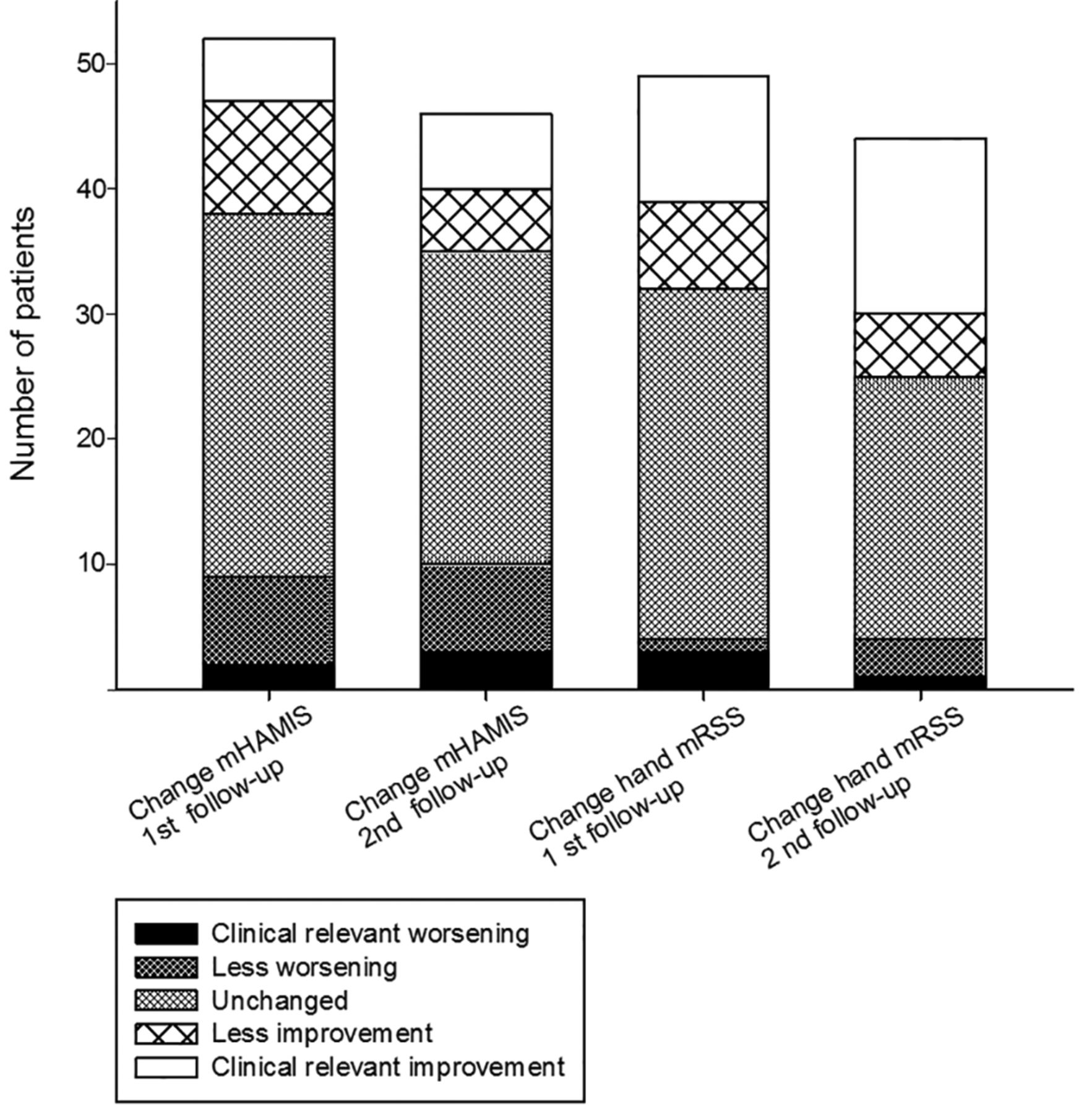
Progress of individual basis of mHAMIS and mRSS hand during the followup. mHAMIS: modified Hand Mobility in Scleroderma test; mRSS: modified Rodnan skin score.
Skin involvement, including mRSS and mRSS hand, improved significantly from baseline to the first and to the second followup points (p < 0.01; Table 2). Serum COMP improved significantly between baseline and the second followup (p = 0.003), while mHAMIS did not change significantly between baseline and the followup (between baseline and first followup, p = 0.068, and between baseline and second followup, p = 0.688; Table 2).
Skin involvement, hand mobility, and serum COMP at baseline and the evolution during the followup. Except for number data, data are median (IQR). Negative change in values = improvement.
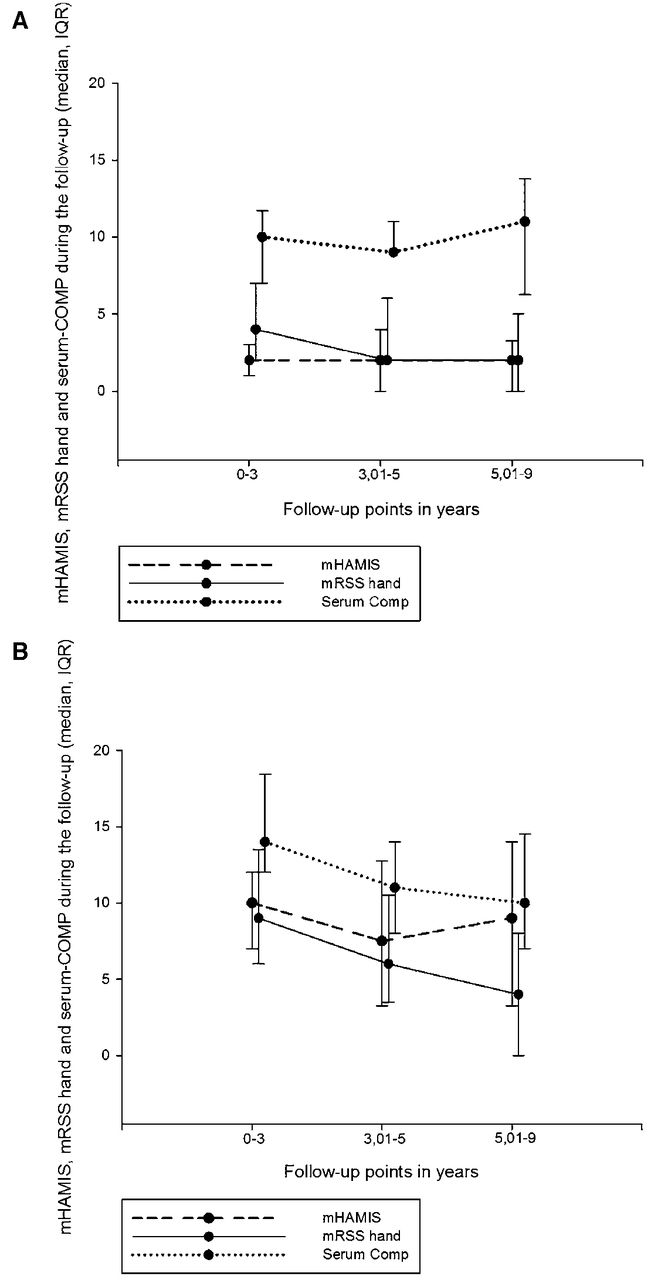
The patients were divided into 2 groups depending on the mHAMIS score at baseline. In the inframedian group, the mHAMIS was in median (IQR) 2.0 (1–3) and mRSS hand was 4.6 (2–7). Both mHAMIS and mRSS hand were stable during the followup and did not change significantly (mHAMIS: between baseline and first followup, p = 0.480, and between baseline and second followup, p = 0.520; in mRSS hand the corresponding p values were 0.361 and 0.104, respectively; Figure 2A). In the supramedian group, into which the majority of patients with dcSSc fell, the median (IQR) of mHAMIS was 10 (7–12), and 9 (6–13.5) in mRSS hand. During the first 5 years after disease onset, mHAMIS and mRSS hand changed synchronously, but not in the later stage (Figure 2B). There was a significant improvement in mHAMIS between baseline and the first followup (−2, −5 to 0; p = 0.024), but not between baseline and the second followup (−1.5, −6.8 to 2; p = 0.420). A negative value indicates improvement. The mRSS hand improved significantly at both the first followup (−2, −4.5 to 0; p = 0.004) and the second (−4, −8 to −2; p = 0.001).
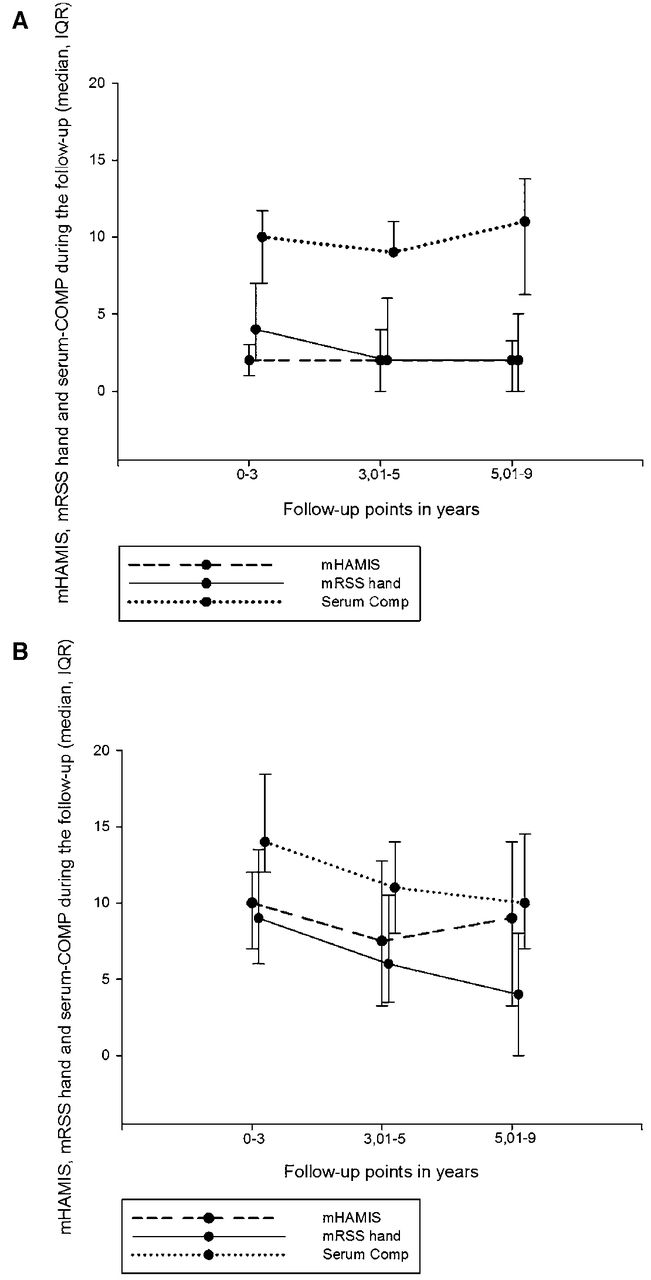
A. Longitudinal followup of mHAMIS, mRSS hand, and serum COMP in patients with low mHAMIS at baseline. B. Longitudinal followup of mHAMIS, mRSS hand, and serum COMP in patients with high mHAMIS at baseline. mHAMIS: modified Hand Mobility in Scleroderma test; mRSS: modified Rodnan skin score; COMP: cartilage oligomeric matrix protein; IQR: interquartile range.
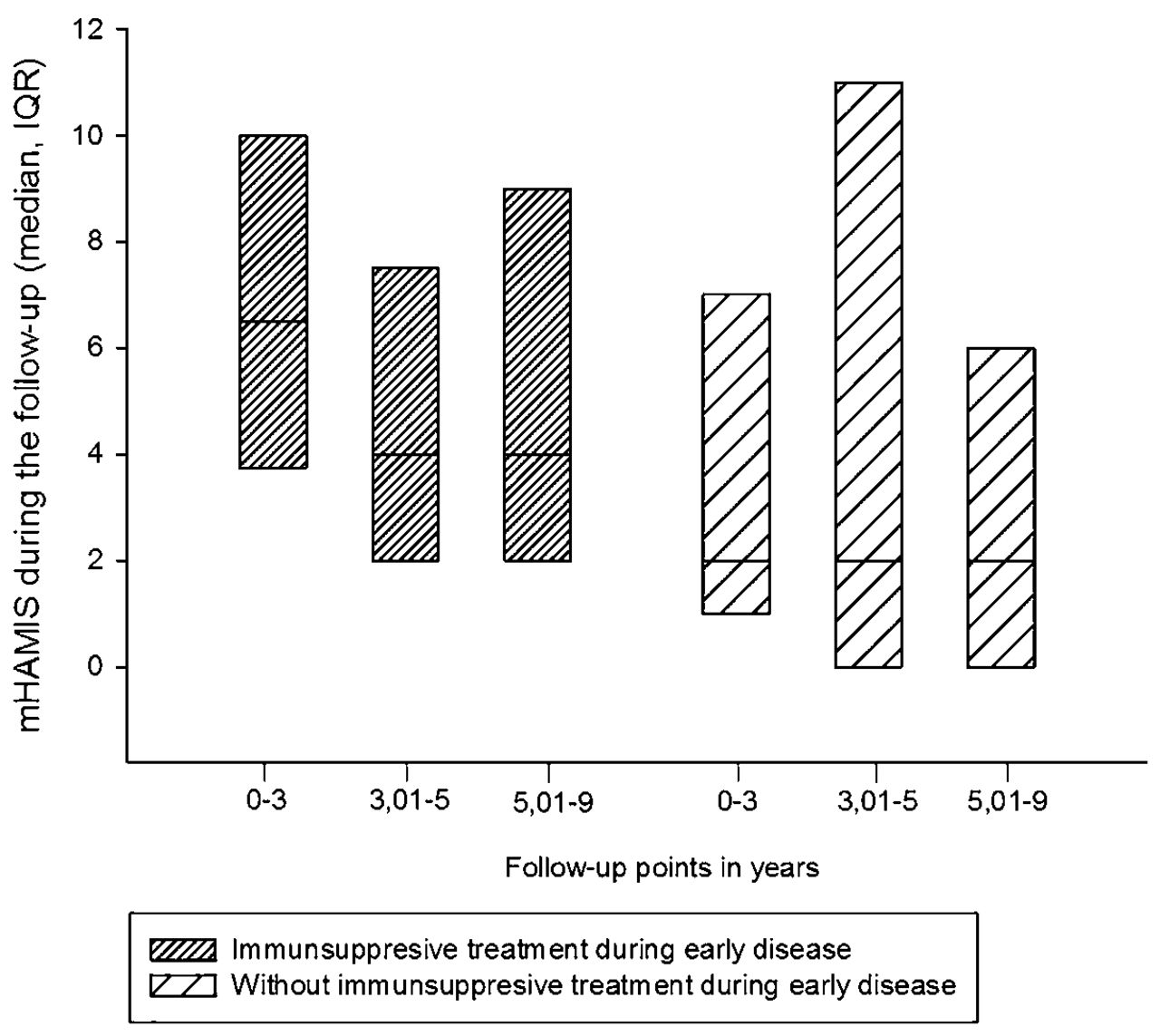
Patients with immunosuppressive treatment at baseline and first followup had significantly higher mHAMIS and mRSS hand scores compared to patients without this treatment. The mHAMIS was 6 (3.5–10) compared to 2 (1–9), p = 0.029, and mRSS hand 7 (5.3– 10.8) compared to 4 (2–8.5), p = 0.032. Patients with immunosuppressive treatment in this early stage improved significantly in mHAMIS between baseline and the first followup (p = 0.005) and between baseline and the second followup (p = 0.011). Patients without this treatment did not change either way. The change was between baseline and first followup (p = 0.430), and between baseline and second followup (p = 0.107; Figure 3). In patients with immunosuppressive treatment, the mRSS hand changed significantly between baseline and the first followup (p = 0.008) and between baseline and the second followup (p = 0.0001). In the group without treatment, corresponding p values for change were p = 0.763 and p = 0.428 (data on change in mRSS hand not shown).

Longitudinal followup of mHAMIS in patients with and without immunosuppressive treatment in early disease. IQR: interquartile range; mHAMIS: modified Hand Mobility in Scleroderma test.
Associations between mHAMIS and mRSS hand, mRSS, serum COMP, and digital vascular lesions
The mHAMIS baseline values and the Δ values at the first followup were significantly correlated with baseline and Δ values of mRSS hand, and serum COMP (Table 3). The mRSS hand at baseline correlated significantly with mHAMIS at the first and second followup [rs = 0.54 (p = 0.001) and rs = 0.64 (p = 0.001), respectively]. This was interpreted as fibrotic skin and high disease activity in early disease causing high mHAMIS, i.e., impaired hand mobility in a later stage.
Correlations at baseline and the change between baseline and followup (Δ values) between mHAMIS and mRSS hand, and serum COMP.
Patients with dcSSc had significantly higher mHAMIS at baseline, in lcSSc 3 (1–7) compared to dcSSc 8 (4.5–12.8), p = 0.002, and in mRSS hand, 5 (2–8) in lcSSc compared to 11 (6–14) in dcSSc (p = 0.001). There were, however, no differences in changes between lcSSc and dcSSc, neither of mHAMIS nor of mRSS hand at the followup. The change of mHAMIS at the first followup was −1.5 (−2.3 to 2) in lcSSc and −1 (−3.3 to 0.8) in dcSSc. At the second followup, the corresponding values were 0 (−3 to 0.8) in lcSSc and 0 (−2 to 0) in dcSSc. The change of mRSS hand at the first followup was −1 (−3.8 to 0) in lcSSc and 0 (−5 to 1.5) in dcSSc. At the second followup the change was −2 (−6 to −1) in lcSSc and −2 (−9 to 2) in dcSSc.
Patients with antitopoisomerase I (ATA) and anti-RNA polymerase III antibodies (ARA) had significantly higher mHAMIS scores at baseline and at the second followup compared to patients with anticentromere antibodies (ACA). Scores for mHAMIS in patients with ATA and ARA at baseline in median (IQR) were 8 (6.5–10.5) compared to 2 (1 – 6; p = 0.003) in ACA. In the second followup, the values were 8.5 (4.8–13.5) in ATA and ARA compared to 2 (0–6), p = 0.030, in ACA. Compared to patients without lesions, those with digital vascular lesions at baseline had significantly higher mHAMIS at first followup: 7 (2.8–14.8) vs 2.5 (0–6.3), p = 0.006; and at second followup 6 (2.8–14) vs 2 (0–4.8), p = 0.011. Compared to those without vascular lesions, patients with vascular lesions also had higher mRSS hand at baseline: 8 (6–12) vs 4 (2–7.8), p = 0.002; and at first followup: 8.5 (3.5–12) vs 4 (2–6), p = 0.020. These results indicate that high disease activity, measured with mRSS hand in early disease, as well as ARA, ATA, and vascular lesions in early disease may be risk factors for impaired mobility in advanced disease.
DISCUSSION
We demonstrated here that in the early stage of the disease, mHAMIS had clear correlations with measurements that assess the fibrotic evolution and the fibrotic activity in the skin. The finding indicates that the mHAMIS fulfills the criteria of the OMERACT filter18 regarding truth, and we therefore suggest that mHAMIS can be valuable in assessing the outcome of therapy directed toward reducing fibrotic skin manifestations in the early stage of SSc. However, even if mHAMIS changed in the early stage of the disease and was higher in patients with dcSSc, that would not be enough to fulfill the OMERACT criteria of discrimination and sensitivity to change. To ensure this fulfillment, mHAMIS have to be used in prospective interventional studies.
However, in contrast to mRSS hand, the mHAMIS did not improve significantly in a longterm perspective in the whole study group. Even if mHAMIS changed ≥ 3 units in more than 40% of the patients during followup, the change was not uniform. Just as many worsened as improved. This is in contrast to mRSS hand, where 40% changed, all improvement. This may happen because thin but tight skin may score a low mRSS but a high mHAMIS. In the later stages of the disease, skin atrophy dominates, which often means a skin tightly tethered to the underlying tissue3. That patients with higher mHAMIS at baseline (supramedian group) had a significant improvement at first followup but not at the second could mean that mHAMIS in later stages is likely measuring the damage caused by previous fibrotic activity. The mHAMIS could therefore serve as a feasible endpoint in routine followup and clinical trials. From a patient’s perspective, it would make more sense to assess the mobility of the fingers rather than to measure the perception of skin thickness, which may or may not affect this mobility.
Interestingly, there is also a relationship between skin involvement, hand mobility, and digital vascular lesions. In our study we found that patients with vascular lesions at baseline had higher mRSS compared to those without lesions. Patients with vascular lesions also had more limited hand mobility at followup. This is in line with studies by Mouthon, et al19 and Ennis, et al20 showing that a high mRSS value was a risk factor for digital ulcers and that ulcers influence hand mobility and performance of daily activities. It is also worth noting that mHAMIS improved significantly during followup in patients with immunosuppressive treatment, but not in the group without treatment. Patients without treatment had a low mHAMIS in early disease, making it nearly impossible to improve. On the other hand, the mHAMIS did not get worse during followup, indicating mild disease in this group, in contrast to mRSS hand, which improved regardless of this treatment. Our study was not powered or designed to study this in detail, but there are likely several explanations. One possibility is that the consequence of fibrosis is reduced and another is that articular involvement also influenced mobility and that this was reduced by the treatment. However, articular involvement was not recorded, which precludes drawing conclusions about the relationship between articular involvement and mHAMIS in our present study. But the relationship between hand mobility and articular involvement was demonstrated in an earlier study: Del Rosso, et al10 showed that patients with hand arthritis had higher HAMIS scores.
Our study is limited by the retrospective design based on data collected during routine clinical care. In addition, the percentage of dcSSc cases was low, although this reflects the composition of our cohort, especially considering that we study patients who survived the first years of disease. The prevalence of lcSSc in the Skåne region was 82% in December 201021. The result concerning clinically relevant change should be interpreted with some caution because the cutoffs for mHAMIS and mRSS hand were determined through clinical experience only and not through statistical analysis. The lack of information on articular involvement makes it impossible to assess what effect this could have on the mHAMIS. Nevertheless, there is strong evidence that the mHAMIS to a large extent measures the fibrotic skin changes and specifically the impaired function caused by fibrosis.
In the early stages, the mHAMIS reflects disease activity and can in later stages be regarded as a measure of disease-related damage arising from the fibrotic process and vascular involvement. The mHAMIS test measures the fibrotic skin changes of importance for the patients’ activities of daily life and is therefore suitable as an endpoint in followup examinations. However, to further investigate the responsiveness of mHAMIS, prospective interventional studies are needed.
Footnotes
Supported by grants from the Swedish Medical Research Council, the Medical Faculty of Lund University, the Swedish Rheumatism Association, Norrbacka-Eugenia Fund, King Gustaf V 80-year Fund, the Österlund Foundation, and the Kock Foundation.
- Accepted for publication March 31, 2016.








{kind=link}
{kind=link}
{kind=link}