
Abstract
Objective. Systemic sclerosis (SSc) leads to a high mortality from internal organ involvement. Scleroderma renal crisis (SRC) usually occurs in the diffuse cutaneous SSc (dcSSc) subset early in the disease, often with acute severe hypertension and renal failure. Prevalence of SRC since its classification in the early 1970s was determined in publications to assess whether the prevalence of SRC has changed over time because the proportion with the dcSSc subset is smaller in contemporary cohorts.
Methods. A review of the literature was conducted up to May 2015 using the PubMed, EMBASE, CINAHL, and Cochrane Library databases. Articles were included if they mentioned the prevalence of SRC and were cohort or cross-sectional studies with 50 or more patients with SSc. Articles were excluded if they were not in English or were a case series of SRC or case-control studies.
Results. Of the 5317 citations identified, 22 qualified. Years of publication were from 1983 to 2011, and cohort size varied from 68 to 8554 patients with SSc totaling 21,908 patients (9248 with dcSSc, 42%). There was no statistical reduction in the temporal prevalence of SRC noticed in the overall patients (4%), patients with dcSSc (7%–9%), or patients with limited cutaneous SSc (lcSSc; 0.5%–0.6%) based on either the start date of the cohort or publication date.
Conclusion. It appears that SRC remains uncommon in lcSSc and the rate in the dcSSc group may be stable over time. However, increasing awareness of SRC could lead to higher rates in more recent years and/or better survival from SRC, but this was not observed.
- SYSTEMIC SCLEROSIS
- SCLERODERMA
- RENAL CRISIS
- TEMPORAL TREND
- METAANALYSIS
Systemic sclerosis (SSc) is an autoimmune connective tissue disease with increased mortality from involvement of various internal organs1. The disease can be categorized into diffuse cutaneous (dcSSc) and limited cutaneous (lcSSc) subsets based on skin involvement. Severe organ complications, including scleroderma renal crisis (SRC), are more common in the dcSSc subset2.
SRC is defined in patients with SSc by acute severe hypertension (> 150/85 mmHg), acute renal failure (≥ 30% reduction in estimated glomerular filtration rate), microangiopathic hemolytic anemia, and an elevated creatinine3. Not all of these symptoms need be present to diagnose SRC. SRC is treated with angiotensin-converting enzyme (ACE) inhibitors with improved survival4. With decreasing SRC mortality5, we wondered whether the rate of SRC was also decreasing because of less severe dcSSc over the last quarter century (possibly because of the inclusion of more mild cases in cohorts from detection bias, proportionately less dcSSc in contemporary cohorts, or evolution of SSc disease over time). However, recognition of SRC may be increased because of the years of literature about this severe complication, which could actually increase its reported frequency. The survival with SRC has improved and this could increase the prevalence over time because patients would previously have died from SRC and would not be included in a cross-sectional study of patients with longstanding SSc. Our study aimed to determine whether the frequency of SRC in the published literature had changed over time.
MATERIALS AND METHODS
Study selection
A comprehensive literature review was performed on the PubMed, EMBASE, CINAHL, and Cochrane Library databases. Search dates were from the earliest studies in each database (1950 or later) until May 4, 2015. We included English-language, full-text articles for the prevalence of SRC in cohorts of SSc where the publications were cross-sectional or cohort studies and contained at least 50 patients. The prevalence or frequency of SRC had to be reported. We extracted data for the frequency of SSc overall and in subsets (dcSSc and lcSSc). The following were used as search terms: scleroderma: scleroderma, systemic sclerosis, dermatosclerosis, and skin sclerosis with: renal crisis: acute kidney injury, acute renal injury, acute renal insufficiency, acute kidney insufficiency, acute kidney failure, acute renal failure, scleroderma renal crisis, scleroderma kidney crisis, glomerulosclerosis, glomerulonephritis, and hypertension: hypertension, and high blood pressure.
Identified titles/abstracts were reviewed and full reports were obtained if appropriate. Studies were considered if they provided data on the prevalence of SRC, were not duplicates, and were not case-control studies where the rate of SRC could not be determined. Case reports were excluded. Additional articles were retrieved by hand searching relevant references.
Data collection
One reviewer (MT) extracted data from the studies and the other reviewer (JP) reviewed all abstracts for consensus. A standard data extraction form was used to record the following information: year of publication, author, location of study, study design, patient population, year of cohort inception or study onset, sample size, and proportion with SRC overall and within SSc subsets.
Quality assessment
Each study was assessed by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist6,7. STROBE is a 22-item checklist with items pertaining to the title and abstract of the article (item 1), background and objectives (items 2 and 3), methods (items 4–12), results (items 13–17), discussion (items 18–21), and funding (item 22). The purpose of the STROBE is not to give a quality score, but to ensure clear presentation of reporting.
Statistical analysis
Proportions were pooled with a random-effects model8. Forest plots were created to estimate prevalence of SRC in the study overall and dcSSc and lcSSc subsets where available with a 95% CCI. The I2 statistic was used to quantify the magnitude of heterogeneity (mild 0–30%, moderate 31–50%, high > 50%). Tau-squared was the square root of the between-study variance, and the p value was for Cochrane Q measure of heterogeneity. Metaregression through random-effects model was also used to analyze the study level associations between the prevalence of SRC and the year of publication, and separately the year of cohort inclusion/study onset in each publication (where provided). A p value < 0.05 was considered statistically significant. Metaregression was used to determine the study level associations between the rates of disease and publication year. Random-effects models were used, reporting the proportion of heterogeneity accounted for in the outcome by the year of publication. A bubble plot was used: a scatter plot of the disease rate on the Y-axis and the publication year (or study onset) on the X-axis. The size of the circle is inversely proportional to the variance of the estimated treatment effect. Publication bias was determined using funnel plots.
RESULTS
Search results
The literature search identified 5317 citations with 180 duplicates. Titles or abstracts (if available) were screened for eligibility, yielding 52 citations for full text review. Three studies were editorials or reviews and were excluded, 8 studies did not report on the prevalence of SRC, and 13 studies examined only those with SRC and not an entire cohort. A total of 5295 publications were excluded, with 22 remaining studies used for our metaanalysis (Supplementary Figure 1, available online at jrheum.org).
Description of the included studies and participants
There were 22 studies reporting on the prevalence of SRC in SSc including 9 for overall prevalence, 13 for frequency within dcSSc, and 10 in lcSSc. There were 21,908 patients with SSc enrolled.
Across all studies, the median number of items fulfilled on the STROBE checklist was 25.5, with a range from 22 to 31 with no noticeably improved reporting in more recent studies. Characteristics of the included studies are shown in Table 1A and Table 1B1,9–18,19–28,29.
Characteristics of the 22 studies included in the metaanalysis: 13 studies that identified prevalence* of SRC within SSc subsets.
Characteristics of the 22 studies included in the metaanalysis: 9 studies reporting the prevalence of SRC in SSc overall.
There was an outlier study where the rate of SRC was much higher than other studies published, from an SSc site that specialized in SRC, so referral bias was possible20. Analyses were performed with and without inclusion of the study to determine whether heterogeneity declined when the study was removed.
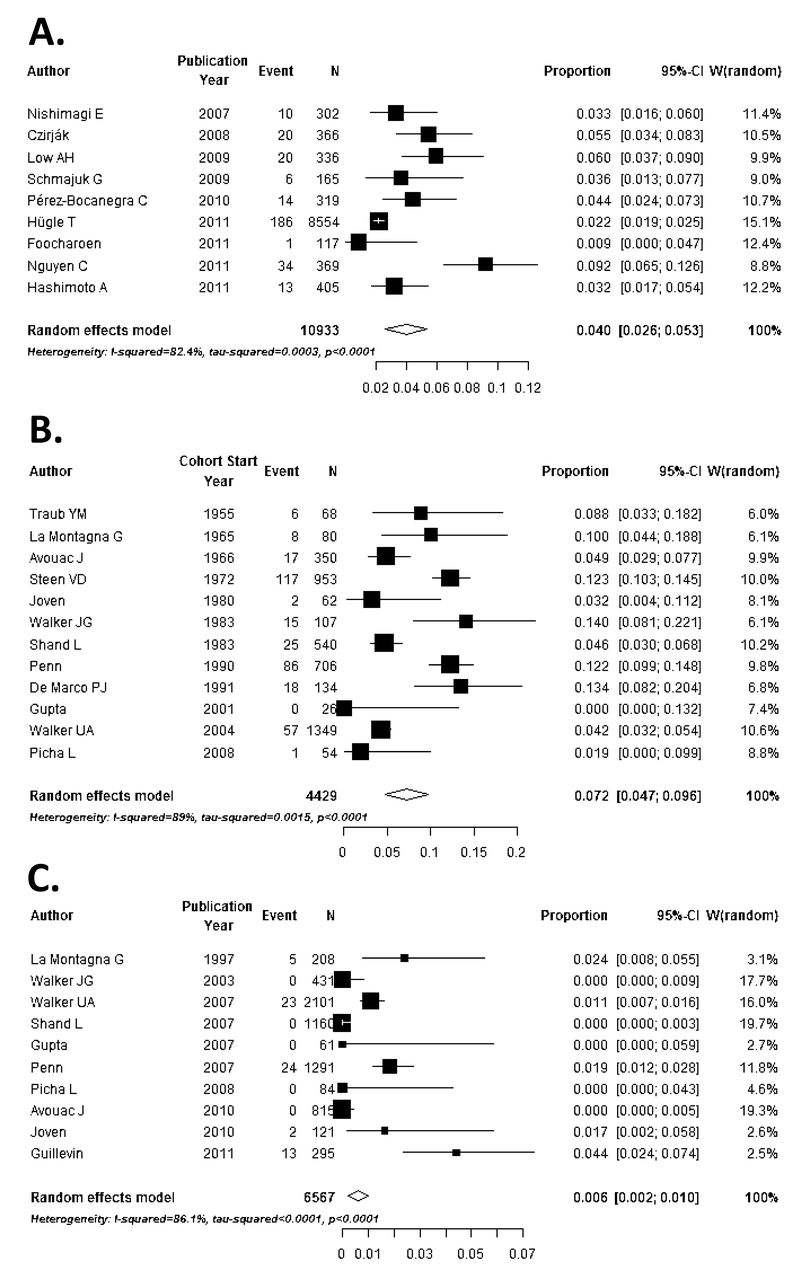
The prevalence of SRC was 4% in the overall SSc population, and 7% to 9% in the dcSSc subset (the smaller number was calculated when removing the outlier study that had the highest SRC rate, where the authors reported that they were a referral center for SRC, so the rate was expected to be high20). The lcSSc subset had a frequency of 0.5% to 0.6% with SRC. Our metaanalyses had large heterogeneity even when removing the outlier study for the prevalence of SRC overall and in the subsets. Forest plots with 95% CI for the prevalence of SRC are shown in Figure 1 (for the overall cohorts and within the dcSSc and lcSSc subsets).

The frequency of SRC over time in patients with (A) SSc overall, (B) dcSSc, and (C) lcSSc. Results are given with forest plots and 95% CI. SRC: scleroderma renal crisis; SSc: systemic sclerosis; dcSSc: diffuse cutaneous SSc; lcSSc: limited cutaneous SSc.
There were no significant differences in the rate of SRC over time by year of cohort onset or year of publication. However, the frequency of SRC in patients with dcSSc showed a nonsignificant reduction over time when analyzing the data by year of cohort entry (p = 0.16; Figure 2). Funnel plots showed that there may have been publication bias in the overall SSc population, but not in the dcSSc subgroup (Supplementary Figure 2 and Supplementary Figure 3, available online at jrheum.org).

{kind=link}
{kind=link}
Metaregression for associations between the rates of SRC in dcSSc and publication year. The frequency of SRC in dcSSc is decreasing over time, but not significantly (p = 0.16). SRC: scleroderma renal crisis; dcSSc: diffuse cutaneous systemic sclerosis.
DISCUSSION
Our study systematically evaluated the prevalence of SRC over time in SSc and in the subsets of dcSSc and lcSSc. While more recent SSc cohorts may be composed of more patients with lcSSc than dcSSc, within SSc cohorts overall, SRC prevalence seemed to be fairly constant. There was no statistical change in the prevalence of SRC temporally. Those at risk for SRC are especially men versus women, dcSSc versus lcSSc, early versus late SSc, and those with positive RNA polymerase 3 antibodies, high skin scores, rapidly progressive changes (interstitial lung disease, pericardial effusions, presence of tendon friction rubs), and use of steroids30. ACE inhibitors have reduced mortality, likely from rapid blood pressure control, where renin is reduced and expression of bradykinin, which seems to be unique to ACE inhibitors and not angiotensin II receptor antagonists, is increased. The blood pressure should be lowered to a normal value as quickly as possible, so other antihypertensives should be rapidly added to an ACE inhibitor if necessary.
Our study has limitations. There was no uniform definition for SRC, so we used the authors’ definitions. Non-English studies are excluded. However, it is reassuring that our funnel plots did not have obvious asymmetries to suggest publication bias. We studied “ever prevalence,” which is considered frequency in the studies. We did not determine incidence, which would be better calculated with a large claims database, not with the methodology of our study. Prevalence of SRC was given in studies with variable disease duration and length of followup. However, SRC occurs primarily in early dcSSc, so the length of followup of studies with disease duration of at least a few years compared with decades would not likely yield a different prevalence of SRC, other than that some patients may have died prior to inclusion in a prevalent cohort. The publications in general were from SSc centers. Other inclusion criteria were not described in detail (such as the referral area of the patients with SSc) or compared between studies, so the generalizability of the findings is unknown.
Because cohorts were assembled over various periods of time, we could examine only the year of publication or years the cohort spanned, and not the exact year of each individual event of SRC within the cohorts. In addition, SRC may occur more frequently in different demographics (SSc subsets, tertiary care setting, race, ethnicity, use of steroids, presence of RNA polymerase 3 antibodies), so results may have confounding that would result in variable prevalence of SRC among studies. The highest rates of SRC were reported in the United States, Australia, and the United Kingdom; these countries may also have higher rates of RNA polymerase 3 antibodies31. Last, there could be fewer recent publications about SRC because it is a known complication of SSc. This could bias recent estimates of the rate of SRC (either up or down). There could be a bias in which improved survival would inflate the frequency of patients with longstanding SSc having SRC ever. Previous mortality before ACE inhibitors was about 80%, and now it is 10% to 20%32. We did not report the incidence of SRC because the studies did not provide individual patient data of when SRC occurred each year. A better design for the incidence of SRC would be hospital codes for SRC over a defined period or administrative claims data because most people with SRC are hospitalized.
SRC may have a stable frequency over time. Patients with dcSSc are still at higher risk for developing SRC. Awareness of SRC is important because it is a potentially lethal complication if unrecognized.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
We thank Dr. Heather Thiessen Philbrook for her knowledge and assistance with statistical analyses and for making the forest plots.
- Accepted for publication March 3, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.