

Abstract
Objective. In daily practice, we noticed that hand osteoarthritis (OA) was commonly associated with primary Sjögren syndrome (pSS). Therefore, we aimed to investigate its prevalence in patients with pSS in a controlled study.
Methods. The study included patients with pSS and controls with systemic lupus erythematosus (SLE). Standard hand/wrist radiographs were obtained and classified according to the Kellgren-Lawrence system. “Erosive hand OA” was defined according to the Verbruggen-Veys classification.
Results. There were 114 patients with pSS (110 women, 51.0 yrs) and 34 patients with SLE (33 women, 42.4 yrs). Among 114 patients with pSS, 42.7% had radiographic, 30.3% symptomatic, and 16.0% erosive hand OA. The prevalences of radiographic (45.5%) and erosive hand OA (14.4%) in 90 patients with pSS with age- and sex-matched patients with SLE were significantly higher than those in patients with SLE (14.7% and 0.0%, p = 0.007 and p = 0.012, respectively). Interobserver reliabilities for diagnosing radiographic and erosive OA were found to be good (ĸ = 0.780 and ĸ = 0.788, respectively). Intraobserver reliabilities for diagnosing radiographic and erosive OA were also good (ĸ = 0.784 and ĸ = 0.825 for FO, and ĸ = 0.722 and ĸ = 0.800 for AB, respectively). The frequency of hand OA in patients with pSS was found to be increased with increasing age (r = 0.513). The mean age of those with erosive hand OA was significantly higher than those without erosive OA (p < 0.001).
Conclusion. This study suggests that pSS, conversely to SLE, is more frequently associated with hand OA.
The distribution of arthritis in primary Sjögren syndrome (pSS) is similar to that of systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA), primarily affecting the small joints of the hands. Unlike RA, erosive arthritis is rarely seen in pSS1. In daily practice, we noticed that hand osteoarthritis (OA), especially erosive hand OA, was commonly associated with pSS.
In the review of literature, we found no controlled study investigating the relationship between pSS and hand OA, although there are some published observations similar to ours2,3. The aim of our study was to investigate the prevalence of hand OA in patients with pSS.
MATERIALS AND METHODS
The patients with pSS followed up in a university hospital were called by telephone and invited to participate in our study. Patients with SLE were included as controls. We obtained a detailed medical history and performed a full physical examination in all patients who agreed to take part in our study.
All patients were asked whether they had pain/aching/stiffness on most days in any of their hand joints including the bilateral distal interphalangeal (DIP), proximal interphalangeal (PIP), metacarpophalangeal (MCP), thumb interphalangeal (IP), and thumb base joints.
The results of laboratory investigations were recorded, including rheumatoid factor (RF), anticyclic citrullinated peptide antibodies (anti-CCP), antinuclear antibody (ANA), anti-Ro/SSA and anti-La/SSB antibodies, and minor salivary gland biopsies previously performed.
Standard posteroanterior and oblique hand/wrist radiographs (both hands on the same film) were ordered in all patients. Each radiograph was read by both an experienced rheumatologist (FO) and a radiologist (AB) who were “blinded” to the patients’ identities. Forty-five of the 114 radiographs were read a second time by both of the investigators. When there was no agreement between the readers, they were re-read by the 2 investigators together and then final common opinion was obtained. All the radiographs were classified according to the Kellgren-Lawrence (KL) classification system4. At joint level, “radiographic hand OA” was defined as KL grade ≥ 2 and “symptomatic hand OA” as KL grade ≥ 2 plus pain/aching/stiffness5. Erosive OA was defined as the presence of eroded or remodeled phase in ≥ 1 IP or thumb base joints following the Verbruggen-Veys classification6,7,8. At subject level, participants with ≥ 1 affected joint(s) according to the definitions above were classified as cases5.
RESULTS
We included in our study 114 patients (110 women, mean age 51.0 yrs) with pSS who fulfilled the American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for pSS9.
Of the patients, 110 (96%) had arthralgia and 2 (1.8%) had arthritis in their hand joints including the bilateral DIP, PIP, MCP, thumb IP, and thumb base joints. Twenty percent of patients with pSS with joint pain had inflammatory arthralgia.
ANA was found to be positive in 75 of 114 patients with pSS (65.7%), RF in 33 of 101 patients (32.7%), and anti-CCP in 3 of 57 patients (5.3%). Anti-Ro/SSA and anti-La/SSB antibodies had been assessed in 88 patients with pSS. Anti-Ro/SSA was positive in 63 patients and anti-La/SSB was in 32. Minor salivary gland biopsy had been performed in 88 patients and 81 of them had revealed positive results (focus score ≥ 1; Table 1)10.
Demographic and clinical features of patients with pSS and controls. Values are n (%) unless otherwise specified.
In total, 34 patients (33 women, 1 man) who fulfilled the 1982 revised ACR criteria for SLE11 were enrolled as controls. Their mean age was 42.4 years. Of the patients with SLE, 33 (97%) had arthralgia and 20 patients (59%) had arthritis in their hand joints. There were no differences in the family history of hand OA, body mass index, and C-reactive protein (CRP) levels between the pSS (matched with age and sex with SLE) and SLE groups.
The hand/wrist radiographs were obtained in 114 patients with pSS and 34 patients with SLE. Among the 114 patients with pSS, 51 (42.7%) had radiographic hand OA, 36 (30.3%) had symptomatic hand OA, and 19 (16.0%) had erosive hand OA (Table 2). There were wrist joint erosions in 2 patients with pSS (1.7%). RF and anti-CCP antibodies were negative in these patients. They had also no erosive hand OA.
Prevalence of hand OA in patients with pSS and controls. Values are n (%) unless otherwise specified.
The prevalences of radiographic hand OA (45.5%) and erosive hand OA (14.4%) in 90 patients with pSS who were age- and sex-matched with patients with SLE were significantly higher than those in patients with SLE (14.7% and 0.0%, p = 0.007 and p = 0.012, respectively; Table 2).
Interobserver reliabilities for diagnosing radiographic and erosive OA were good (ĸ = 0.780 and ĸ = 0.788, respectively). Intraobserver reliabilities for diagnosing radiographic and erosive OA were also found to be good (ĸ = 0.784 and ĸ = 0.825 for FO, and ĸ = 0.722 and ĸ = 0.800 for AB, respectively).
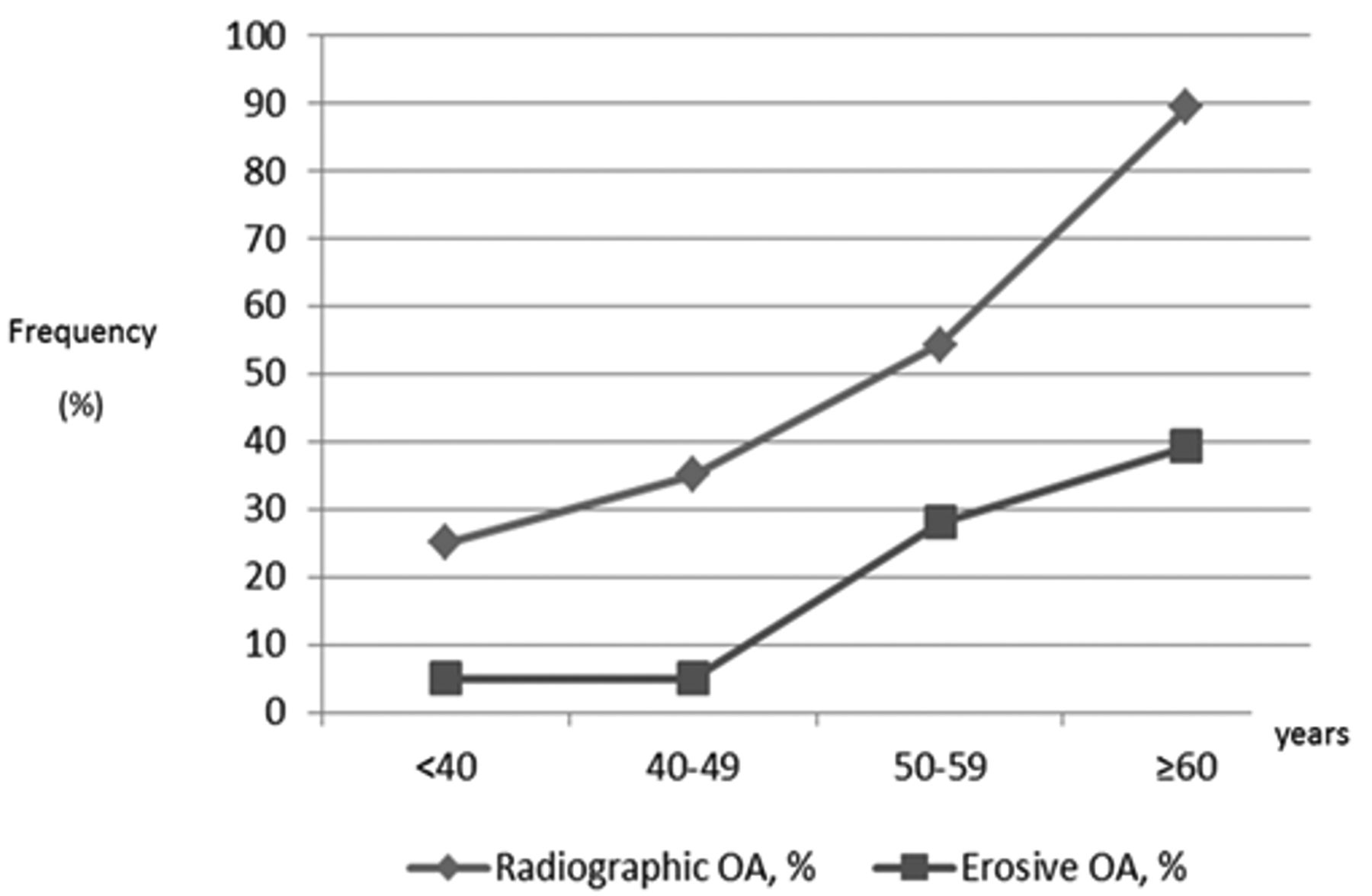
The frequency of hand OA in patients with pSS increased with increasing age (r = 0.513, p < 0.001; Figure 1). Patients with pSS with erosive hand OA had significantly higher mean age than those without erosive hand OA (p < 0.001). Cigarette smoking (p < 0.05) and ANA positivity (p < 0.001) were less common among the patients with erosive hand OA than those without erosive hand OA. There was no difference in the frequency of RF, anti-CCP, and anti-Ro/SSA and anti-La/SSB antibodies between these 2 groups. No relationship was observed between the presence of erosive hand OA and inflammation markers including erythrocyte sedimentation rate (ESR) and CRP.

The frequency of hand OA in patients with primary Sjögren syndrome by age group. OA: osteoarthritis.
DISCUSSION
Our study suggests that patients with pSS display more frequently hand OA than SLE. The prevalence estimates of hand OA in population surveys5,12,13,14,15,16 show great variation, which may be because of methodologic, genetic, and geographic differences across cohorts. The Framingham Osteoarthritis Study5 demonstrated that the age-standardized prevalence of radiographic hand OA was 44.2% in women and 37.7% in men, whereas the age-standardized prevalence of erosive and symptomatic OA was much higher in women (9.9% vs 3.3%, and 15.9% vs 8.2%). The prevalence of radiographic hand OA in patients with pSS was found to be similar in the Framingham Osteoarthritis Study, but the prevalence of erosive hand OA was much higher than in the general population in that study. A previous population study estimated the prevalence of 8.4% for symptomatic hand OA in Turkish women aged > 40 years17, which was significantly less than what we found in patients with pSS (30.3%). However, this result should be evaluated with caution because interpretation of hand symptoms in patients with pSS may be difficult. In our study, 22% of patients with symptomatic hand OA with pSS had inflammatory arthralgia, and this symptom may be attributable more to SS than to hand OA.
There are no controlled studies investigating the relationship between pSS and hand OA. In a previous report, 5 patients with SS with erosive hand arthropathy were described3. Although their early clinical and radiological findings were compatible with a diagnosis of erosive hand OA, hand involvements progressed to a different pattern between erosive hand OA and RA. Authors suggested that the diagnosis of psoriatic arthritis and also calcium pyrophosphate dihydrate arthritis were unlikely in their patients. Based on our report, our finding of increased frequency of erosive hand OA in the patients with pSS may suggest that these patients had a more severe form of hand OA. However, we did not find any association between the existence of soft tissue swelling and erosive hand OA in the patients with pSS. No patients with pSS with erosive hand OA had synovitis. There was also no correlation between the presence of erosive hand OA and clinical (morning stiffness ≥ 30 min) and laboratory (CRP and ESR) markers of inflammation.
In another report, a subset of patients presenting with xerostomia attributable to nonspecific sialadenitis, who also have generalized nodal OA, was described. This combination was called “SOX” syndrome: sialadenitis, OA, and xerostomia, a new disease entity. No patients met the ACR/EULAR criteria for pSS9. Authors also reported that 25% of subjects with nodal OA had clinical and laboratory features of SOX syndrome2.
There is some evidence that nodal hand OA may be an autoimmune disease18. Further, increased frequency of the HLA-A1B8 and MZ α1-antitrypsin phenotypes was observed (27% vs 11.5%, relative risk 2.79, and 12% vs 3.6%, relative risk 3.73, respectively) in patients with nodal hand OA. These associations were found to be related to the development of the disease rather than to severity19. Interestingly, an increased frequency of a combination of HLA-A1, B8, and DR3 was also demonstrated in patients with pSS20.
Our study suggests that patients with pSS display more frequently hand OA than patients with SLE. The main limitation of our study was that healthy controls could not be included for the comparison of hand OA prevalence. Moreover, our study was performed in the hospital-based sample and these patients might be different from a primary rheumatology care population. However, the finding of significantly higher frequency of erosive hand OA in patients with pSS than expected in the general population suggested that there was an association between erosive hand OA and pSS rather than a coincidence. Further studies investigating their pathogenesis may provide new information about this possible association.
- Accepted for publication February 19, 2016.








{kind=link}