

Abstract
Objective. To differentiate predictive factors for sustained clinical remission between elderly and younger patients with rheumatoid arthritis (RA) receiving abatacept (ABA) as an initial biological disease-modifying antirheumatic drug.
Methods. The study involved 277 biologic-naive patients with RA with high or moderate disease activity, who were treated with intravenous ABA and evaluated for 48 weeks in 43 Japanese hospitals and rheumatology clinics (the ABatacept Research Outcomes as a First-line Biological Agent in the Real WorlD study: UMIN000004651). Predictive factors associated with sustained clinical remission defined by the 28-joint Disease Activity Score with C-reactive protein (DAS28-CRP) during the 24–48–week or 36–48–week periods were determined in elderly (≥ 65 yrs, n = 148) and younger patient groups (< 65 yrs, n = 129) using logistic regression analysis.
Results. Clinical remission was achieved at 24 and 48 weeks in 35.1% and 36.5% of patients in the elderly group and 34.9% and 43.4% in the younger group, respectively. In elderly patients, anticitrullinated protein antibody (ACPA) positivity and a lower DAS28-CRP score were significantly associated with sustained clinical remission; however, a lower Health Assessment Questionnaire-Disability Index (HAQ-DI) score was not related to sustained clinical remission. In younger patients, lower DAS28-CRP and HAQ-DI scores were predictive factors for sustained clinical remission, whereas ACPA positivity was not a useful predictive factor for sustained clinical remission.
Conclusion. Although the effectiveness of ABA in biologic-naive patients with RA was equally recognized in elderly and younger patients, the baseline clinical characteristics associated with sustained clinical remission were substantially different.
- RHEUMATOID ARTHRITIS
- ABATACEPT
- CLINICAL REMISSION
- METHOTREXATE
- ANTICITRULLINATED PROTEIN ANTIBODIES
- HEALTH ASSESSMENT QUESTIONNAIRE-DISABILITY INDEX
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized mainly by chronic joint inflammation. In the synovial membrane of patients with RA, hyperplasia and inflammatory cell infiltration have been observed, including activated T cells, which are involved in the pathogenesis of RA1. Activated T cells proliferate and induce monocytes, macrophages, and synovial fibroblasts to produce proinflammatory cytokines, such as tumor necrosis factor-α (TNF-α), interleukin 1 (IL-1), and IL-61, and the stimulation of osteoclastogenesis and matrix metalloproteinase secretion2. Therefore, the suppression of T cell activation is considered a reasonable therapeutic target. Abatacept (ABA) is a soluble human recombinant fusion protein in which the extracellular domain of human cytotoxic T lymphocyte-associated molecule 4 is bound to the Fc portion of human IgG1. The safety and efficacy of ABA in patients with RA have been demonstrated in many worldwide studies for those who are methotrexate (MTX)-naive3, MTX-inadequate responders4,5, or anti-TNF-α–inadequate responders6. ABA is the fifth biological disease-modifying antirheumatic drug (bDMARD) adopted in Japan; it has been administered mainly to patients with RA who have experienced adverse events (AE) or an inadequate response to previous bDMARD such as TNF inhibitors or anti-IL-6 receptor antibodies. Consequently, no published reports have fully assessed the effectiveness of ABA in a Japanese multicenter study exclusively in biologic-naive patients with RA.
There are no specific recommendations for treatment of elderly patients with RA. In Japan, safety profiles are sometimes developed for the treatment of elderly patients with RA, especially those who have comorbidities such as renal dysfunction and chronic lung disease. Additionally, increasing age is a strong independent risk factor for serious infection in patients with RA7. Consequently, the strategies for treatment of elderly patients with RA tend to focus more on safety when compared with younger patients8. Based on the results of previous studies5,9,10, treatment with ABA is thought to be safer than with TNF inhibitors. Therefore, treatment with ABA tends to be favorable for elderly patients with RA.
The aims of our present study were to identify the predictive factors associated with sustained clinical remission for biologic-naive patients with RA and to compare them between elderly (≥ 65 yrs) and younger patients (< 65 yrs).
MATERIALS AND METHODS
The ABROAD study
The ABROAD (the ABatacept Research Outcomes as a First-line Biological Agent in the Real WorlD) study was a prospective, multicenter, open-label observational cohort study performed between December 2010 and October 2014. The study aimed to evaluate the effectiveness and safety of an intravenous (IV) infusion of ABA in biologic-naive Japanese patients with RA. Forty-three institutions participated, and all enrolled patients met either the 1987 American College of Rheumatology (ACR) classification criteria or the 2010 ACR/European League Against Rheumatism (EULAR) classification criteria11,12. All patients had moderate (MDA) or high disease activity (HDA) and had no treatment history with bDMARD and tofacitinib, although patients treated with MTX or other conventional DMARD (cDMARD) were included. The clinical effectiveness and safety of ABA treatment were evaluated over 48 weeks. Before enrollment, written informed consent was obtained from all the patients according to the Declaration of Helsinki. The study design was first approved by the Ethics Committee of Hyogo College of Medicine on November 2010, and then approved by each participating center or institution. The ABROAD study was registered with the University hospital Medical Information Network Clinical Trial Registry (UMIN000004651).
Treatment protocol
ABA was administered by an IV infusion according to the standard protocol on days 1, 15, and 29, and every 4 weeks thereafter. All enrolled patients continued to receive their background RA therapy upon study entry. A stable dose of a glucocorticoid (GC; ≤ 10 mg prednisolone equivalent daily) given for at least 28 days before treatment with ABA was permitted. However, during the study period, the new addition of MTX or GC or an increase in the dose above its baseline amount were not permitted. All the cDMARD (e.g., salazosulfapyridine) other than MTX and tofacitinib could be added during the study period.
Assessment of ABA effectiveness
Disease activity of all the patients was evaluated using the 28-joint Disease Activity Score with C-reactive protein (DAS28-CRP) and was categorized as HDA (DAS28-CRP > 4.1), MDA (2.7 ≤ DAS28-CRP ≤ 4.1), low disease activity (LDA; DAS28-CRP < 2.7), or remission (DAS28-CRP < 2.3)13. The participants’ physical function was assessed using the Health Assessment Questionnaire-Disability Index (HAQ-DI)14. The DAS28-CRP and HAQ-DI scores were recorded at baseline and then at 4, 12, 24, 36, and 48 weeks after the initiation of ABA. The clinical effectiveness of ABA was compared between elderly (≥ 65 yrs) and younger patients (< 65 yrs). Associations between the baseline patient profiles, including the disease activity, concomitant MTX use, and laboratory findings at baseline, and sustained clinical remission were examined using logistic regression analysis. Sustained clinical remission was defined as clinical remission (DAS28-CRP) that was achieved at 48 weeks and continued over 12 weeks during the final 24 weeks of the study period. Instances of drug withdrawal were not included in the assessment of sustained clinical remission, even if clinical remission was observed when the drug was discontinued.
Statistical analysis
Statistical analysis of the 2-group comparison was performed using the paired Student t test (or Wilcoxon rank sum test when appropriate) for paired data and the Student t test (or Mann-Whitney U test when appropriate) for unpaired data. The chi-square test (or Fisher’s exact test when appropriate) was used to compare categorical data. Missing data on clinical characteristics of patients who discontinued their participation before 48 weeks or could not be evaluated through regular visits were imputed using a last observation carried forward analysis. The log-rank test was used to compare the retention rate of ABA treatment and each withdrawal rate because of AE or infection. Multivariate logistic regression analysis with stepwise backward selection was performed to identify the variables at baseline that were potentially associated with sustained clinical remission. All statistical tests were 2-sided, and significance was defined as p < 0.05. All analyses were performed using JMP 11 (SAS Institute Inc.).
RESULTS
Characteristics of the patients
In our present study, 277 biologic-naive patients with RA with HDA or MDA were evaluated. Their demographic and clinical characteristics at baseline are shown in Table 1. The mean and median ages of the participants were 63.2 ± 13.3 years and 65 years, respectively. The proportion of patients whose age was in the 70s was 31.0%, which was the highest percentage of any age group by decade (Supplementary Figure 1, available online at jrheum.org). The percentage of concomitant MTX use was 69.0% with a mean dose of 7.8 ± 2.7 mg/week, whereas GC use was 55.2% with a mean dose of 5.1 ± 2.4 mg/day. Rheumatoid factor (RF) and anticitrullinated protein antibody (ACPA) positivity rates among patients with measurements were 79.2% and 84.4%, respectively.
Patients’ profiles in the ABROAD study. A significance test was performed between the elderly and younger patient groups. Values are mean ± SD: median unless otherwise specified.
One hundred forty-eight patients (53.4%) were ≥ 65 years old (elderly group) and 129 (46.6%) were < 65 years old (younger group). The ratio of men to women, RA disease activity, and disease duration were similar between the groups. The mean HAQ-DI score was higher in the elderly patient group than in the younger patient group (1.24 ± 0.73 vs 0.94 ± 0.73, p = 0.0011). The percentage of concomitant GC use and the mean GC dosage were similar between the groups. However, MTX was more frequently used in the younger patient group than in the elderly patient group (81.4% vs 58.1%, p < 0.0001). At the initiation of ABA treatment, 1 patient in the elderly group used 2 cDMARD concomitant with MTX, and 10 and 1 used 2 and 3 cDMARD without MTX, respectively. In the younger group, 5 patients used 2 cDMARD with MTX, and 3 and 2 patients used 2 and 3 cDMARD without MTX, respectively. Eleven patients were administered additional cDMARD, other than MTX, during the study period [tacrolimus (n = 7), salazosulfapyridine (n = 3), and mizoribine (n = 1); Supplementary Table 1, available online at jrheum.org]. Although ACPA and RF positivity rates were similar between the groups, a highly positive ACPA (≥ 13.5 U/ml; > 3× the upper limit of normal12) was more frequently recognized in the elderly group than in the younger group.
Clinical effectiveness and safety
Figures 1A and 1B illustrate the number of patients who achieved sustained remission on each time course.
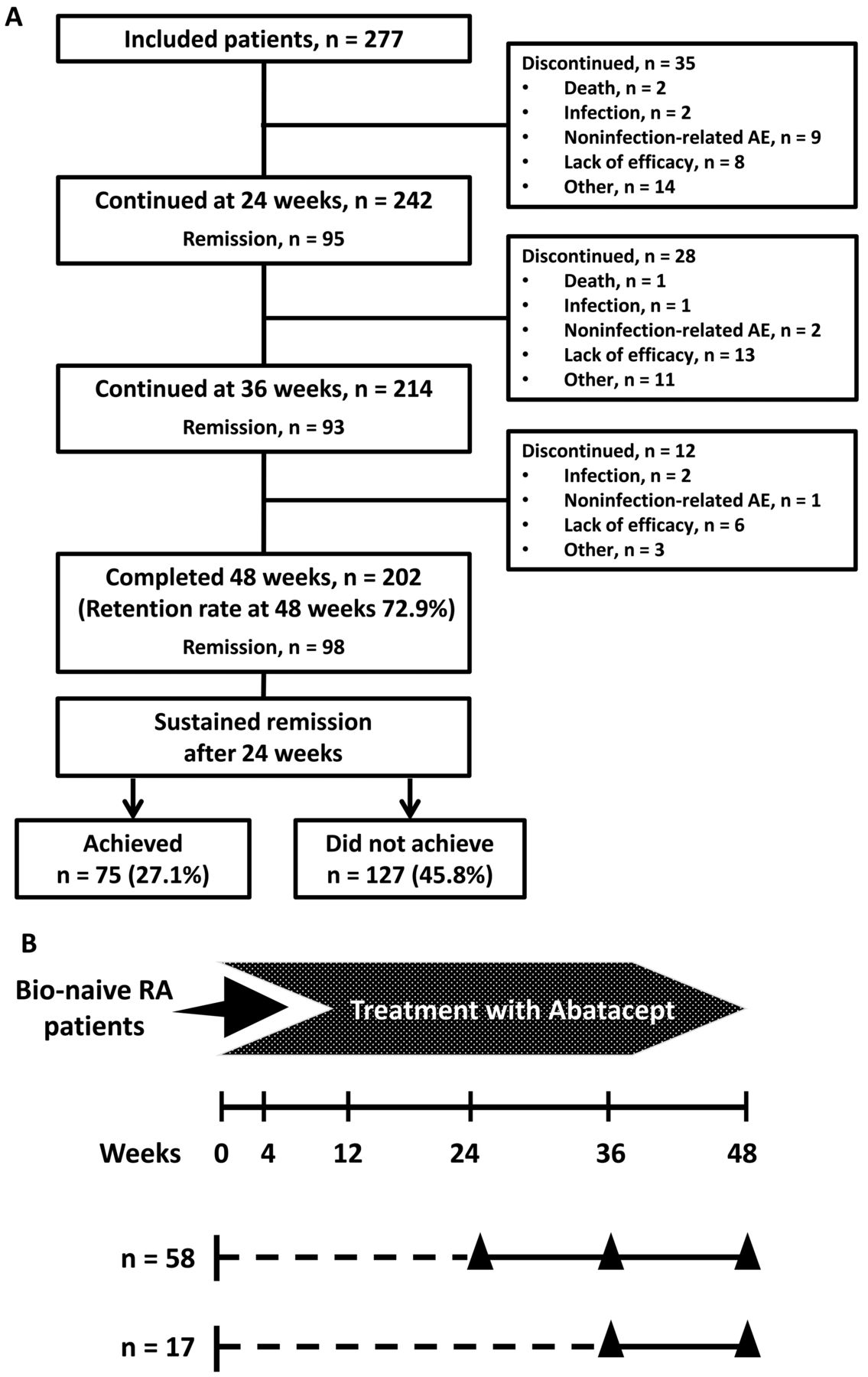
A. Patients’ disposition. Sustained clinical remission was defined as clinical remission (DAS28-CRP < 2.3) that was achieved at 48 weeks and continued over 12 weeks during the final 24 weeks in the study period. Cases of treatment withdrawal were not considered to have achieved sustained clinical remission, even if clinical remission was observed when the drug was discontinued. Seventy-five of the 202 patients who completed the study achieved sustained clinical remission. The reasons for discontinuing treatment other than AE and a lack of efficacy were lost to followup (n = 8), withdrawal of consent (n = 7), remission/major improvement (n = 3), economic reason (n = 2), other (n = 4), and unknown (n = 4). B. Evaluation points in our cohort. Fifty-eight and 17 patients achieved sustained clinical remission during weeks 24–48 and 36–48, respectively. Triangles indicate the points of attained clinical remission. DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein; AE: adverse events; RA: rheumatoid arthritis.
Clinical effectiveness of ABA treatment at each evaluation point is shown in Figure 2. After ABA treatment, the mean DAS28-CRP score significantly decreased from 4.58 ± 1.14 at baseline to 3.57 ± 1.15 at Week 4 (p < 0.0001) and to 2.79 ± 1.27 at Week 48 (data not shown). At weeks 4, 12, 24, and 48, DAS28-CRP–defined clinical remission rates were 11.9%, 28.5%, 35.0%, and 39.7%, respectively, and LDA rates were 23.1%, 45.5%, 50.5%, and 53.8%, respectively (Figure 2A). As shown in Figure 2B, the clinical remission rate at each point and the sustained clinical remission rate after 24 weeks were equivalent in both elderly and younger patients. Additionally, the LDA achievement rate at each point did not differ between the 2 age groups (Supplementary Figure 2, available online at jrheum.org). Treatment with ABA significantly lowered the mean HAQ-DI score from 1.10 ± 0.74 at baseline to 0.90 ± 0.73 at Week 4 (p < 0.0001), and it continued to decrease to 0.74 ± 0.72 at Week 48 during the course of treatment. The percentage of patients achieving functional remission (HAQ-DI ≤ 0.5) was increased to 50.2% at 48 weeks (Figure 2C). However, in the elderly group, the functional remission rate was significantly lower than in the younger group during the entire study period, although it persistently increased from 20.5% at baseline to 40.9% at Week 48 (Figure 2D).

Clinical effectiveness of ABA in biologic-naive patients with rheumatoid arthritis. A. The change in the proportion of patients who achieved clinical remission and LDA after ABA treatment. All the patients had moderate disease activity or high disease activity at baseline, and 35.0% and 39.7% of patients achieved clinical remission at 24 and 48 weeks, respectively. B. Comparison of the clinical remission rate between the elderly and younger patient groups. Sustained remission was defined as clinical remission (DAS28-CRP < 2.3) that was achieved at 48 weeks and continued over 12 weeks during the final 24 weeks in the study period. There were 27.7% of elderly patients and 31.8% of younger patients who achieved sustained remission. C. The change in the mean values of the HAQ-DI score and the proportion of patients achieving functional remission after ABA treatment. D. Comparison of the functional remission rate between the elderly and younger patient groups. ABA: abatacept; LDA: low disease activity; DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein; HAQ-DI: Health Assessment Questionnaire-Disability Index; LOCF: last observation carried forward.
Baseline predictive factors for achieving sustained clinical remission in each age group
The predictive factors for sustained clinical remission were determined in each age group (Table 2). In univariate logistic analysis, significant variables affecting the sustained clinical remission for elderly patients were ACPA positivity, the DAS28-CRP score, and the HAQ-DI score. However, significant variables associated with sustained clinical remission for younger patients were concomitant MTX use, Steinbrocker stage I or II, the DAS28-CRP score, the HAQ-DI, and disease duration. RF positivity was not associated with sustained clinical remission in either age group in univariate analysis. HAQ-DI was significantly correlated with both the DAS28-CRP score and disease duration in both age groups. Therefore, multivariable logistic regression analysis was performed separately in 2 models, which included DAS28-CRP and disease duration (Model A) and HAQ-DI alone (Model B). The multivariable logistic regression analysis (Model A) indicated that that ACPA positivity (OR 8.141, p = 0.0138) was a useful independent predictive factor of sustained clinical remission in elderly patients, and a higher DAS28-CRP score at baseline was negatively associated with achieving sustained clinical remission in both elderly and younger patients (in elderly patients, OR 0.560, p = 0.0069; in younger patients, OR 0.460, p < 0.0001). In younger patients, concomitant MTX use (OR 3.183, p = 0.0588) had a tendency to be associated with sustained clinical remission, although the difference was not statistically significant. In the second multivariable logistic regression analysis (Model B), ACPA positivity (OR 6.792, p = 0.0270) was the only useful independent predictive factor for achieving sustained clinical remission in elderly patients, while in younger patients, a higher HAQ-DI score at baseline (OR 0.188, p < 0.0001) was negatively associated with sustained clinical remission.
Logistic regression analysis of baseline characteristics associated with sustained clinical remission with abatacept treatment. An increase in the continuous variable (i.e., the DAS28-CRP, HAQ-DI, and disease duration) represented a lower sustained clinical remission rate. Univariate analysis variables were included in a multivariable logistic model, and the model was developed using a stepwise selection process. The multivariate logistic regression model contained 5 variables (female sex, concomitant MTX use, ACPA positivity, RF positivity, and Steinbrocker stage I or II). In addition to these variables, Model A included DAS28-CRP and disease duration, while Model B contained HAQ-DI.
Retention rate and safety of treatment with ABA in different age groups
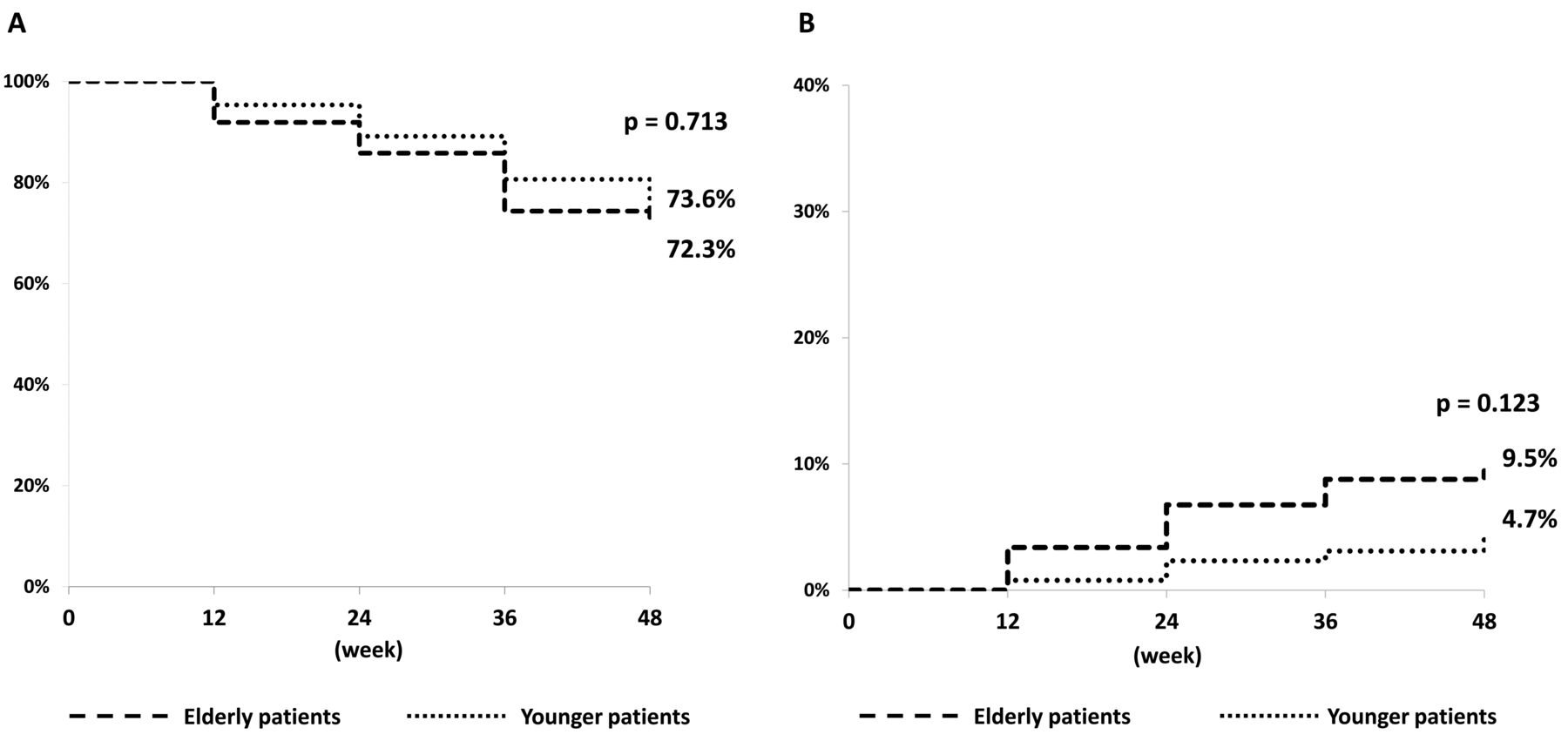
Figure 3 shows the retention rate of ABA treatment and the withdrawal rate owing to AE during the study period in each age group. Retention rates at 48 weeks in the elderly and younger patient groups were 72.3% and 73.6%, respectively (p = 0.713). No significant difference was found in the withdrawal rate of treatment with ABA owing to AE in each age group (elderly group: 9.5%, younger group: 4.7%, p = 0.123). The reasons for discontinuation of treatment because of AE are summarized in Table 3. There were 3 deaths in the elderly patient group during the course of the study; the causes of death for each patient were Pneumocystis jirovecii pneumonia, interstitial pneumonia, and acute myocardial infarction (MI). All patients who died were over 80 years old. The patient who developed interstitial pneumonia received MTX therapy and did not have an abnormal shadow on chest radiography at the beginning of the ABA treatment. Therefore, this may be a case of adverse reaction induced by ABA, and MTX may have been involved. The patient who died of acute MI had severe atherosclerosis and an ascending aortic aneurysm before treatment with ABA. Thus, although different from the other cases, MI may not have been caused by ABA. Four patients in the elderly patient group and 1 in the younger patient group discontinued ABA treatment because of infection. The most frequently reported infections were pneumonia (elderly group: 3 patients, younger group: 1 patient) and pyogenic arthritis (elderly group: 1 patient). There was no statistically significant difference in withdrawal rate because of infection between age groups (elderly group: 3.4%, younger group: 0.8%, p = 0.137).

Retention rates and incidence of adverse events over 48 weeks of abatacept treatment. A. Retention rate in different age groups. Retention rates based on all unfavorable causes at 48 weeks: 72.3% in the elderly and 73.6% in the younger group. B. Withdrawal rate because of adverse events in different age groups. Withdrawal rate because of AE at 48 weeks: 9.5% in the elderly and 4.7% in the younger group.
Summary of patients discontinuing treatment because of adverse events in each age group. Values are n unless otherwise specified.
DISCUSSION
To our knowledge, our present study is the first to assess the effectiveness and safety of ABA for biologic-naive Japanese patients with RA in a multicenter trial. Our effectiveness data seemed equivalent to those found for TNF inhibitors; the RECONFIRM-2 study showed that 27.8% of biologic-naive Japanese patients with RA achieved clinical remission at 22 weeks and 27.6% at 54 weeks with infliximab (IFX) treatment15. In the DANBIO registry, 39%, 33%, and 27% of patients with RA who received adalimumab (ADA), etanercept (ETN), and IFX, respectively, as the first biologic treatment obtained clinical remission (DAS28 < 2.6) at 12 months16. In addition, several studies have shown that the efficacy of TNF inhibitors was inferior in elderly patients with RA compared to younger patients with RA16,17,18, whereas other reports have demonstrated that the effectiveness was equally observed, irrespective of age19,20. As for tocilizumab (TCZ) treatment, there are a few reports on effectiveness data that compare elderly and younger patients with RA. Pers, et al reported that the effectiveness of TCZ was inferior in elderly patients with RA compared with younger patients with RA21. In our study, although the rate of clinical remission seemed slightly higher in younger patients than in elderly patients at 48 weeks, the effectiveness of ABA at 24 weeks, which is the timepoint for treatment decision making, was not associated with age in biologic-naive patients with RA. Although our study was performed in biologic-naive patients with RA, the proportion of elderly patients (≥ 65 yrs) was higher than that of other previous registries with ABA22,23,24. We speculate that a reason for this is that TNF inhibitors tend to be used less frequently for elderly patients with RA because in Japan, older age was reported as one of the risk factors for serious infection from the postmarketing surveillance programs for IFX, ETN, and ADA25,26,27.
Our study, however, clearly showed that the predictive factors associated with sustained clinical remission after 24 weeks are different between elderly and younger patients. Being biologic-naive was an independent predictive factor for achieving LDA or a favorable EULAR response at 24 weeks28, whereas concomitant MTX use was independently associated with the improvement of clinical effectiveness from 24 weeks after initiating ABA treatment onward29. The Orencia and Rheumatoid Arthritis (ORA) registry, a nationwide prospective cohort study that investigated the longterm safety and effectiveness of ABA for treating RA and was designed by the French Society of Rheumatology, showed that anticyclic citrullinated peptide antibody (anti-CCP) positivity was associated with a EULAR response at 6 months and a high ABA survival rate30. Because our study and these reports do not include radiography data for the joints, we selected patients with sustained clinical remission, which is strongly recommended by the EULAR guideline31, because it can be linked to the inhibition of structural joint destruction32. Of note, our results suggest that the predictive factors for a clinical response to ABA are similar to the previous items, but they were different according to patients’ ages.
First, ACPA positivity was an independent predictive factor in elderly patients, but not in younger patients. In fact, accumulating data suggest that ACPA-positive patients may respond better to ABA and rituximab33,34,35. ACPA positivity, therefore, may be associated with sustained clinical remission in a certain subset of patients treated with ABA; however, it should be elucidated why ACPA positivity is linked to the effectiveness of ABA only in elderly patients. In the 2-year AMPLE study (Abatacept versus Adalimumab Comparison in Biologic-naïve RA Subjects with Background Methotrexate), patients with a high concentration of anti-CCP2 at baseline had a better clinical response with ABA than those with a lower concentration of anti-CCP2 at baseline36. In our study, the proportion of patients with a highly positive ACPA was higher in the elderly group than in the younger group, which may contribute to the superior effectiveness of ABA in elderly patients compared with younger patients. In contrast with our results, in the ORA registry including 2-year followup data23, ACPA positivity was not a predictive factor for good or moderate EULAR response with ABA in very elderly patients (≥ 75 yrs). On the other hand, in elderly patients (65–74 yrs), ACPA positivity was a predictive factor for a good or moderate EULAR response. Thus, we could not directly compare these results with the results of our study because of the differences in both the categorization of patients’ ages and the followup period.
ABA can be used as monotherapy, and ABA efficacy with and without MTX was comparable in the DANBIO37 and ORA Registries30. The Assessing Very Early Rheumatoid arthritis Treatment (AVERT) study, a phase IIIb, randomized, controlled trial that evaluated drug-free remission with a subcutaneous infusion of ABA in MTX-naive patients with early RA, indicated that the clinical efficacy of ABA concomitant with MTX treatment was superior to ABA monotherapy when administered continuously for 12 months38. In our present study, the additional effect of MTX on ABA was not apparent. The aim of our present study was not direct comparison between the effectiveness of ABA with and without MTX. However, as demonstrated by our results, concomitant MTX tended to be associated with the achievement of sustained clinical remission in younger patients. Therefore, MTX use may be recommended, if possible, especially in younger patients with RA.
Takeuchi, et al reported that a lower DAS28 score and a lower HAQ-DI score at baseline were independent predictive factors for achieving clinical remission at 52 weeks of TCZ treatment39. In multiple logistic regression analysis in our present study, a lower clinical disease activity and lower HAQ-DI score were also shown to be important factors, but their association with sustained remission depended on patients’ age. Both factors were distinctly related to sustained clinical remission in younger patients. However, in elderly patients, the effect of a lower HAQ-DI on achieving sustained clinical remission was smaller than that of lower clinical disease activity. Therefore, the favorable characteristics for ABA treatment in elderly patients are not similar to those in younger patients.
In the ABROAD study cohort, 3 deaths were reported during the study period. Mortality was higher in our study than in previous reports3,4,5,40, and this may be because our cohort included patients older than those in the previous reports. Lahaye, et al reported that the incidence of death in the ORA registry was higher with age, and mortality among very elderly patients (≥ 75 yrs) treated with ABA was 8.65 per 100 patient-years23. Hence, we considered that mortality in our study was not necessarily high. The discontinuation rate of ABA treatment because of AE or infection appeared to be high in elderly patients in comparison with younger patients, although there was no statistically significant difference. Based on the results of previous studies5,9,10, ABA treatment is thought to be safer than TNF inhibitors. However, ABA treatment should be closely monitored, similarly to treatment with TNF inhibitors, especially in elderly patients.
Our study has some limitations. First, radiographic data were absent. Given the importance of a joint protective effect for demonstrating clinical effectiveness, the ability to evaluate radiographic changes in patients treated with ABA will be necessary in the future. Second, in patients treated without MTX, the reasons MTX was not used are unknown. Hence, we could not indicate how the reasons not to treat with MTX influenced the ability to reach sustained remission. Finally, the proportion of patients without ACPA positivity might be too small to produce a strong result. In addition, ACPA was not measured in about one-third of patients before initiation of ABA treatment; thus, the number of participants who could be evaluated was substantially decreased.
The ABROAD study demonstrated that ABA shows a sustained clinical effect over 24 weeks in biologic-naive patients with RA, irrespective of age. ABA treatment may be strongly recommended for elderly patients with MDA who are ACPA-positive, as well as younger patients with a low HAQ-DI and MDA.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
The authors wish to acknowledge the patients and the members of the ABROAD Study Group.
APPENDIX 1.
List of study collaborators. The ABROAD Study Group: K. Maeda, H. Nakahara, S. Higa, Y. Hamano, M. Nishide, S. Nozaki, NTT West Osaka Hospital; A. Yamamoto, Y. Kukita, T. Seno, H. Nagahara, Kyoto Prefectural University of Medicine; H. Hashimoto, Rinku Hashimoto Rheumatology Orthopedics; A. Yokota, Yokota Clinic; K. Miki, Amagasaki Central Hospital; N. Shinmyo, T. Fujimura, Kashiba Asahigaoka Hospital; H. Goto, M. Tada, T. Koike, Y. Sugioka, T. Okano, Osaka City University; T. Fujimoto, Nara Medical University; Y. Ozaki, Y. Son, Kansai Medical University; M. Kitano, Hyogo College of Medicine; S. Irimajiri, Rinku General Medical Center; T. Hidaka, Zenjinkai Shimin-no-Mori Hospital; Y. Nozaki, M. Funauchi, S. Hino, M. Sugiyama, T. Shiga, Kinki University School of Medicine; T. Kuroiwa, Yukioka Hospital; I. Yoshii, Yoshii Hospital; M. Hashimoto, N. Yamakawa, Kyoto University; K. Ohmura, Jyujyo Takeda Rehabilitation Hospital; K. Hatta, T. Azuma, Tenri Hospital; T. Igawa, K. Inoue, Osaka Rehabilitation Hospital; T. Takeuchi, Hayaishi Hospital; M. Tanaka, Kanazawa Medical University; K. Higami, Higami Hospital; M. Namiki, T. Yamazaki, Takarazuka City Hospital; T. Nakatani, T. Saito, Kishiwada City Hospital; Y. Imura, T. Nakajima, Osaka Red Cross Hospital; S. Namiuchi, K. Akashi, M. Nakata, Osaka Saiseikai Nakatsu Hospital; T. Takeuchi, Osaka Medical College; A. Omoto, Japanese Red Cross Kyoto Daiichi Hospital; A. Nanpei, Osaka Rosai Hospital; S. Watanabe, Watanabe Orthopedic Clinic; K. Ushio, Ushio Orthopedic Clinic; Y. Hideki, Nijoekimae Clinic; S. Oshima, Osaka Minami Medical Center; S. Kashiwagi, Amagasaki Iryou-Seikyou Hospital; H. Yokoyama, Yokoyama Orthopaedic Clinic; M. Morimoto, Kobe City Medical Center West Hospital; Y. Uesugi, Saiseikai Noe Hospital; S. Mokuda, M. Onishi, Dogo Spa Hospital; H. Yanagita, National Hospital Organization Utano Hospital; K. Sugimoto, Fukui General Hospital; T. Sasaki, Nishinomiya Watanabe Hospital; A. Hashiramoto, Kobe University.
- Accepted for publication July 6, 2016.








{kind=link}
{kind=link}
{kind=link}