

Abstract
Objective. To examine the associations between lowering low-density lipoprotein cholesterol (LDL-C) and cardiovascular (CV) outcomes among patients with rheumatoid arthritis (RA) and patients without it.
Methods. Adult patients with RA and 2 age- and sex-matched control cohorts [RA plus general controls (RA/GN), RA plus osteoarthritis (OA) controls (RA/OA)] were identified between January 1, 2007, and December 31, 2011. Patients with a diagnosis of hyperlipidemia who initiated statin therapy without prior CV events were included. Multivariable Cox proportional hazard analyses were used.
Results. The study identified 1522 patients with RA with 6511 general controls (RA/GN cohort); and 1746 patients with RA with 2554 OA controls (RA/OA cohort). During followup, mean (SD) LDL-C (mg/dl) was 96.8 (32.7) for RA, 100.1 (35.1) for general controls, and 99.1 (34.3) for OA. The relationship between lowering LDL-C and CV outcomes was similar for both RA and non-RA controls (p for interaction = 0.852 in RA/GN cohort, and p = 0.610 in RA/OA cohort). After adjusting for baseline CV risk factors, lowering LDL-C was associated with a 29%–50% lower risk of CV events (HR [95% CI] = 0.71 [0.57–0.89] in RA/GN, 0.50 [0.43–0.58] in RA/OA). Subgroup analyses showed that lowering LDL-C was associated with a similar degree of reduction of CV events in RA and non-RA controls (HR of 0.67–0.68 for RA, 0.72 for general controls, 0.76 for OA controls).
Conclusion. Lowering LDL-C levels was associated with reduced CV events. The relationship between lowering LDL-C and CV outcomes in RA was similar to the relationship found in matched general and OA controls.
Cardiovascular (CV) disease is a common comorbidity for patients with rheumatoid arthritis (RA). It is estimated that patients with RA have a 50% increased risk of CV events or early mortality relative to the general population1,2. A high systemic inflammatory burden3 as well as traditional risk factors such as hypertension (HTN), diabetes, and smoking appear to be key contributors to the increased CV events in RA4. High cholesterol is an important factor for the increased risk of CV events for the general population; however, growing evidence suggests a complex relationship between lipid levels and CV risk in patients with RA5,6,7. Epidemiological studies reported lower lipid levels in patients with RA compared to the general population6,8, but at the same time, patients with RA had higher rates of myocardial infarction (MI) and ischemic stroke6. These findings are potentially due to the altered lipid metabolism from systemic inflammation, drug therapy, and several genetic factors in RA9.
Because of this complex relationship between lipid levels and CV diseases in RA, there is a lack of clinical guidelines to identify patients at high risk for CV disease and to manage these groups. The European League Against Rheumatism10 currently recommends an annual CV risk assessment, treatment, and management according to guidelines that apply to the general population11. The hydroxymethylglutaryl CoA reductase inhibitor (statin) therapy has been shown to be beneficial in primary and secondary prevention of CV diseases in the general population12,13. However, evidence regarding the benefits of lowering elevated low-density lipoprotein cholesterol (LDL-C) in patients with RA is not clear. Although several studies suggest potential CV protective effects of statin therapy in RA, the results are from posthoc analyses14,15, and a recent prospective randomized controlled trial was terminated early owing to low CV event rates16. Specifically, differences in CV disease associated with lowering lipid levels between patients with RA and without need to be further investigated.
Given these uncertainties, the purpose of our study was to evaluate the association between lowering LDL-C levels and CV outcomes among RA subjects and age- and sex-matched controls who are prescribed statin therapy in a US managed care setting. Understanding differences in benefits of lowering LDL-C levels for patients with RA will be helpful to better manage these patients.
MATERIALS AND METHODS
Data source
A retrospective cohort study of patients enrolled in Kaiser Permanente Southern California (KPSC) was conducted using information from the KPSC electronic medical records (EMR) and administrative databases between January 1, 2006, and December 31, 2011. KPSC is a nonprofit, integrated health insurance provider with a current membership of over 4 million in Southern California. KPSC also provides comprehensive medical services through its own facilities, which include hospitals, outpatient sites, and a centralized laboratory. All aspects of care and interaction with the healthcare delivery system are included.
Study cohort
Adult patients aged ≥ 18 years were required to have 2 or more diagnoses of RA [International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code, 714.xx] from January 1, 2007, to December 31, 2011 (identification period), to be eligible for the RA cohort. Patients were also required to have at least 1 prescription for a disease-modifying antirheumatic drug (DMARD) within 12 months (before or after) the RA diagnosis17. The first RA diagnosis date or DMARD prescription date was defined as an index date. Continuous membership with drug benefit for 12 months prior to the index date (baseline period) was required to be included in the RA cohort.
Two RA cohorts were identified. The first was matched to the general KPSC population (general controls) in a ratio of 4:1. The second RA cohort was matched to individuals with a diagnosis of osteoarthritis (OA; ICD-9-CM of 715.xx; OA controls) in a ratio of 1:1. OA is a chronic condition that brings patients into regular contact with the healthcare system similar to RA. Matching of both RA cohorts to general and OA controls was based on sex and birth year (within a window of ± 2 yrs). Matched controls were required to have at least 1 outpatient or inpatient encounter so that an index date could be assigned during the matching process. They could not have an RA diagnosis or be receiving any DMARD therapy during the study period. Matched controls were also required to have continuous KPSC membership plus drug benefit for 12 months prior to the index date as well as continuous membership plus drug benefits until the matched reference individual completed the qualification criteria. Unmatched patients with RA were dropped from the RA cohort (n = 1243 for RA matched to general controls; n = 165 for RA matched to OA controls).
Patients with a hyperlipidemia diagnosis (ICD-9-CM of 272.0, 272.1, 272.2, 272.4, 272.5, 272.8, or 272.9) and ≥ 1 statin prescription (Generic Product Identifier Class Codes of 3940, 3999) in the baseline period were included in the study. We excluded patients with a history of CV disease [MI, old MI, revascularization process, angina, stroke, transient ischemic attack (TIA), intermittent claudication, heart failure, abdominal aortic aneurysm, acute carotid procedures] during the baseline period because the focus of our study was a primary prevention population. Patients without an LDL-C laboratory result during the followup period were excluded from the analyses. Patients were followed from their index date until the first CV outcome, end of enrollment in the health plan, death from other causes, or the end of the study (December 31, 2011), whichever occurred first.
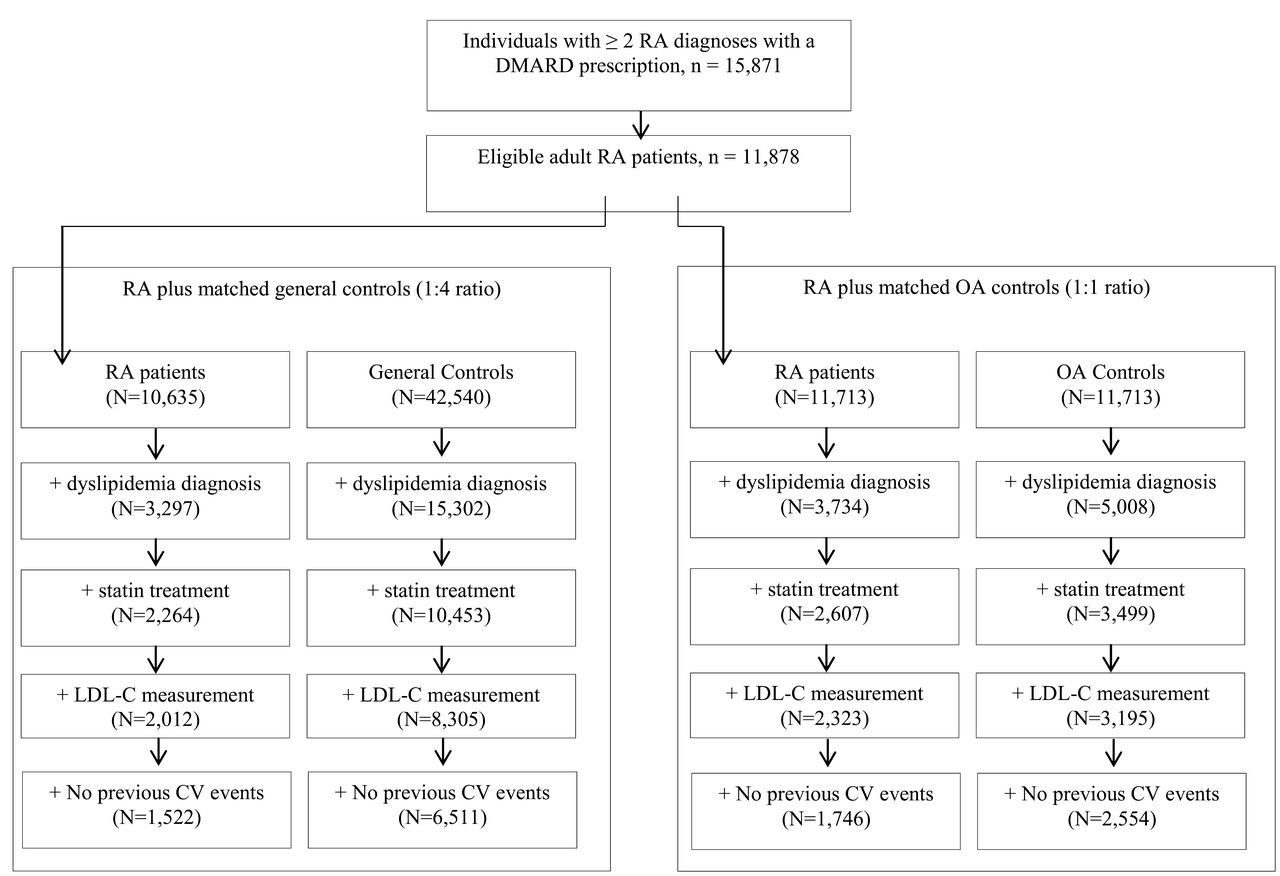
Through the matching procedure, we were successful in matching 10,635 patients with RA to 42,540 general controls (1:4 match) and 11,713 patients with RA to 11,713 OA controls (1:1 match). After restricting the population to those with a hyperlipidemia diagnosis plus ≥ 1 statin prescription during the baseline period, no previous CV events and ≥ 1 LDL-C measurements during the followup period, our sample was reduced to 1522 patients with RA matched with 6511 general controls, and 1746 patients with RA matched with 2554 OA controls (Figure 1). Median followup periods for the final study samples were 3.1 years for RA plus general controls and 4.0 years for RA plus OA controls. The study protocol was approved by the KPSC Institutional Review Board (#6331).

Flowchart of study subjects. RA: rheumatoid arthritis; DMARD: disease-modifying antirheumatic drugs; LDL-C: low-density lipoprotein cholesterol; CV: cardiovascular; OA: osteoarthritis.
Lowering LDL-C levels
LDL-C during followup was categorized as whether the LDL-C was lowered to the recommended levels by the National Cholesterol Education Program Expert Panel — Adult Treatment Panel III guidelines18. Though this guideline was updated in 201319, it was the standard of care during the time period for our study. The LDL-C recommended levels were < 100 mg/dl (2.6 mmol/l) for individuals at high risk, < 130 mg/dl (3.4 mmol/l) for those with moderate CV risk, and < 160 mg/dl (4.1 mmol/l) for those in the lowest CV risk category. The risk category was assigned to each individual based on coronary heart disease (CHD) status or a 10-year risk for CHD using baseline information18. Multiple LDL-C measurements during the followup period were observed and the analyses were conducted using the closest LDL-C value to the CV event or end of followup.
Other variables
Baseline patient characteristics including demographics (age, race/ethnicity, sex), body mass index, smoking status, comorbidities (Charlson comorbidity index, HTN and anti-HTN medication use, and diabetes) and baseline CV risk were obtained from the EMR. Among these variables, age, sex, HTN, anti-HTN medication use, smoking status, and diabetes were used as covariates to investigate the relationship between LDL-C and CV events, consistent with Framingham risk prediction20.
Study outcomes
The study outcomes of interest included MI, angina, stroke, TIA, intermittent claudication, heart failure, or death from CV disease20. Primary hospital discharge records were used to define MI, angina, and stroke. The ICD-9-CM codes for each outcome are listed in Appendix 1. Outpatient and/or emergency department visit records were further used to define TIA, intermittent claudication, and heart failure. Any death occurring within 1 month after a defined CV event was classified as death from CV disease. Death was identified from health plan databases, Social Security Administration vital status files, and California state death files.
Statistical analyses
Baseline demographic information was summarized using descriptive statistics. Comparisons between RA and matched controls were conducted using t tests or Wilcoxon-Mann-Whitney tests for continuous variables, and chi-square tests for categorical variables. To investigate the association between LDL-C and CV outcomes, univariable and multivariable Cox proportional hazard analyses were conducted. HR and 95% CI were reported. Interaction terms between having RA and LDL-C levels were investigated to examine the differences in LDL-C and CV outcomes across RA and matched controls. Subgroup analyses were conducted for RA and non-RA controls separately.
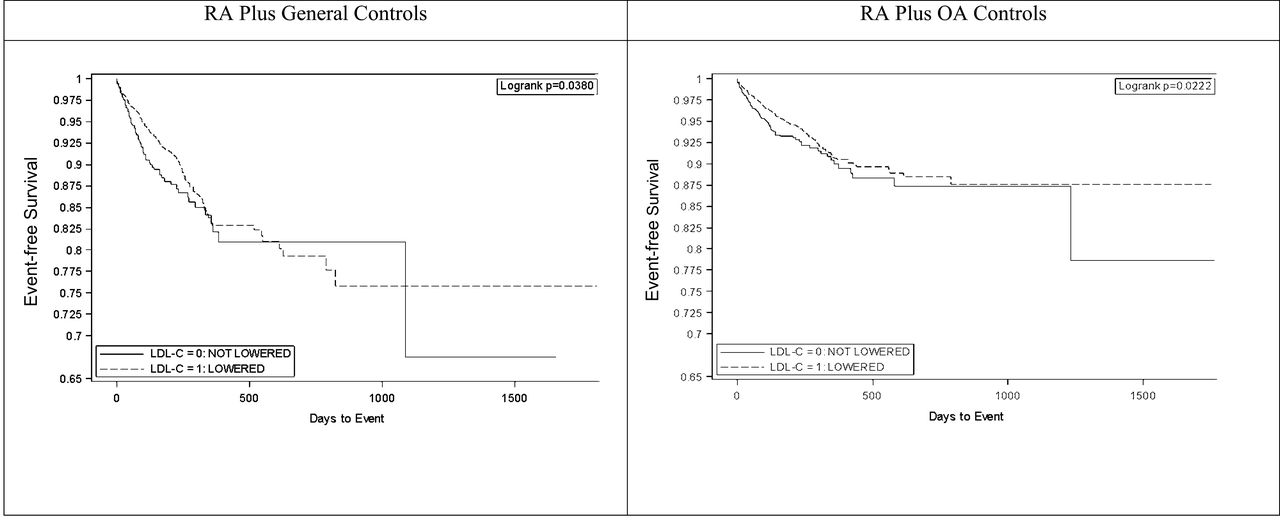
Kaplan-Meier survival curves with log-rank tests were used to demonstrate the event-free survival over time for the group that lowered LDL-C to the recommended levels compared with the group that did not (Figure 2). Sensitivity analyses were conducted using different LDL-C results (average LDL-C during followup, median LDL-C during followup) or different followup periods (starting to followup from the last LDL-C). Statistical analysis was performed with SAS version 9.2 (SAS Institute Inc.).

Kaplan-Meier survival curves show the event-free survival over time for the group that lowered LDL-C to the recommended levels compared with the group that did not. RA: rheumatoid arthritis; LDL-C: low-density lipoprotein cholesterol; OA: osteoarthritis.
RESULTS
The baseline demographic information for the 2 cohorts is presented in Table 1. Overall, traditional CV risk factors were higher in patients with RA compared with general and OA controls. In the RA cohort matched to general controls, 74.2% had HTN, 40.9% had diabetes, 33.9% were obese, and 10.4% were smokers. These were all higher than the proportions found in the matched controls. Similarly, higher proportions of CV risk factors were found in RA cohort matched to OA controls except for obesity, which was higher in OA controls. Patients with RA had higher CV risk at baseline compared to general controls (high risk: 41.3% vs 38.1%) and compared to OA controls (high risk: 40.3% vs 36.2%).
Baseline characteristics. Data are n (%) unless otherwise indicated.
Identified statin therapy included atorvastatin 10–80 mg, simvastatin 5–80 mg, fluvastatin 20–80 mg, lovastatin 10–40 mg, rosuvastatin 5–40 mg, and pravastatin 10–80 mg. Lower baseline lipid levels were observed in RA cohorts compared to general [mean LDL-C for RA vs general controls: 104.6 vs 109.6 in mg/dl; 2.70 vs 2.83 in mmol/l] and OA controls [mean LDL-C for RA vs OA controls: 104.5 vs 109.8 in mg/dl; 2.70 vs 2.84 in mmol/l]. The same trend was observed for total cholesterol and triglyceride levels. High-density lipoprotein cholesterol (HDL-C) levels did not differ between the RA and the control groups.
During followup, mean LDL-C levels were 96.8 mg/dl (2.50 mmol/l) for RA group matched to general controls, 100.1 mg/dl (2.59 mmol/l) for general controls, 96.5 mg/dl (2.50 mmol/l) for RA group matched to OA controls, and 99.1 mg/dl (2.56 mmol/l) for OA controls. The proportion of patients who lowered LDL-C to the recommended levels was 78.7% for both RA and general controls, and 80.0% for OA controls.
The association between lowering LDL-C levels and CV outcomes is shown in Table 2. After adjusting for other risk factors (RA status, age, sex, HTN, anti-HTN medication use, smoking status, and diabetes), a reduction of LDL-C was associated with a 29% lower risk of CV events in patients with RA plus general control cohort (HR 0.71, 95% CI 0.57–0.89) and a 50% lower risk of CV events in RA patients plus OA control cohort (0.50, 0.43–0.58). Having an RA disease was associated with a 76% increased risk of CV events after controlling for other risk factors including LDL-C status. These factors were also associated with an increased risk of CV events: older age, male sex, having HTN or anti-HTN medication use, smoking, and having diabetes. The overall model showed that there were no differences in relationships between lowering LDL-C and CV outcomes among RA and general or OA controls [p for interaction term (RA × LDL-C levels) was 0.852 for RA vs general controls, and 0.610 for RA vs OA controls; Table 2].
Association between lowering low-density lipoprotein cholesterol (LDL-C) to clinically recommended levels and CV outcomes for each cohort.
Although there were no significant differences in the relationship between lowering LDL-C and CV outcomes, we conducted a priori subgroup analyses to further show that the LDL-C effects on CV outcomes are in the same direction for RA and non-RA controls. Univariable and multivariable regression analyses for the RA and matched controls were conducted separately (Table 3). After adjusting for other risk factors (age, sex, HTN, anti-HTN medication use, smoking status, and diabetes), lowering LDL-C levels was associated with a similar degree in reduction of CV events in patients with RA identified from both cohorts (HR 0.68, 95% CI 0.46–1.02 for matched RA to general controls and HR 0.67, 95% CI 0.46–0.96 for matched RA to OA controls). A decrease in LDL-C was also associated with a reduction in CV events in general controls (HR 0.72, 95% CI 0.55–0.95), and similar HR results were found in OA controls (HR 0.76, 95% CI 0.53–1.07). Sensitivity analyses showed that the results were consistent, applying average or median LDL-C values to define LDL-C status instead of the closest value to the end of followup.
Association between lowering low-density lipoprotein cholesterol (LDL-C) to clinically recommended levels and CV outcomes for each subgroup.
DISCUSSION
We investigated the effect of lowering LDL-C in patients with RA compared with age- and sex-matched general and OA controls. Among patients with a diagnosis of hyperlipidemia and taking statins, we found that a decrease in LDL-C to the clinically recommended levels based on baseline CV risk was associated with 29% and 50% reduced CV events in RA plus matched general controls, and in RA plus matched OA controls, respectively. Interaction terms consistently showed that the effect of lowering LDL-C levels on CV outcomes was similar for both RA and matched general as well as matched OA controls. These findings are meaningful due to the complex relationship between lipid profiles and CV events for patients with RA. Myasoedova, et al5 reported increased CV risk with low and high levels of total cholesterol and LDL-C. This nonlinear relationship was also observed in independent RA cohorts by Zhang, et al21 and Liao, et al22.
Our results of reduced CV effects associated with lowering LDL-C confirm previous findings. A recent prospective statin-placebo controlled clinical trial in patients with RA found that treatment with atorvastatin 40 mg daily resulted in a 34% risk reduction for major CV events compared to placebo, although these findings are not statistically significant because of early termination of the trial16. Posthoc analyses from 2 large clinical trials also reported that patients with inflammatory joint disease (IJD) including RA and non-IJD patients had comparable lipid reduction and protection against CV events both regarding intensive and conventional lipid lowering with statins14,15.
It is important to note that our inclusion criteria allowed patients with hyperlipidemia who initiated statin therapy. From previous studies investigating LDL-C and CV outcomes in RA, only 17%–30% among patients with RA received a statin5,21. Other interventional studies compared statin users and placebo14,15,16. Our study design requiring only statin initiators was intended to avoid treatment selection bias; patients who initiated statin therapy may be different from patients who did not. Also, additional antiinflammatory properties of statin may further bias the results23,24. Thus, our study shows the benefits of lowering LDL-C levels in hyperlipidemia patients who initiated statin treatment.
Similar reductions in CV outcomes were found in subgroup analyses. The HR ranged from 0.67 to 0.76 in 4 different subgroups. Although 2 of the HR (1 in RA subgroup, 1 in matched OA controls) are not statistically significant, this should be interpreted with caution25,26,27. False-negatives and false-positives due to small sample sizes may lead to these findings25.
Our RA study population is currently taking DMARD therapy, with 11% taking biologic DMARD. About 30% of patients with RA were positive either for rheumatoid factor (RF) or anticitrullinated protein antibodies (ACPA). Also, 50% of patients with RA were considered positive for either C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) even if a large proportion of data was missing (45% missing for either RF or ACPA, and 24% missing for either CRP or ESR). It may be important to note the treatment and inflammatory status in this study population because these could influence the study results. Studies showed that inflammatory status may change lipid levels; lower levels of total cholesterol, HDL-C, and LDL-C were found among RA patients with active inflammation8,28.
Consistent with previous findings, patients with RA in this study reported lower levels of LDL-C and total cholesterol compared to lipid levels in matched general or OA controls at baseline. During the followup, the mean LDL-C levels were further decreased, and patients with RA still had lower lipid levels compared to matched controls. However, the proportion of patients who lowered their LDL-C to recommended levels was the same in RA and general controls, and the benefits of lowering LDL-C levels were also similar.
Our analyses further verified that having RA itself increased CV risk by 76% even after adjusting for traditional risk factors such as age, sex, smoking, HTN, and diabetes. These findings are consistent with previous findings, which suggest about a 50% higher risk of CV events and mortality among patients with RA relative to the general population1,2. High inflammation may explain these findings29,30,31,32; currently emerging studies on this matter may determine the reasons for the additional CV risk for patients with RA.
Our study has several potential limitations. First, this observational study design limits the causal inferences that can be made between the LDL-C levels and CV outcomes. Patients with lower LDL-C levels may have healthier lifestyles or may adhere to other CV prevention measures compared to patients with higher LDL-C levels. These factors are usually unmeasured and may result in biased effect estimates. Therefore, we should emphasize that this study investigated an “association” between LDL-C and CV outcomes rather than a “causal relationship” between the two. This study was not designed to address the CV benefits of a specific LDL-C treatment target. Instead, we emphasize that the relationship between lowering LDL-C levels and CV outcomes was not different between patients with RA and non-RA controls. Moreover, this study was not able to disentangle the benefits of lowering LDL-C and statin adherence. Our findings might be better explained by the benefits from higher adherence to statin therapy rather than lowering LDL-C.
Another limitation is that our study population is solely from 1 healthcare system and thus our results may not be generalizable to other settings. However, the relationship between LDL-C and CV outcomes should be similar in other populations, and the KPSC population has been shown to be generalizable to that of Southern California33. Moreover, we assumed that patients continue their statin therapy during the followup. Also, we considered that 1-time LDL-C measurement during the followup represents the LDL-C status for the entire followup period. This may not be plausible; statin medication adherence and/or LDL-C levels may change over time and this may affect the CV outcomes. However, results were consistent from sensitivity analyses using different LDL-C values (average or median LDL-C instead of closest LDL-C to the end of followup) or a different followup period (start to followup from the last LDL-C to the end of followup).
We were unable to evaluate inflammatory factors in this study investigating CV outcomes because about 50% of the data on those factors were missing. Also, our study focused only on patients already taking statin therapy with a hyperlipidemia diagnosis. There may be higher-risk patients who did not initiate statin therapy or who were not diagnosed with hyperlipidemia and who were not included in our study. However, we believed that investigating LDL-C status and comparing outcomes among the treated hyperlipidemia patients may be reasonable because the population is homogeneous.
Despite these limitations, our study has a number of strengths. This study investigated the association between lowering LDL-C and CV outcomes in a relatively large patient cohort having RA. Also, we were able to create age- and sex-matched non-RA and OA controls based on an ethnically diverse population so that we could examine the LDL-C and CV outcome across a diverse cohort. An additional strength is the relatively rich and high-quality clinical data. Most of the statin users (89% for patients with RA and 79% for non-RA controls) had at least 1 followup LDL-C value so that we could minimize missing data.
Our study showed that lowering LDL-C levels to clinically recommended levels based on baseline CV risk was associated with a decreased CV risk. The relationship between LDL-C and CV outcomes in RA was similar to the relationship found in matched general and OA controls. These findings are consistent with a previous study showing the similar relationship in LDL-C and CV outcomes in RA and non-RA subjects22, and support CV protective effects of lowering LDL-C with statins in RA suggested by interventional studies14,15,16. Even though specific LDL-C treatment targets are no longer recommended, our study supports the benefits of lowering LDL-C for patients using statin therapy, for both RA and non-RA controls. Future prospective studies to address this matter will be essential to better understand the benefits of lowering LDL-C in patients with RA. Further, our study showed that patients with RA still had a 76% higher risk of CV even after controlling for LDL-C status. Future studies should address excessive CV risk management strategies in addition to LDL-C in RA.
APPENDIX 1.
Definition of cardiovascular outcomes.
Footnotes
Supported by Bristol-Myers Squibb.
- Accepted for publication July 20, 2016.








{kind=link}
{kind=link}