

Abstract
Objective. To estimate the prevalence of inflammatory back pain (IBP) and axial spondyloarthritis (axSpA) using the Assessment of SpondyloArthritis International Society (ASAS) classification criteria among employees in a university.
Methods. In the first stage of the study, a face-to-face interview was done using a standard questionnaire to investigate IBP in 381 subjects randomly selected from 2894 employees at Dokuz Eylul University in Izmir, Turkey. In the second stage, subjects with back pain for ≥ 3 months and age at onset < 45 years were evaluated for axSpA using the ASAS criteria. Both the European Spondyloarthropathy Study Group (ESSG) criteria and Amor criteria were used for the classification of the whole group of spondyloarthritis (SpA).
Results. There were 131 male and 250 female subjects (mean age: 38.0 yrs). Twenty-five subjects (6.6%) were classified as having IBP according to the ASAS criteria. The prevalence of IBP according to the Berlin and Calin criteria was 7.1% and 21.5%, respectively. The prevalence of axSpA was estimated at 1.3% according to the ASAS classification criteria (0.5% for radiographic axSpA and 0.8% for nonradiographic axSpA). A total of 7 patients (1.8%) fulfilled both the Amor and ESSG criteria for the whole group of SpA.
Conclusion. This is the first prevalence study of IBP and axSpA using ASAS classification criteria in the Turkish population. The prevalence estimates of IBP and axSpA reported here are within the upper range of other studies in European countries and the United States.
Spondyloarthritides are among the most prevalent inflammatory rheumatic diseases1. There is a considerable diagnostic delay (8.9 yrs) in ankylosing spondylitis (AS), the prototype of this group, mainly because of the requirement of radiographic sacroiliitis for its diagnosis2. Low awareness of inflammatory back pain (IBP), the first and most common symptom of spondyloarthritis (SpA), in daily practice is also a major reason for the diagnostic delay3. New classification criteria developed by the Assessment of SpondyloArthritis International Society (ASAS) provide that patients with SpA can be classified as either patients with axial SpA (axSpA) or those with peripheral SpA. The ASAS axSpA criteria cover the entire spectrum of axial disease including AS and nonradiographic axSpA (nr-axSpA)4. Early diagnosis of axSpA can create an opportunity for better treatment strategies.
The number of epidemiological studies regarding IBP5,6,7,8 and axSpA9 is limited. In a review of the literature, we found no population-based study that investigated their prevalence using the new ASAS classification criteria. We sought to determine the prevalence of IBP and axSpA using these criteria among university employees in Izmir, Turkey.
MATERIALS AND METHODS
We conducted our study at the Health Sciences Campus at Dokuz Eylul University in Izmir, which has 2894 medical and nonmedical staff aged between 18 and 67 years. A sample of 395 subjects was selected randomly by a computer from the list of all employees, based on the IBP prevalence of 5% in the general population5, using OpenEpi (version 2.3) and CI ± 2%. A total of 381 of these 395 subjects agreed to participate, an acceptance rate of 96.5%. In the first stage of the study, 6 trained medical students, using a standard questionnaire, interviewed participants face to face. Questionnaire responses were used to determine whether participants met the ASAS criteria for IBP10. Subjects were also evaluated for IBP based on the Berlin11 and Calin criteria12 (Table 1).
Inflammatory back pain criteria sets.
In the second stage, the subjects with back pain for more than 3 months and symptom onset before age 45 years were invited to the rheumatology outpatient clinic to participate in the study. Subjects who accepted the invitation were evaluated for axSpA by 2 rheumatologists using the ASAS classification criteria4. Pelvic radiographs and magnetic resonance imaging (MRI) of the sacroiliac joint (SIJ) were obtained. They were read by an experienced rheumatologist and a radiologist blinded to the patients’ identities. The patients with at least 2 features of SpA and negative imaging or who had no SIJ imaging were tested for HLA-B27.
The subjects were also evaluated to determine whether they met the modified New York (mNY) criteria for AS13 and both the European Spondyloarthropathy Study Group (ESSG) criteria14 and Amor criteria15 for SpA.
Ethics approval for our study was obtained from the Local Research Ethics Committee (22 March 2012/11-15).
Statistical analysis
Stats Direct Statistical Software (version 3.0.23, Stats Direct Ltd.) was used for calculating the prevalence and 95% CI.
RESULTS
In the first stage of our study, among the 395 subjects who had been contacted, 381 (131 men, 250 women; mean age: 38.1 ± 9.5 yrs) had agreed to take part; an acceptance rate of 96.5%. Among them, 299 (78.5%; 95% CI 69.8–87.9) had experienced back pain at least once in their lifetime. A total of 172 subjects (45.1%; 95% CI 38.7–52.4) had back pain lasting more than a month and 127 (33.3%; 95% CI 27.8–39.7) more than 3 months.
Among 381 subjects, 25 (6.6%; 95% CI 4.3–9.7) were classified as having IBP according to ASAS criteria10. The prevalence of IBP according to Berlin11 and Calin criteria12 was found to be 7.1% (95% CI 4.7–10.3) and 21.5% (95% CI 17.1–26.7), respectively (Table 2). The prevalence of IBP according to the ASAS criteria was 8.4% (95% CI 5.4–12.3) among all patients with back pain. It was estimated to be 14.5% (95% CI 9.4–21.5) and 19.7% (95% CI 12.7–29.0) among those with chronic back pain lasting more than 1 month and 3 months, respectively.
Prevalence of inflammatory back pain and axial spondyloarthritis/spondyloarthritis according to various classification criteria among university employees.
The prevalence of IBP in women (8.0%; 95% CI 4.9–12.4) was found to be higher than that in men (3.8%; 95% CI 1.2–8.9), according to the ASAS criteria. IBP was also more prevalent among women than men according to other IBP criteria sets (Table 2).
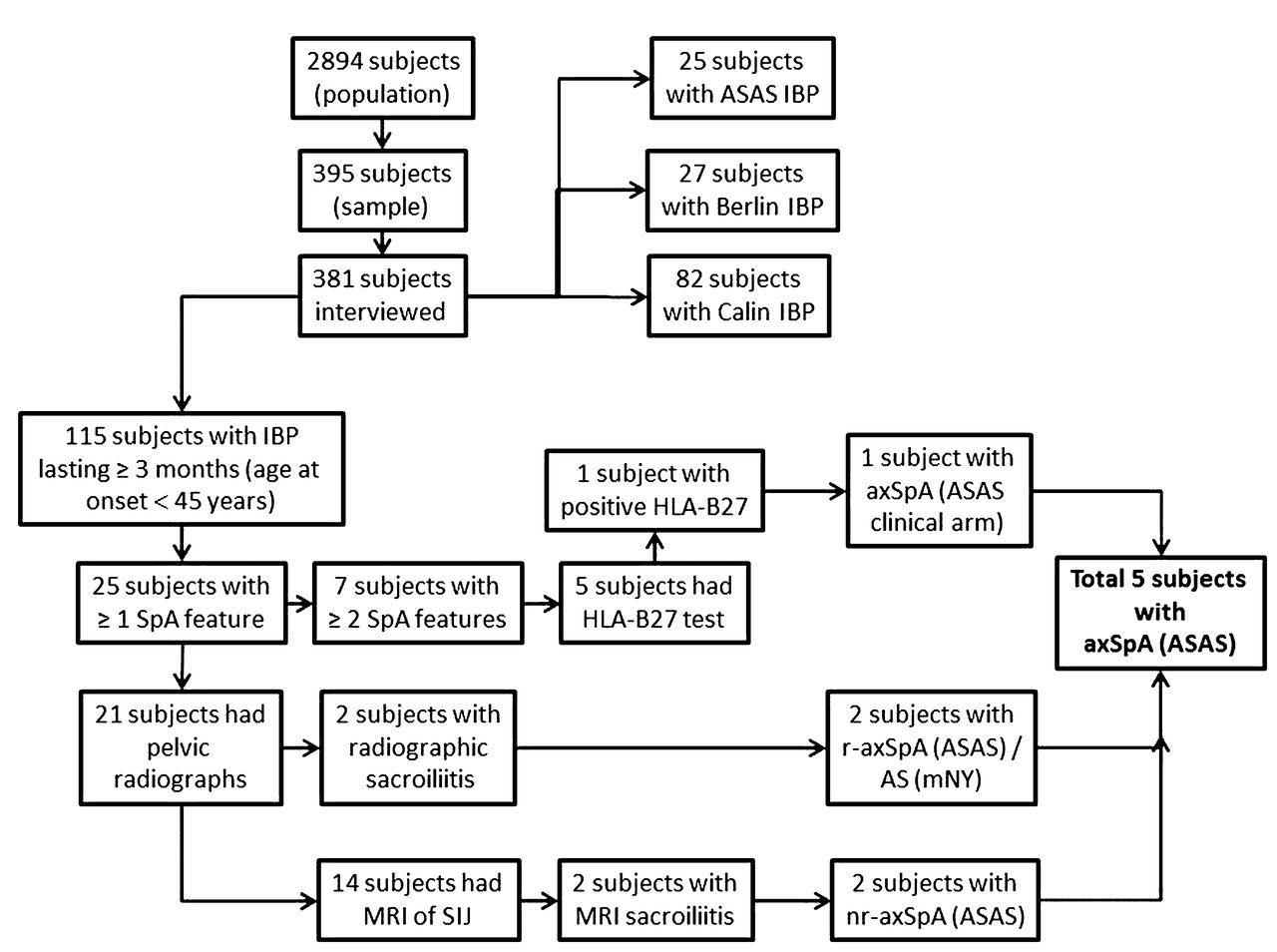
There were 115 patients (30%) with back pain for more than 3 months and symptom onset before the age of 45 years. They were invited to undergo further clinical evaluation at the rheumatology outpatient clinic, and 95 (82.6%) agreed to do so. Twenty-five of them had at least 1 SpA feature. All these patients had IBP based on the ASAS criteria and 7 of them had other SpA features (6 gluteal pain, 3 enthesitis, 1 psoriasis, 1 peripheral arthritis, and 1 dactylitis; Figure 1).

Study design and results in each stage. IBP: inflammatory back pain; ASAS: Assessment of SpondyloArthritis International Society; SpA: spondyloarthritis; axSpA: axial SpA; r-axSpA: radiographic axSpA; SIJ: sacroiliac joint; MRI: magnetic resonance imaging; AS: ankylosing spondylitis; mNY: modified New York criteria; nr-axSpA: nonradiographic axSpA.
Pelvic radiographs were obtained in 21/25 patients with at least 1 SpA feature. Two of them demonstrated bilateral grade 3 sacroiliitis. In 14 out of 19 patients with normal radiographs, MRI of SIJ could be performed. Two of these patients demonstrated signs of acute sacroiliitis (Figure 1).
There were 7 patients with chronic back pain and at least 2 SpA features. One of them had MRI sacroiliitis. Among the remaining 6 patients, SIJ imaging was not available for 3 and the other 3 had negative MRI of SIJ. Five of the 7 patients with chronic back pain and at least 2 SpA features could be tested for HLA-B27 and 1 of them was found to be positive. This patient was classified as nr-axSpA according to the clinical arm of the ASAS criteria (Figure 1).
In total, 5 subjects (1.3%) with at least 1 SpA feature (all had IBP) were classified as having axSpA according to the ASAS classification criteria4. Two of them (0.5%) had radiographic sacroiliitis and met the mNY criteria for AS13. The prevalence of nr-axSpA was estimated to be 0.8%. There were 7 patients (1.8%) who fulfilled both the Amor15 and ESSG criteria14 for the whole group of SpA (Table 2). One of them had psoriasis and met the ClASsification for Psoriatic ARthritis (CASPAR) criteria16 for psoriatic arthritis (Figure 1).
We found the prevalence of axSpA to be 1.5% in men and 1.2% in women. The prevalence of r-axSpA was higher in men than in women (0.8% vs 0.4%), but nr-axSpA was found to be slightly more prevalent in women than in men (0.80% vs 0.76%). The prevalence of SpA based on the Amor and ESSG criteria among women and men was 2.0% and 1.5%, respectively (Table 2).
Two patients were newly diagnosed as having nr-axSpA and 1 as having r-axSpA (AS) during the study period. Previously, they had been diagnosed by a nonrheumatologist with lumbar disc hernia (LDH).
DISCUSSION
Our epidemiological study estimated a prevalence of 6.6% for IBP based on the ASAS criteria among the health campus employees of a university in Izmir, a major city in Turkey. The only previous study using the ASAS criteria for IBP6 estimated a slightly higher prevalence of IBP (7.7%) among a primary care patient population in the United Kingdom. In that study, the prevalence was 15.4% by the Berlin criteria, which was also higher than the prevalence of 7.1% using the same criteria in our study6. The higher results in the UK survey may be related to the study population including subjects with previous back pain history. On the other hand, the higher prevalence for IBP by the Calin criteria in the 2 studies could be due to a higher sensitivity and lower specificity of these criteria compared to the others17. The reported IBP prevalence in different studies may also vary according to geographic and genetic factors as well as criteria used and other methodological differences. A study based on the COPCORD (Community Oriented Program for the Control of Rheumatic Diseases) in the Mexican population7 and a retrospective analysis of data from the National Health and Nutrition Examination Survey (NHANES) II (1971–1975) in the United States8 estimated significantly lower IBP prevalences of 3% and 0.8%, respectively. No standardized criteria sets to define IBP were used in these studies but the 2009–2010 NHANES survey used a data collection instrument specifically designed for IBP. In the latter survey, the age-adjusted prevalence of IBP was found to be 5.0% by Calin criteria among US adults. The IBP prevalence was 5.6% based on the ESSG criteria, and 5.8% and 6.0% based on the Berlin Criteria 8a and 7b, respectively5.
IBP was found to be about twice as prevalent among women than men in our study. The NHANES (2009–2010)5 and UK studies6 also reported somewhat higher frequencies in women than in men although the differences were not significant.
We estimated a prevalence of 1.3% for axSpA in the second stage of the study. More than half the patients with axSpA were found to have nr-axSpA with the prevalence of 0.8%. The only previous study9 using the ASAS classification criteria estimated the prevalence of axSpA in the United States at 0.7%, which was lower than what we found. However, that was a retrospective cohort study and the diagnosis of axSpA was established on identification of elements of the ASAS criteria in medical records of at-risk patients treated by a representative sample of US rheumatologists. Thus, this may have led to underestimation of the prevalence of axSpA. In that study, the prevalence estimates of AS and nr-axSpA were 0.35% and 0.35%, respectively9. Our previous study among adults in an urban area of Izmir demonstrated a prevalence of 0.5% for AS based on the mNY criteria18. In our current study, we estimated the same prevalence for AS (mNY)/r-axSpA (ASAS).
The major disadvantage of the mNY criteria, the most commonly used criteria in epidemiological studies, is the requirement of radiographic sacroiliitis of at least grade 2 bilaterally or grade 3 unilaterally for the classification of AS13. Therefore, a diagnostic delay up to 10 years is commonly seen in AS, due to slow progression of radiographic damage19. Further, the mNY criteria focus on axial involvement, and other important SpA features such as extraspinal and extraarticular findings, family history, and response to nonsteroidal antiinflammatory drugs are not included13. The new ASAS axSpA criteria include MRI as a sensitive method for detection of inflammation in the sacroiliac joints, which is not well demonstrated by plain radiographs. They also include HLA-B27 testing when imaging was not performed. Therefore, these criteria allow for the identification of nr-axSpA. ASAS criteria have been demonstrated to be sensitive (82.9%) and specific (84.4%) for the classification of axSpA4.
Our current study confirmed that SpA was one of the most common forms of inflammatory rheumatic diseases in the general white population1. The prevalence of SpA by both the ESSG and Amor criteria was estimated to be 1.8%, which was higher than that in the previous general population study in Izmir (a prevalence of 1.05% by the ESSG criteria)18.
The previous survey in the Turkish general population showed that AS affected men more frequently than women, but the rate of SpA, as a whole group, was slightly higher in women18. In our current study, these findings were confirmed. The prevalence of r-axSpA (AS) in men was established to be about twice as high as in women and the whole group of SpA was slightly more prevalent in women than men, with a ratio of 1.33. This study also showed that the prevalence of nr-axSpA was similar among women and men. There were no other population-based studies that compared the prevalence of nr-axSpA between men and women. Results from the German Spondyloarthritis Inception Cohort (GESPIC)19, which included patients with axSpA, demonstrated that AS was more prevalent in men; however, nr-axSpA was characterized by a higher prevalence among women. More recently, data from GESPIC were confirmed in the Herne20 and Swiss Clinical Quality Management21 cohorts, which included patients with r-axSpA and nr-axSpA. These results are in line with the well-known finding that male patients with AS have more severe radiographic changes22.
There were 3 patients who were newly diagnosed as having axSpA during this study period. One of them had r-axSpA. Although all these patients had IBP, previously they had been diagnosed by a nonrheumatologist with LDH. This result is consistent with that found in our previous study, which showed that an initial diagnosis of LDH is associated with a later diagnosis of AS3.
Our study suggests that axSpA is a more prevalent rheumatic disease than previously thought. Awareness of IBP and other symptoms of SpA in clinical practice may provide a chance for early diagnosis and treatment. The new ASAS criteria for axSpA that include MRI of SIJ and HLA-B27 testing may help to better classify patients with nr-axSpA.
Acknowledgment
We thank the third-year medical students of the Special Study Module Group of Dokuz Eylul University School of Medicine for their assistance with this study.
- Accepted for publication May 27, 2015.








{kind=link}