
Abstract
Objective. We examined the clinical significance of autoantibodies to the erythropoietin receptor (EPOR) in patients with systemic lupus erythematosus (SLE) who had biopsy-proven lupus nephritis (LN).
Methods. Forty-six Japanese patients with SLE with LN who had undergone renal biopsy during 1993–2014 were enrolled in this study and followed for a mean of 83 months. Sera from those patients were screened for anti-EPOR antibodies using ELISA.
Results. Anti-EPOR antibodies were detected in 18 (39%) of the 46 patients with SLE with anemia. Anti-EPOR antibodies were associated with low hemoglobin concentrations and reticulocytopenia. In addition, anti-EPOR antibodies were positively correlated with SLE disease activity, even though serum levels of the complement factors 3 and 4 did not differ between the 2 groups. In patients with International Society of Nephrology/Renal Pathology Society 2003 class IV LN, anti-EPOR antibodies were associated with active lesions including cellular crescents in glomeruli. Decrease in renal function was more frequently observed in patients without complete or partial renal response than in patients with it, and serum levels of the antibodies as well as renal response to treatment were significant risk factors for progression of renal dysfunction.
Conclusion. The present study suggests that anti-EPOR antibodies might be involved in overall disease activity and active renal lesions, as well as in the impaired erythropoiesis in patients with SLE with LN. Further, the levels of anti-EPOR antibodies may be an additional predictor for renal injury.
- LUPUS NEPHRITIS
- PROGNOSIS
- ERYTHROPOIETIN RECEPTOR
- AUTOANTIBODY
- ANEMIA
Systemic lupus erythematosus (SLE) is a chronic inflammatory disease of unknown etiology that can affect multiple organ systems. Immunological abnormalities with the characteristic production of a number of autoantibodies to nuclear antigens as well as to membrane molecules are hallmarks of the disease.
A number of hematologic abnormalities have been detected during the course of the disease1,2. Among these, anemia commonly occurs in about 50% of patients2. Several factors have been reported to contribute to the development of anemia, such as chronic diseases, loss of blood, nutritional deficiencies, immune-mediated diseases, myelofibrosis, uremia, certain medications, microangiopathic hemolysis, hypersplenism, infectious diseases, and myelodysplasia1,2.
With regard to the immunological mechanism of anemia in SLE, impaired erythropoietin (EPO) response attributable to autoantibodies to EPO has been reported since 19973. While relationships between the anemia profile and anti-EPO antibodies were investigated in some studies3,4,5,6, other studies have detected the involvement of autoantibodies and anti-EPO receptor (EPOR) antibodies in decreased response to EPO7.
EPOR is expressed not only in erythroblasts in bone marrow, but also in other organs including the kidneys, which can be commonly injured in the course of SLE. Previous in vitro and in vivo studies demonstrated that EPO may contribute to protecting the kidneys from injuries by binding to EPOR on renal resident cells, such as tubular epithelial cells, as well as through the correction of anemia8.
We evaluated the clinical significance of anti-EPOR antibodies in patients with SLE with biopsy-proven lupus nephritis (LN) on the basis of the aforementioned studies to show that anti-EPOR antibodies are associated with overall disease activity and active kidney lesions, and that they are inversely related to preserved kidney functions.
MATERIALS AND METHODS
Patients
Forty-six patients with SLE who had been diagnosed and followed at the Kanazawa University Hospital between 1993 and 2014 were included in our retrospective study. The diagnosis of SLE was based on the American College of Rheumatology (ACR) criteria9. A diagnosis of LN was confirmed by histological characteristics using renal biopsy specimens including light microscopy, electron microscopy, and immunofluorescence examination. Renal biopsy was performed for precise diagnosis of renal lesions with the consent of each patient. Antiphospholipid antibody syndrome (APS) was diagnosed according to the revised Sapporo criteria10. All blood samples were obtained after the patients had given their written informed consent at the admission for renal biopsy. The study protocol was approved by the medical ethics committee of Kanazawa University.
Clinical features and routine laboratory tests of patients with SLE
Demographic and clinical features were evaluated for each patient with SLE at the time of renal biopsy. Baseline clinical and laboratory findings were extracted from medical records; individual items included in the ACR criteria were also considered9, as well as the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)11 and the British Isles Lupus Assessment Group (BILAG) index12. To obtain a global score of the BILAG index, its component scores were assigned numerical values: A = 9, B = 3, C = 1, D = 0, and E = 0, resulting in a potential summed range of 0–72 points13. Other immunological and kidney-related variables were also identified, including anti-dsDNA, complement factors (C3, C4, CH50), antiphospholipid antibodies, lupus anticoagulants, 24-h urinary protein excretion, and serum creatinine. Anti-dsDNA antibodies were measured by a commercial quantitative ELISA (MESACUP DNA-II test [ds], MBL). Estimated glomerular filtration rate (eGFR) for Japanese patients was calculated using the following equation:

In addition, response to treatment including corticosteroid and immunosuppressive agents was evaluated based on the following definitions15: complete renal response with urine protein:creatinine ratio < 0.5 g/d and normal or near-normal eGFR, and partial renal response with ≥ 50% reduction in proteinuria to subnephrotic levels and normal or near-normal eGFR.
Detection of autoantibodies to EPOR
Anti-EPOR antibodies were detected by ELISA as previously described7. Briefly, polyvinyl 96-well microtitration plates (Nunc International) were coated with recombinant human EPOR (R & D Systems) at 5 μg/ml diluted in 0.2 M NaHCO3 buffer at 4°C for 24 h. The remaining free-binding sites were blocked with 1% bovine serum albumin (BSA) in phosphate buffered saline (PBS) at 4°C. After we washed the plates with Tween 20 Tris-buffered saline, samples were added in duplicate at 1:1000 dilution to 1% BSA in PBS for 20 h at 4°C. The plates were washed 4 times with the same buffer and incubated with goat anti-human Ig-conjugated with horseradish peroxidase (Millipore) at 1:5000 dilution for 1.5 h at room temperature. The substrate tetramethylbenzidine (KPL Inc.) was added and the reaction was stopped by the addition of 2 N sulphuric acid. Optical density was determined at 450 nm using an automatic plate reader and the antibody unit was calculated by a standard curve. The antibody was considered positive when the unit was ≥ 2.0.
Histopathologic studies
Renal biopsy specimens were prepared for light microscopic examination as previously described16. In brief, patients’ samples were fixed in 10% phosphate-buffered formalin (pH 7.4), embedded in paraffin, and sliced into 4 µm sections. These specimens were stained with H, periodic acid Schiff reagent, Mallory-azan, and periodic acid silver methenamine, and were examined under a light microscope, following the criteria of the International Society of Nephrology/Renal Pathology Society (ISN/RPS) 2003 classification17. The frequency of active and chronic lesions was determined, and activity index and chronicity index of histologic appearance were also calculated according to the National Institute of Health scores by Austin, et al18. Renal tissue specimens were examined by 2 pathologists.
Immunohistochemistry
After being deparaffinized and rehydrated, renal specimens were microwaved in 10 mM sodium citrate for antigen retrieval. After they were blocked with a Protein Block Serum-Free (Dako Co.), the sections were incubated with diluted anti-EPOR antibodies (sc-5624; Santa Cruz Biotechnology) overnight at 4°C. A peroxidase-labeled polymer conjugated to goat anti-rabbit IgG (EnVision System; Dako Co.) was then applied for 1 h. Finally, the sections were incubated in diaminobenzidine, and hematoxylin was used for counterstaining.
Statistical analysis
All comparisons between the 2 patient groups were performed using the chi-square test and the Mann-Whitney U test. ANOVA and regression analysis were used to correlate units of anti-EPOR antibodies measured using ELISA with SLEDAI and BILAG index scores and other clinical indices. The renal outcome curve was obtained using the Kaplan-Meier method and compared using the log-rank test. A multivariate Cox proportional hazards regression model was used to select factors that significantly affected the incidence of renal outcome and to estimate risk. All analyses were carried out with the statistical package SPSS, version 22 (SPSS). P values < 0.05 were considered statistically significant.
RESULTS
Characteristics of enrolled patients
The baseline characteristics of the 46 patients are shown in Table 1. Patients’ median age was 37 (14–70) years, and 41 (89.1%) of the patients were women. The median hemoglobin (Hb) concentration and reticulocyte count were 10.6 g/dl and 4.5 × 104/µl, respectively. The main causes of anemia were anemia of chronic disease (n = 28) and iron deficiency anemia (n = 8). Immunological assessment revealed that antibodies against dsDNA were present at median levels of 22 IU/ml. Fifteen patients (32.6%) were diagnosed with APS. Serum levels of C3 and C4 were decreased to median levels of 56 mg/dl and 8 mg/dl, respectively. Kidney-related variables included a median urinary protein excretion of 0.50 g/day at the time of renal biopsy and a median serum creatinine concentration of 0.64 mg/dl. The median SLEDAI score for overall disease activity was 10.
Clinical characteristics of patients at time of renal biopsy. Values are median (range) or n (%) unless otherwise specified.
Clinical characteristics of patients with SLE with and without anti-EPOR antibodies
Patients’ serum samples were analyzed using ELISA. Anti-EPOR antibodies were detected in 18 of the 46 patients. Demographic and clinical findings as well as coexisting autoantibodies were compared between patients with and without anti-EPOR antibodies; selected findings are shown in Table 1. The Hb level and number of reticulocytes were significantly lower in patients with anti-EPOR antibodies than in patients without them. Hb levels were correlated with anti-EPOR antibody levels (Figure 1A). In addition, SLEDAI scores were higher in patients with anti-EPOR antibodies than in patients without them. Similarly, the BILAG index, another SLE disease activity scoring system, was higher in patients with anti-EPOR antibodies than in patients without it (19, 9–43 vs 9, 0–39, p < 0.01). No difference was found in the 2 groups for other variables, including serum levels of anti-dsDNA antibodies, complement levels, and renal function at time of renal biopsy.

Relationship between disease activity and unit of anti-EPOR antibodies. (A) Hb concentration, (B) Anti-dsDNA antibody levels, (C) SLEDAI, and (D) BILAG scores were plotted against the unit of anti-EPOR antibodies determined by ELISA. Anti-EPOR: anti-erythropoietin receptor; Hb: hemoglobin; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; BILAG: British Isles Lupus Assessment Group index.
Correlation of anti-EPOR antibody levels with SLE disease activity
We examined the relationship between serum levels of anti-EPOR antibodies and SLE disease activity. Serum levels of anti-EPOR antibodies correlated with anti-dsDNA antibody levels (p < 0.05), the SLEDAI (p < 0.01), and the BILAG index scores (p < 0.01; Figures 1B–D), while not statistically significant with C3 levels. These results suggest that serum levels of anti-EPOR antibodies were correlated with SLE disease activity in patients with LN.
Renal pathological characteristics of patients with SLE with anti-EPOR antibodies
Renal biopsy findings were evaluated among enrolled patients. The activity index in 18 patients with anti-EPOR antibodies was higher than that in 28 patients without (Figure 2A). In addition, among 12 patients who had been diagnosed with LN class IV on the basis of the ISN/RPS 2003 classification, anti-EPOR antibody levels were significantly higher in patients with cellular crescents than in those without in individual components of the activity index (Table 2). On the other hand, chronicity index in patients with anti-EPOR antibodies tended to be higher than in patients without the antibodies in overall patients, but not statistically significant (Figure 2B). Also, anti-EPOR antibody levels were not different between patients with or without each component of the chronicity index (data not shown).

Comparison of activity index and chronicity index scores between patients with and without anti-EPOR antibodies and localization of EPOR in diseased kidneys. (A) Activity index score and (B) chronicity index score. (C) Negative control of immunostaining for EPOR. (D) Positive expression of EPOR mainly on glomerular infiltrated cells. Original magnification 200×. EPOR: erythropoietin receptor.
Comparison of anti-EPOR antibody levels between 2 groups by the presence or absence of individual components of activity index in 12 patients with Class IV LN. Antibody levels are presented as the unit. Values are median (range).
Expression of EPOR in the diseased kidney
Based on the finding that anti-EPOR antibody levels correlated with cellular crescents in diseased glomeruli, possible localization of its binding site, EPOR, was examined. EPOR immunoreactivity was observed in the renal tissue, especially infiltrated cells in glomeruli (Figures 2C–D).
Outcome of renal function
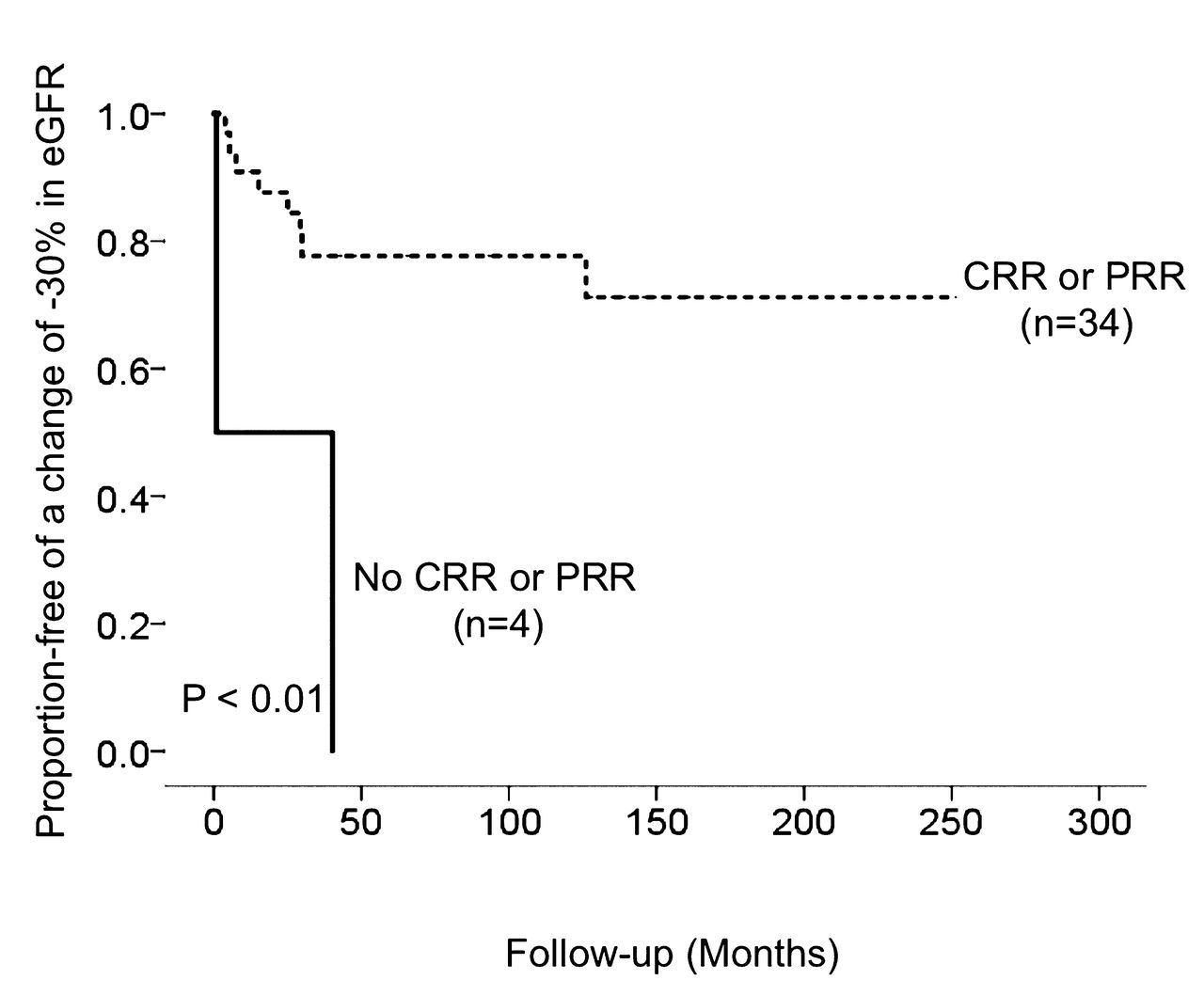
Followup data on immunosuppressive treatment were available for the course of renal function in 38 patients. The mean followup period was 83.2 ± 65.7 months between 1993 and 2014. The rate of changes of −30% in eGFR, an alternative endpoint for chronic kidney disease (CKD) progression19, was significantly smaller in patients with complete or partial renal response to immunosuppressive therapy than in patients without (Figure 3).

{kind=link}
{kind=link}
{kind=link}
The renal outcome of the retrospective analysis of 38 patients with LN with immunosuppressive treatment. Event-free rate of eGFR change of −30% stratified by renal response to treatment according to the Kaplan-Meier method. Dotted line means CRR or PRR (n = 34). Solid line means no CRR or PRR (n = 4). The mean followup period was 83.2 ± 65.7 months. Differences between groups were compared by a log-rank test. LN: lupus nephritis; eGFR: estimated glomerular filtration rate; CRR: complete renal response; PRR: partial renal response.
Clinical variables for the deterioration of renal function
The results of the multivariate Cox proportional hazards regression analysis are shown in Table 3. The unit of anti-EPOR antibodies as well as complete and partial renal response to immunosuppressive therapy was the independent risk factor for eGFR change of −30% (HR 1.44, 95% CI 1.12–1.87, p < 0.01).
Variables identified by multivariate Cox proportional hazards regression analysis associated with a change of −30% in eGFR. HR are adjusted for covariates including age, sex, unit of anti-EPOR antibodies, and no CRR or PRR.
DISCUSSION
Our present retrospective study demonstrated that serum levels of anti-EPOR antibodies were associated with disease activity in all patients and with active renal lesions in class IV LN as well as with anemia in SLE. In addition, renal function more rapidly declined in patients without renal response to treatment than in patients with the response, and anti-EPOR antibody levels were additional risk factors for the progression of renal dysfunction.
Our study showed that the presence of serum anti-EPOR antibodies was associated with reticulocytopenia and low Hb in anemic patients with LN. Autoantibodies to EPOR were detected in a part of 60 patients with SLE with or without LN and those with other CKD7. In addition, the antibodies were reported to bind to EPO and to inhibit the proliferation of erythroid progenitors in vitro7. Clinically, anti-EPOR antibodies had a negative correlation with the number of bone marrow erythroblasts in anemic patients with immune-mediated diseases7. The results of our study suggest that anti-EPOR antibodies might be involved in the development of anemia with reticulocytopenia, through interference with the action of EPO in the bone marrow in SLE.
We found a positive correlation between serum anti-EPOR antibodies and overall disease activity in patients with SLE with biopsy-proven LN. A similar relationship was noted in an earlier study that examined the correlation of anti-EPO antibodies with clinical manifestations of SLE3. Similarly, another study showed that patients with SLE with anti-EPO antibodies had a significantly higher disease activity score, as assessed by the European Consensus Lupus Activity Measure (ECLAM), than did patients without4. Additionally, the study showed ECLAM to be an independent predictor of having anti-EPO antibodies4. By contrast, other studies focusing on the relationship of anti-EPO antibodies or autoantibodies to the thrombopoietin receptor showed that levels of antibodies were not associated with disease activity in SLE5,20. Because disease activity indices contain components of nephritis11,12, it is necessary to interpret the association of these indices with anti-EPOR antibodies in consideration of selection bias. These studies collectively suggest that more research is needed to clarify whether anti-EPOR antibodies could qualify as indicators of disease activity in patients with SLE.
Anti-EPOR antibodies correlated with renal active pathological lesions, particularly cellular crescents in glomeruli, in patients with class IV LN. The most common renal injury seen in SLE is immune complex-mediated glomerular disease, and class IV is the most severe histological form of LN16,21. The pathogenesis of class IV LN is known to be primarily related to the in situ formation of immune deposits, such as the anti-DNA immune complex22,23. As a result, activation of complement proteins with the production of the chemoattractants (C3a and C5a) results in the recruitment of inflammatory cells, including neutrophils and mononuclear cells22,23. While expression of EPOR in diseased kidneys was identified by immunohistochemistry, we did not examine similar involvement and nephrotoxicities of the EPOR–anti-EPOR antibodies complex or antibodies themselves in kidneys. After reviewing the correlations with cellular crescents in glomeruli in our present study, we propose that more basic studies are needed to elucidate the interaction between EPOR on glomerular resident cells and/or infiltrating cells and anti-EPOR antibodies in the kidney.
In our study, renal function in patients with anti-EPOR antibodies declined earlier than in patients without the antibodies. Further, in multivariate analysis, serum levels of anti-EPOR antibodies were selected as a significant risk factor for decline of renal function. In addition to the effect of anemia on the kidney, basic studies have demonstrated that the EPOR is expressed by renal resident cells, including endothelial cells, mesangial cells, and podocytes24,25. Previous in vitro and in vivo studies demonstrated that EPO has renoprotective effects through not only suppression of inflammation, oxidative stress, and apoptosis, but also through maintenance of proteins such as nephrin in the cytoskeleton25,26. In addition, administration of EPO in patients with CKD has the potential to preserve renal function, as suggested by previous clinical trials and epidemiological studies27,28,29. The findings of these studies suggest that renal function may be exacerbated by the blockade of the EPO–EPOR interaction by antibodies and that measurement of anti-EPOR antibodies may predict renal prognosis. Overall, these studies suggest that further investigation is required to determine whether anti-EPOR antibodies can be used as a serologic marker for progression of renal injury in LN in combination with other known variables, including the elevated titers of anti-dsDNA and low complement levels.
We noted several limitations in our present study. First, our study was dependent on collectable medical records because of its retrospective design. Second, limiting study enrollment to only patients with renal biopsy likely created an influence of bias. These limitations may have placed significant constraints on the interpretation of the results, particularly those related to differences in renal outcome. However, clinical examination by longterm observation in patients with biopsy-proven LN is important for understanding the pathophysiology of LN and its clinical outcome.
Autoantibodies to the EPOR may be involved in disease progression and may be a useful serologic marker for monitoring disease activities in LN.
Footnotes
Supported by a grant from the Ministry of Education, Science, Sports and Culture, Japan.
- Accepted for publication March 11, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.