
Abstract
Objective. To assess bladder toxicity of cyclophosphamide (CYC) and uroprotective effect of mesna in rheumatic diseases.
Methods. Data of 1018 patients (725 women/293 men) treated with CYC were evaluated in this retrospective study. All of the following information was obtained: the cumulative CYC dose, route of CYC administration, duration of therapy, concomitant mesna usage, and hemorrhagic cystitis. Cox proportional hazard model was used for statistics.
Results. We identified 17 patients (1.67%) with hemorrhagic cystitis and 2 patients (0.19%) with bladder cancer in 4224 patient-years. The median time for diagnosis to hemorrhagic cystitis was 10 months (4–48) and bladder cancer was 8 years (6–10.9). There were 583 patients (57.2%) who received mesna with intravenous CYC therapy. We observed similar incidence rate for hemorrhagic cystitis in both patient groups concomitantly treated with or without mesna [9/583 (1.5%) vs 8/425 (1.8%) respectively, p = 0.08]. Cumulative CYC dose (HR for 10-g increments 1.24, p < 0.001) was associated with hemorrhagic cystitis.
Conclusion. Cumulative dose was the only risk factor for hemorrhagic cystitis in patients treated with CYC. No proof was obtained for the uroprotective effect of mesna in our cohort.
- HEMORRHAGIC CYSTITIS
- MESNA
- RHEUMATIC DISEASES
Cyclophosphamide (CYC), despite significant toxicity, remains a drug of choice for the severe forms of rheumatic diseases, including systemic lupus erythematosus (SLE), systemic sclerosis (SSc), and vasculitis. Like its clinical effect, toxicity also varies depending on the dose, route of administration, cumulative dose, or duration of the treatment1,2,3,4,5,6,7,8.
CYC is an alkylating agent, acts as a prodrug, and is metabolized to active and inactive form by the liver. Its inactive metabolite — acrolein, which is directly toxic to the bladder — can cause hemorrhagic cystitis9,10,11. To prevent the toxicity of acrolein, concomitant mesna administration is recommended based on 4 small controlled trials of ifosfamide therapy, a structural analog of CYC12,13,14,15,16,17,18. CYC doses used in cancer chemotherapy are significantly higher than the doses commonly used in rheumatology practice, and to date, no controlled trials support the concurrent use of mesna with CYC in rheumatology practice, so we conducted a retrospective analysis to address this issue.
Here, we aimed to analyze the incidence rate of urotoxicity in patients receiving CYC for severe rheumatic diseases. We also questioned the uroprotective effect of mesna in patients treated with CYC for rheumatologic disorders.
MATERIALS AND METHODS
We retrospectively analyzed the data of 1156 patients treated with CYC for severe manifestations of various rheumatologic diseases. Subjects for our study were selected from the rheumatology clinics of 13 university hospitals that have collected clinical and laboratory data. All of these rheumatology clinics have continuous approval from the University Health Research Ethics Boards and informed consent was obtained from all patients for accessing their data for research studies. The database was searched for patients with SLE, SSc, vasculitis, and other autoimmune diseases treated with CYC. Because hemorrhagic cystitis was expected to occur during or shortly after CYC treatment, patients exposed to CYC for at least 3 months were included for analysis. We excluded patients from the analysis if there was missing information on treatment protocol or followup.
According to our therapy protocol, intermittent intravenous (IV) pulses of CYC were prescribed at doses of 0.5–0.6 g/m2 every 2–4 weeks or oral CYC were given in a dosage of 1.5–2 mg/kg per day. Mesna, at 20–40% of the CYC dose, was administered — if it was used — intravenously 10 min before CYC administration in some of the outpatient centers in the cohort. The route of CYC administration (orally or IV) and whether to use mesna were solely dependent on the preference of the treating physician.
Hemorrhagic cystitis was diagnosed based on the basic urinalysis screen during the followup period. All patients with hematuria were evaluated by urinary tract ultrasonography, urine culture, and urinary analysis to exclude other causes of hematuria. Either microscopic or macroscopic hematuria occurring in the absence of urinary tract infection, nephrolithiasis, erythrocyte casts, or declining renal function was defined as hemorrhagic cystitis. Cystoscopic confirmation of hemorrhagic cystitis was not required, but tissue biopsy was requested for diagnosis in case of bladder cancer.
In addition to demographic characteristics, the route of drug administration, cumulative dose, and time span of CYC therapy, as well as concomitant mesna use, were extracted from the medical records. The effect of disease subset on hemorrhagic cystitis was also assessed. The incidence of bladder carcinoma was also evaluated in a subgroup of patients who were being followed at least 5 years after last CYC dose.
Statistical analysis
Continuous variables are expressed as the mean ± SD for normal distributions and as the median (interquartile range) for abnormal distributions. Comparisons between groups were made using nonparametric Mann-Whitney U tests.
Univariate Cox proportional hazard analyses were performed using hemorrhagic cystitis occurrences as dependent variables and the following 4 variables as covariates: (1) cumulative CYC dose (analyzed as continuous variable), (2) duration of CYC therapy (analyzed as continuous variable), (3) mesna usage (dichotomized as ever used vs never used), and (4) CYC administration route (stratified as ever-oral vs IV). All variables that detected p ≤ 0.20 in univariate analysis were entered into the multivariate Cox regression model, and then selected by backward stepwise algorithm. P values ≤ 0.05 were considered significant. All statistical analysis was performed using the SPSS 11.5 statistical package program.
RESULTS
Clinical features of the patients
The data of 1018 patients (725 women and 293 men) treated with CYC for autoimmune diseases (n = 729) and vasculitis (n = 289) from 13 rheumatology centers were analyzed (Table 1). Because of missing detailed information and/or insufficient monitoring after CYC exposure on the database, 138 patients were excluded from the study.
Clinical characteristics of the 1018 patients treated with CYC.
The median CYC dose was 9 g (6–14, range 1.5–180), duration of CYC treatment was 12 months (range 2–102), and followup time after CYC treatment was 36 months (range 3–365). CYC was administered only intravenously in 928 patients (90.6%), exclusively orally in 49 patients (4.8%), and by both routes in 41 patients (4%). The mean CYC dose was significantly higher in the ever-oral route compared with the IV-only route [27 g (12.5–46.2) vs 9 g (6–12), respectively, p < 0.001]. There were 583 patients (57.4%) who received mesna with IV CYC infusion. None of the patients receiving oral CYC used mesna. Cumulative CYC dose was not different between patients with or without mesna use (p > 0.05; Table 2).
Incidence of hemorrhagic cystitis following CYC therapy. Values are median (IQR) or n (%).
Urinary tract toxicity
We identified 17 patients (1.67%) with hemorrhagic cystitis and 2 patients (0.19%) with bladder cancer in a median time of 10 months (4–48) and 8 years (6–10.9), respectively. The median cumulative dose of CYC in our cystitis patients was 10 g (range 2.5–180).
Hemorrhagic cystitis incidence was similar in patients treated with mesna [with vs without mesna 9/585 (1.53%) vs 8/424 (1.88%), respectively, p = 0.08]. Seven patients (7.7%) developed hemorrhagic cystitis in the ever-oral CYC group; so did 10 patients (1.07%) in the IV CYC group (p = 0.01).
Among those 1018 patients, 2 bladder cancers (transitional cell cancer) occurred. One patient was receiving oral CYC in a total cumulative dose of 108 g and the other of 116 g.
Predictors of hemorrhagic cystitis
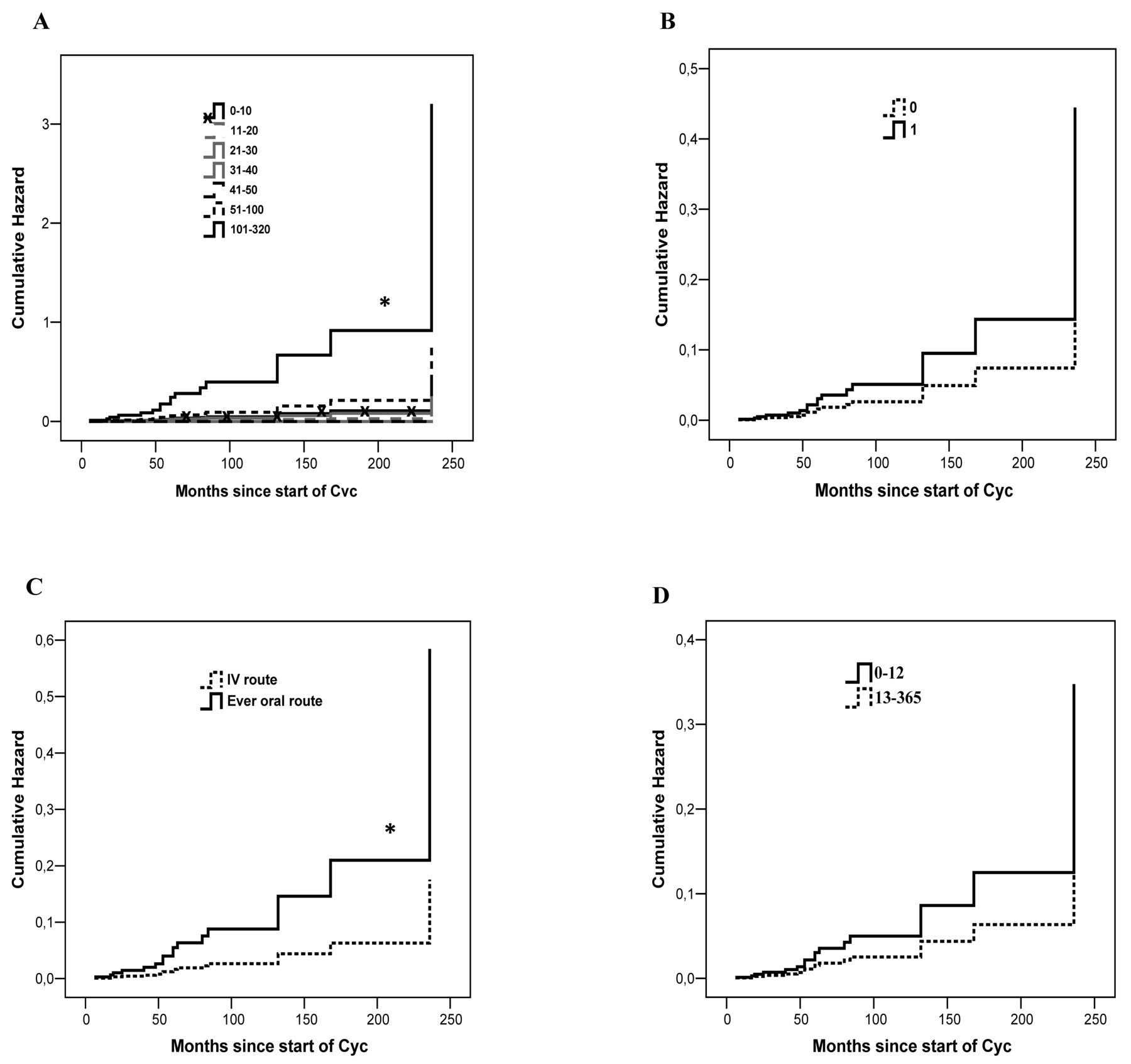
In Table 3, univariate analysis for predictors of hemorrhagic cystitis are summarized. Briefly, ever-oral administration of CYC and cumulative CYC dose were found as predictors of hemorrhagic cystitis occurrence (p = 0.01 and p < 0.001, respectively). Disease subset, mesna use, and duration of CYC treatment did not satisfy the statistical significance. The following 4 variables were included in the multivariate survival analysis: (1) mesna usage, (2) cumulative CYC dose, (3) CYC therapy duration, and (4) CYC administration route. Figure 1 shows the relationship between predisposing factors and hemorrhagic cystitis. Cumulative CYC dose was found as the only independent variable for hemorrhagic cystitis risk (HR for 10-g increments 1.24, 95% CI 1.12–1.38, p < 0.001; Table 3).

{kind=link}
Cumulative incidence of hemorrhagic cystitis in all patients stratified by (A) cumulative CYC dose (g), (B) concomitant mesna administration, (C) CYC administration route, and (D) CYC therapy duration (mos). * p < 0.05. CYC: cyclophosphamide.
Cox proportional hazard regression analysis of predisposing factors for hemorrhagic cystitis occurrence.
DISCUSSION
In our study, we identified 17 hemorrhagic cystitis and 2 bladder cancers in patients treated with CYC in 4224 patient-years of exposure. In the risk factor analysis, cumulative CYC dose was the only significant factor associated with hemorrhagic cystitis. However, the model failed to show significant effect of mesna for protection.
Hemorrhagic cystitis is one of the well-known side effects of CYC therapy. However, the incidence of hemorrhagic cystitis varies in different studies in the rheumatology literature. Monach, et al1 published a review on bladder toxicity of CYC therapy in a mixed group of patients with granulomatosis with polyangiitis4,19,20,21,22,23,24,25, SLE3,26,27,28,29,30, SSc31,32, and rheumatoid arthritis33,34 in 2010. The review showed a significantly greater incidence rate of hemorrhagic cystitis in patients treated with oral CYC compared with IV treatment regimens, regardless of disease subset. However, this finding could be explained mainly by a more than 3 times higher cumulative CYC dose (> 100 g) in patients receiving oral CYC. Because the cumulative dose is significantly lower and/or hydration is more prominent in intermittent IV CYC than oral CYC regimens, Monach, et al concluded that total dose of CYC is the main factor for bladder toxicity rather than the route of administration3,4,19,20,33. In our study, our incidence rate was substantially lower (1.67%) compared with the studies. It is likely that lesser cumulative CYC dose (median 10 g) and the higher proportion of IV CYC use may explain the big difference in hemorrhagic cystitis development in our cohort. Another issue is that this is not a prospective cohort and the presence of hemorrhagic cystitis is accepted based on personal medical records. Therefore, the true incidence might be overlooked.
We could not show increased urotoxic event depending on the route of CYC regimen. Some of the previous studies supported a favorable safety profile of intermittent CYC, as opposed to daily oral regimen35,36,37,38. In univariate analysis, both oral CYC administration and cumulative CYC dose were independent risk factors for hemorrhagic cystitis development in our data. But in multivariate analysis, the effects of administration route disappeared.
Mesna is known to reduce bladder toxicity of CYC and is recommended to use concomitantly with CYC in some chemotherapy regimens18 and in rheumatology protocols39,40. Randomized controlled trials on uroprotective effects of mesna were designed for chemotherapy regimens, including patients receiving high dose IV CYC or ifosfamide therapy41,42,43. These studies reported that mesna administration was more effective than hyperhydration in preventing hematuria. In oral CYC therapy of patients with granulomatous polyangiitis, hemorrhagic cystitis incidence have been reported as 12% with mesna prophylaxis in 1 study20 and nearly 50% without mesna prophylaxis in other studies4,44. These results suggest that mesna may have uroprotective effects during oral CYC therapy. However, definition and diagnosis of cystitis are different among these studies, so comparison of the results of these studies is not an appropriate approach. In 2 other studies, the incidence of cystitis in IV CYC with mesna was reported as much lower in patients with connective tissue diseases28,44. Because of the limited number of studies that addressed this issue and lack of comparative studies in the literature, data on the efficacy of mesna in preventing cystitis are still lacking. To our knowledge, our study is the largest series in the literature to compare the protective effect of mesna. We should emphasize that nearly half of our patients received mesna and all of them were receiving IV CYC. In the hazard analysis, the incidence of hemorrhagic cystitis was not different between patients, regardless of mesna use. It is also worth mentioning that none of the patients treated with oral CYC received concomitant mesna in our cohort. Therefore, our results are not useful for comparisons.
Our retrospective study reveals that cumulative CYC dose is the most important predictor for hemorrhagic cystitis development. However, we cannot suggest that mesna has a protective effect for hemorrhagic cystitis. Prospective studies are needed to determine the uroprotective effect of mesna.
- Accepted for publication May 19, 2015.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.