

Abstract
Objective. To describe the expression and diagnostic use of 14-3-3η autoantibodies in early rheumatoid arthritis (RA).
Methods. 14-3-3η autoantibody levels were measured using an electrochemiluminescent multiplexed assay in 500 subjects (114 disease-modifying antirheumatic drug-naive patients with early RA, 135 with established RA, 55 healthy, 70 autoimmune, and 126 other non-RA arthropathy controls). 14-3-3η protein levels were determined in an earlier analysis. Two-tailed Student t tests and Mann-Whitney U tests compared differences among groups. Receiver-operator characteristic (ROC) curves were generated and diagnostic performance was estimated by area under the curve (AUC), as well as specificity, sensitivity, and likelihood ratios (LR) for optimal cutoffs.
Results. Median serum 14-3-3η autoantibody concentrations were significantly higher (p < 0.0001) in patients with early RA (525 U/ml) when compared with healthy controls (235 U/ml), disease controls (274 U/ml), autoimmune disease controls (274 U/ml), patients with osteoarthritis (259 U/ml), and all controls (265 U/ml). ROC curve analysis comparing early RA with healthy controls demonstrated a significant (p < 0.0001) AUC of 0.90 (95% CI 0.85–0.95). At an optimal cutoff of ≥ 380 U/ml, the ROC curve yielded a sensitivity of 73%, a specificity of 91%, and a positive LR of 8.0. Adding 14-3-3η autoantibodies to 14-3-3η protein positivity enhanced the identification of patients with early RA from 59% to 90%; addition of 14-3-3η autoantibodies to anticitrullinated protein antibodies (ACPA) and/or rheumatoid factor (RF) increased identification from 72% to 92%. Seventy-two percent of RF- and ACPA-seronegative patients were positive for 14-3-3η autoantibodies.
Conclusion. 14-3-3η autoantibodies, alone and in combination with the 14-3-3η protein, RF, and/or ACPA identified most patients with early RA.
Abnormal autoantibody production before clinically apparent inflammatory events associated with rheumatoid arthritis (RA) has been termed “preclinical RA.” Rheumatoid factor (RF) and anticitrullinated peptide antibodies (ACPA) are well-studied autoantibodies that are elevated in preclinical and clinical RA1,2,3,4,5,6,7,8,9,10. These autoantibodies can have substantial prognostic use, as demonstrated in a Dutch cohort of patients with arthralgia and stiffness, but without clinically apparent synovitis at their baseline examination11. After 2 years of followup, ACPA-positive patients were more likely to develop RA, and this risk was increased by higher levels of ACPA and the concomitant presence of immunoglobulin M (IgM)-RF. Similarly, Rantapää-Dahlqvist, et al found that ACPA and IgA-RF predicted the development of RA in blood donors9.
In 2007, we reported that the soluble biomarker 14-3-3η protein, an intracellular chaperone, was present at significantly higher levels in the synovial fluid (SF) and serum of patients with arthritis compared with healthy individuals12. Serum 14-3-3η protein levels also correlated strongly with the SF and serum levels of the matrix metalloproteinases MMP-1 and MMP-3. More recently, we have demonstrated that the serum 14-3-3η protein was present at significantly higher levels in patients with erosive RA13, that it was highly specific for RA, and that it was complementary to RF and ACPA for RA diagnostic sensitivity14. In vitro results demonstrated that soluble 14-3-3η protein, at clinically relevant concentrations, possessed ligand-like properties activating intracellular signal transduction cascades, such as the extracellular signal-regulated kinases and Janus kinase/stress-activated protein kinases. Activation of these pathways resulted in the convergence of signals within the nucleus and the corresponding upregulation of proinflammatory cytokines, such as interleukin (IL)-1β, IL-6, and tumor necrosis factor-α, and factors that were involved in joint degradation, such as MMP-9 and receptor activator of nuclear factor-κB ligand (RANKL)13.
The family of conserved 14-3-3 regulatory proteins consists of 7 isoforms: β, ɛ, γ, η, τ, ζ, and σ. Under normal physiological circumstances, these proteins exist as intracellular chaperonins that can either homo- or heterodimerize to form a cup-like structure known as the “amphipathic groove” that allows them to interact with more than 200 intracellular proteins to modulate their activities. Interactions include an array of biological processes, such as protein trafficking and cellular signaling. Externalization of the 14-3-3η protein, as observed in RA, is thought to be mediated in part through an exosomal process in a manner similar to other intracellular proteins4,6.
When the 14-3-3η protein is externalized, it is seen by the immune system as being foreign, which results in the development of a 14-3-3η autoantibody response. The role of these autoantibodies to 14-3-3η in inflammatory disease is unknown. The purpose of this investigation was to establish whether measurement of 14-3-3η autoantibodies has diagnostic use in RA and whether these autoantibodies provide additional diagnostic information to RF, ACPA, or the 14-3-3η protein for the identification of RA.
MATERIALS AND METHODS
Patients with RA and controls
Demographics and clinical characteristics for all study participants, as well as clinical characteristics of the early and established RA cohorts, are provided in Table 1. 14-3-3η autoantibody levels were measured in 500 subjects using banked samples from 114 disease-modifying antirheumatic drug (DMARD)–naive patients with early RA, 135 patients with established RA, and 251 controls, including 55 healthy individuals, 126 with other arthropathies, and 70 with other inflammatory and autoimmune disorders. Serological measurements for ACPA, RF, and the 14-3-3η protein were previously measured in these populations, as described in Maksymowych, et al14. Briefly, the 14-3-3η protein measurements were done using the quantitative 14-3-3η ELISA (Augurex life Sciences Corp.). RF and ACPA assays were performed as per manufacturers’ protocols (RF by Quanta Lite IgM ELISA, ACPA by Quanta Lite CCP3 IgG ELISA).
Patient and control demographics and serology. Superscripts denote the number of patients used in the analysis when values were not available for all patients.
The 114 patients with early RA were classified according to the American College of Rheumatology (ACR) 1987 criteria and were a mean (SD) of 53 (11) years old with 86 being women (75%). Patients with early RA were obtained from the Sherbrooke Early Undifferentiated PolyArthritis (EUPA) cohort (n = 40), the Intensified-Combination Therapy with Rheumatoid Arthritis cohort (COBRA; VU University Medical Center, Netherlands, n = 12), and the Reade prospective early RA cohort (Reade, Netherlands, n = 62). All patients with early RA were naive to DMARD therapy. In the EUPA cohort, adult patients with synovitis affecting at least 3 joints for 1–12 months were followed longitudinally, as described previously15. The median [interquartile range (IQR)] disease duration was 1.8 months (1.5–3.0), and the median (IQR) Disease Activity Score at 28 joints (DAS28) was 5.9 (4.8–6.5). The intensified COBRA study was a pilot trial assessing tight control strategies; sera were taken at baseline from a subset of patients with median (IQR) disease duration of 1.0 months (1.0–2.0)16. The Reade prospective early RA cohort recruited patients aged ≥ 18 years, with at least 2 swollen joints and symptom duration of < 2 years with median (IQR) disease duration of 4.2 months (2.9–3.7)17. Sera were available for the 62 patients from the Reade prospective early RA cohort at baseline and 1 year following baseline. The patients from the Reade cohort were receiving standard DMARD therapies within a year of first assessment.
ANOVA revealed no significant differences in 14-3-3η autoantibody levels between the 3 early RA groups; consequently, they were combined for all analyses.
The 135 patients with established RA were previously described in Maksymowych, et al14 and were classified according to the ACR 1987 criteria. These patients were taking standard DMARD therapy, but were naive to biological therapy. For comparison to the RA groups, a total of 251 controls were assessed: 55 presumed healthy subjects from BioChemed LLC, 126 non-RA arthropathy patients [67 patients with ankylosing spondylitis (AS) from the University of Alberta, classified according to the modified New York Criteria; 30 patients with osteoarthritis (OA) from Mount Sinai Hospital, Toronto, Ontario, Canada; 24 patients with psoriatic arthritis (PsA) from the Academic Medical Center, the Netherlands; and 5 patients with gout from Bioreclamation IVT], 25 patients with connective tissue disorders from Bioreclamation IVT (10 patients with systemic lupus erythematosus, 5 with systemic sclerosis, 5 with Sjögren syndrome, and 5 with osteoporosis), and 45 patients with various inflammatory/autoimmune diseases from Bioreclamation IVT [10 patients with Crohn disease, 10 patients with ulcerative colitis, 10 patients with psoriasis, 10 patients with Type 1 diabetes (DB Type 1), and 5 patients with multiple sclerosis]. The attending physician confirmed diagnoses of disease controls.
The study was performed in accordance with the Helsinki Declaration. Written informed consent was obtained from all study participants and ethics approval was obtained from the Health Research Ethics Board of the University of Alberta, the Ethics Review Board of Centre Hospitalier Universitaire de Sherbrooke, the Ethical Review Board of VU University of Amsterdam Medical Center and the Jan van Breemen Institute, and the Mount Sinai Health Ethics Review Board of the University of Toronto.
Serum 14-3-3η autoantibody measurements
Serum 14-3-3η autoantibody levels were measured using the 10-spot multiplexed semiquantitative 14-3-3η autoantibody assay (Augurex Life Sciences Corp.). Ten distinct peptides were spotted at specific locations within each well with the MesoScale Discovery (MSD) reader reporting an individual value for each spot. Serum samples were diluted 1:100 using a proprietary assay buffer containing detergents, salts, and protein. One hundred µl of diluted serum sample was plated on a multispot 96-well plate for 15 min at room temperature without shaking. Following incubation, the plates were washed 4 consecutive times with a phosphate buffer with detergent (wash buffer) and then incubated with freshly diluted conjugate antibody (specificity to IgG, Fcγ Fragment specific) for 15 min at room temperature without shaking. The plates were washed twice with wash buffer and twice with phosphate buffer naive of detergent. A read buffer with surfactant (MesoScale Discovery LLC) was added to the plate and the plates were read using the MSD electrochemiluminescent sector imager. Six of the 10 peptides were prioritized based on receiver-operator characteristic (ROC) curve analysis comparing early RA with healthy subjects and disease controls (described previously) and based on complementarity to each other for RA diagnosis. A cumulative score was generated through the simple addition of the individual values for peptides 1, 2, 4, 7, 9, and 10. The cumulative score is equal to:

Statistical methods
Descriptive statistics were used to express clinical and serological measurements according to disease category and healthy controls. To compare more than 2 groups, the Kruskal-Wallis test with the posthoc Dunn Multiple Comparison method was used to determine whether significant differences existed between groups in levels of the 14-3-3η autoantibodies. Mean and median 14-3-3η autoantibody levels between the RA and control groups were tested for statistically significant differences using the 2-tailed Student t test and the Mann-Whitney U test. ROC curves were used to evaluate the diagnostic performance of 14-3-3η autoantibodies as estimated by the area under the curve (AUC), the corresponding likelihood ratios (LR) at various 14-3-3η autoantibody cutoffs, and the corresponding positive (PPV) and negative predictive values (NPV). The additional diagnostic value added by the inclusion of 14-3-3η autoantibodies was assessed in early and established RA (in addition to RF, ACPA, 14-3-3η protein alone and together with the autoantibodies). An incremental benefit/change was calculated as follows:

The relationship between 14-3-3η autoantibodies and other serological markers was assessed using the Spearman rank correlation coefficient procedure for non-normally distributed data and Pearson product-moment correlation for normally distributed variables. Distribution normality was established by the Shapiro-Wilk normality test. The Wilcoxon matched-pairs signed rank test was used to assess significant changes in autoantibody levels over time.
All statistical analyses were completed with Prism 6 (GraphPad Software Inc.) or JMP11 (SAS Institute Inc.). Statistical significance was denoted by an α of p < 0.05.
RESULTS
Expression of 14-3-3η autoantibodies in early RA
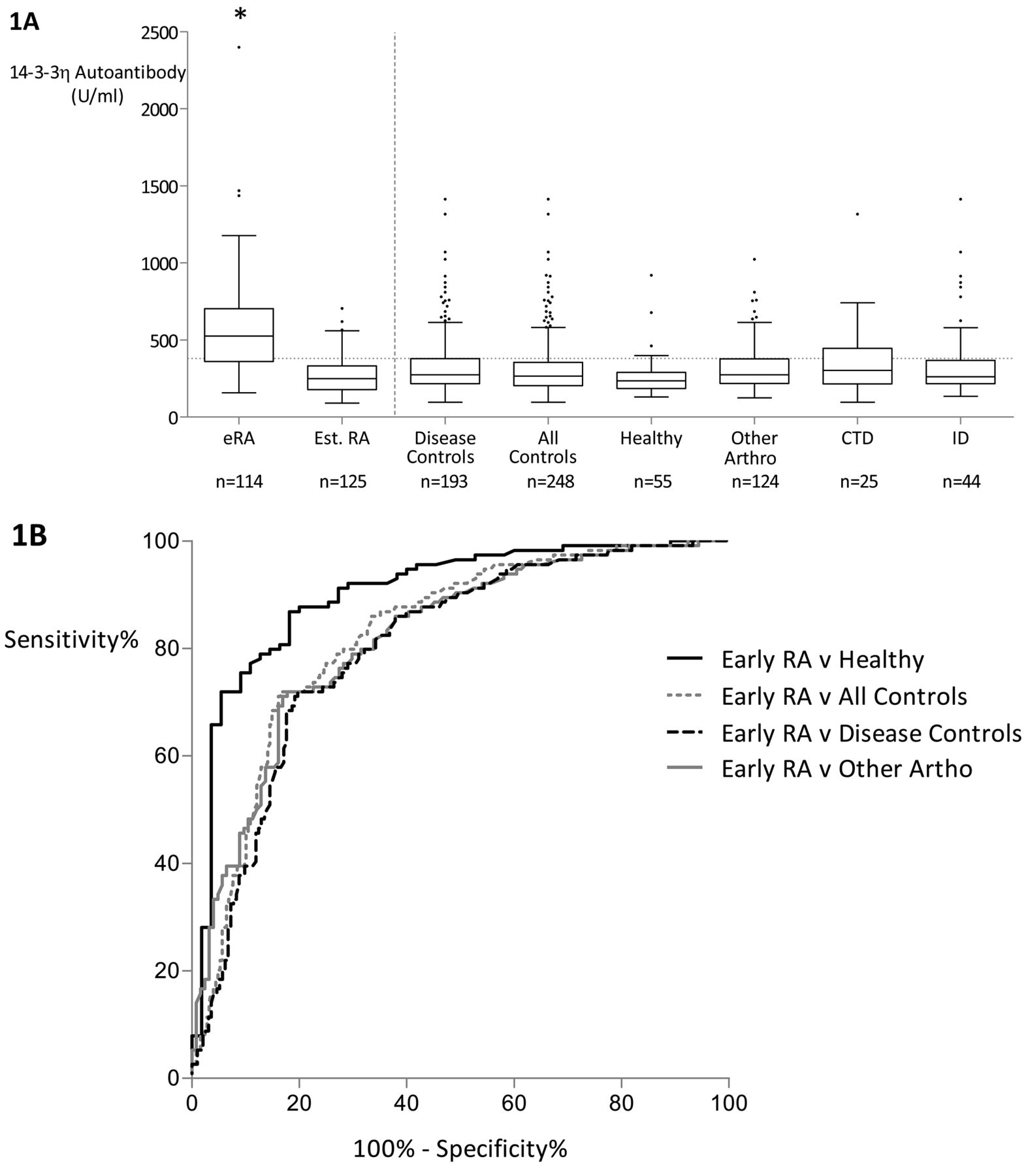
As presented in Figure 1A, median serum 14-3-3η autoantibody concentrations were significantly higher (p < 0.0001) in patients with early RA (525 U/ml) when compared with healthy controls (235 U/ml), connective tissue and inflammatory disease controls (274 U/ml), other non-RA inflammatory arthropathies (274 U/ml), patients with OA (259 U/ml), and all controls (265 U/ml).

A. Serum 14-3-3η autoantibody expression in established and early RA versus combined control cohorts. B. Corresponding ROC curve for early RA versus controls. *Median eRA 14-3-3η autoantibody levels are significantly higher compared with all other cohorts assessed. Median Est. RA 14-3-3η autoantibody levels are not significantly different from the other cohorts assessed. 14-3-3η autoantibody positivity cutoff was established as ≥ 380 U/ml (shown as dashed line across groups). RA: rheumatoid arthritis; eRA: early RA; Est. RA: established RA; Other Arthro: other arthropathies; CTD: connective tissue disorders; ID: inflammatory diseases; ROC: receiver-operator characteristic.
ROC curve analysis comparing early RA with healthy controls demonstrated a significant (p < 0.0001) AUC of 0.90 (95% CI 0.85–0.95). At an optimal cutoff of ≥ 380 U/ml, the ROC curve yielded a sensitivity of 73%, a specificity of 91%, an LR positive of 8.0, a PPV of 0.94, and an NPV of 0.62. At this same cutoff (≥ 380 U/ml), when comparing early RA with all controls, the ROC curve yielded a sensitivity of 73%, a specificity of 79%, an LR positive of 3.5, a PPV of 0.61, and an NPV of 0.86 (Figure 1B, Table 2). Similar discrimination was observed when early RA was compared with disease or patients with other non-RA arthropathies.
Results of ROC curve analyses for 14-3-3η autoantibody scores for early RA versus control cohorts.
Specificity of 14-3-3η autoantibodies for established RA
Median (IQR) 14-3-3η autoantibody levels in patients with established RA (249, 179–332 U/ml) were significantly lower when compared with patients with early RA (525, 360–704 U/ml, p < 0.0001; Figure 1A, Table 1). 14-3-3η autoantibody levels did not discriminate established RA from healthy individuals or any other disease control group.
Associations of 14-3-3η autoantibodies with disease cohorts
There was a significant difference in 14-3-3η autoantibody expression between healthy and disease controls, and upon further investigation, it was determined that this difference in expression resided entirely between healthy individuals and patients with AS: median (IQR) 14-3-3η autoantibodies were modestly but significantly higher (p = 0.0001) in patients with AS [309 U/ml (238–405)] compared with healthy controls [235 U/ml (185–289)].
Associations of 14-3-3η autoantibodies and clinical measures
The correlation matrix presented in Table 3 illustrates the relationship between 14-3-3η autoantibody levels and clinical/serological variables in the early RA cohort. The only significant correlation was with the erythrocyte sedimentation rate, where a weak correlation was observed (r = 0.27, p < 0.01). Moreover, unlike the 14-3-3η protein, no significant correlation was observed with RF or ACPA, or between levels of the 14-3-3η protein and 14-3-3η autoantibodies.
Correlation coefficients of 14-3-3η protein and antibodies with clinical and serological measures in patients with early RA. Correlation between age and HAQ was established with a Pearson product-moment correlation as both variables were normally distributed according to Shapiro-Wilk normality testing; all other correlations are Spearman rank correlation.
Incremental diagnostic use of 14-3-3η autoantibodies
Because ACPA and RF are routinely used together to inform an RA diagnosis18, the incremental benefit of adding 14-3-3η autoantibodies to these markers was assessed. As illustrated in Table 4, of the 113 patients with early RA assessed, 61%, 63%, 59%, and 73% were positive for ACPA, RF, 14-3-3η protein, and 14-3-3η autoantibodies, respectively. Eighty-one (72%) were RF- and/or ACPA-positive, and so 32 (28%) were seronegative according to current clinical designation. Notably, 23 (72%) of the 32 seronegative patients were positive for 14-3-3η autoantibodies. Adding 14-3-3η autoantibodies to positive ACPA and/or RF status enhanced identification of early RA to 92% and reduced the category designated as seronegative to 8%. Combining positive status for either 14-3-3η protein and/or its autoantibodies identified 90% of the patients with early RA. Positivity for any 1 of the 4 markers (RF, ACPA, 14-3-3η, 14-3-3η autoantibodies) identified 94% of patients with early RA and reduced the category designated as seronegative to 6%.
Complementarity between diagnostic markers (RF, ACPA, 14-3-3η protein, and 14-3-3η antibodies) in patients with early RA. Levels of all 4 markers were available in 113 patients with early RA and 121 patients with established RA. Serum level of ≥ 0.19 ng/ml is defined as positive for 14-3-3η and ≥ 380 U/ml is defined as positive for 14-3-3η AAb. Values are n (%) unless otherwise specified.
The proportion of patients with established RA who were positive for 14-3-3η autoantibodies was much lower, at 15%. Positivity for RF and/or ACPA was much higher (88%) than in early RA, and the addition of 14-3-3η autoantibodies did not provide substantial incremental benefit (1%).
The sensitivity and specificity of RF, ACPA, and RF and/or ACPA with and without 14-3-3η autoantibodies in patients with early RA is presented in Table 5. In all comparisons, the addition of 14-3-3η autoantibodies led to notable increases in sensitivity without substantial loss of specificity. When comparing combined RF and ACPA to the combined 14-3-3η protein and 14-3-3 autoantibodies, there were substantial increases in sensitivity with the 14-3-3η markers, with only a modest decrease in specificity. In the early RA cohort, the sensitivity and corresponding specificity of the combination of RF and/or ACPA positivity when compared with healthy subjects was 0.72/0.87. The combination of the 14-3-3η protein and its autoantibodies delivered a sensitivity of 0.90 with a specificity of 0.82.
Sensitivity, specificity, and LR for RF, ACPA, and 14-3-3η and combinations without and with inclusion of 14-3-3η.
Expression of 14-3-3η autoantibodies at followup timepoints
The 14-3-3η autoantibody levels were significantly lower at the 1-year followup timepoint compared with baseline values (384 U/ml vs 572 U/ml, p = 0.0007). Of the 62 patients with early RA, 42 (68%) were positive for 14-3-3η autoantibodies at baseline whereas only 23 (37%) were positive after 1 year. Of the positive patients at baseline, 20 (48%) remained positive at 1 year with 22 patients (52%) having a decrease in 14-3-3η autoantibody levels below the positive cutoff of ≥ 380 U/ml. Three patients (15%) who were negative at baseline sero-converted to positive at 1 year, and 17 patients (85%) remained negative.
DISCUSSION
To our knowledge, our study is the first report describing the diagnostic use of autoantibodies directed toward the native form of the 14-3-3η protein in early RA that augments the diagnostic detection rate of existing biomarkers, including the 14-3-3η protein. Moreover, the lack of correlation noted between the presence of these autoantibodies and the 14-3-3η protein, ACPA, RF, and acute-phase reactants underscores the unique information provided by the 14-3-3η autoantibodies. The 14-3-3η autoantibodies together with the 14-3-3η protein, ACPA, and RF is of clinical relevance because their combination appears to identify almost all patients with early RA, raising the question as to whether seronegative RA exists. Future studies will focus on determining how the 14-3-3η autoantibodies work together with clinical signs and symptoms to inform RA before there are visible signs of radiographic progression by radiography. Prospective Year 1 longitudinal data from patients with early RA presented here suggest that 14-3-3η autoantibodies decrease over the course of disease, which aligns with the cross-sectional data from patients with established RA, in which 14-3-3η autoantibody expression does not differ from the control groups assessed.
We have previously reported that serum 14-3-3η protein has diagnostic use in patients with RA and that the 14-3-3η protein, as a soluble ligand, activates signaling pathways leading to the upregulation of proinflammatory cytokines, metalloproteinases, and RANKL13. It is thought that extracellular secretion of 14-3-3η may, in part, be an exosomal-mediated process, although what triggers its release is presently unknown. Synovial fluid 14-3-3η protein expression is much higher than what is measured in peripheral blood, indicating its local production and expression. In a recently published study, we described that 14-3-3η levels were even higher in patients with radiographic progression in both RA and PsA, which is consistent with transformation of fibroblasts to an activated phenotype13. Fibroblast exosomes are thought to be a major source of 14-3-3η4,6.
In contrast to RF and ACPA, the results from our study demonstrate that 14-3-3η autoantibodies are significantly lower at Year 1 in comparison to the corresponding baseline measurement. This decrease in 14-3-3η autoantibodies over time as the disease progresses may be reflective of immune tolerance to the 14-3-3η protein or as a consequence of treatment with DMARD. Preliminary results indicate that these autoantibodies might elicit a protective effect in that patients with RA who are positive for 14-3-3η autoantibodies but negative for the 14-3-3η protein have a higher likelihood of achieving DAS28 remission and are also less likely to progress radiographically19. It is therefore possible that these autoantibodies have a role in the clearance of the 14-3-3η protein and that excess production/secretion of the 14-3-3η protein or evasion of clearance through posttranslational modification of the 14-3-3η autoantibodies, through processes such as glycosylation20,21, may constitute an adverse prognostic factor22. Preliminary data in a collagen-induced arthritis model supports this hypothesis. All animals developed autoantibodies to the 14-3-3η protein; however, those animals in which levels of the 14-3-3η protein persisted at high levels were more likely to develop arthritic symptoms23. This hypothesis is further reinforced by the fact that the 6 different epitope specificities assessed in the composite autoantibody score reflected epitopes that were located in the ligand-binding groove of the 14-3-3η protein. These autoantibodies might, therefore, be expected to decrease the interaction between the 14-3-3η protein and its ligand(s). The latter remains to be identified, but the downstream effects of this interaction include the expression of proinflammatory cytokines, metalloproteinases, and RANKL. Further investigation is aimed at identifying the primary specificities associated with diagnostic and prognostic properties of these autoantibodies.
There are several examples of metabolic and autoimmune disorders wherein autoantibodies develop early in the disease course and levels may either be sustained throughout the course of disease or decline with disease progression. An example of the latter is autoantibodies to the islet-specific zinc transport isoform (ZnT8), a test that was approved by the US Food and Drug Administration as a diagnostic marker for DB Type 1. ZnT8 autoantibodies are present in the prediabetic state and have been shown to increase at the time of disease onset, yet decline over time as the disease progresses24. The role that these autoantibodies play in the pathogenesis of the DB Type 1 is yet to be established. It is postulated that certain autoantibodies have a proinflammatory effect while others are antiinflammatory in nature and decline over time as the disease progresses.
We present the first data, to our knowledge, indicating that 14-3-3η, a novel proinflammatory mediator associated with the pathophysiology of joint inflammation in RA, generates an autoantibody response to the native protein. The combination of the 14-3-3η markers (i.e., protein and autoantibodies) independently provides high sensitivity and specificity for early RA as a novel biomarker panel and further augments the diagnostic detection rate of RF and ACPA. Consistent with the focus on identifying patients with RA as early as possible, the 14-3-3η markers provide a means to investigate patients at risk for RA and those with new onset disease. A 14-3-3η autoantibody composite score reflecting 6 different epitope specificities has discriminatory properties for early RA and enhances the diagnostic contribution of existing biomarkers. Expression of antibodies does not correlate with acute-phase reactants or other clinical variables of disease severity, indicating that these antibodies contribute unique information for RA management. Future studies will focus on examining the role of the 14-3-3η autoantibodies in the pathogenesis of RA and validating these findings in prospective cohorts.
Acknowledgment
We thank Dr. K. Shawn Davison for his assistance in the preparation of this manuscript.
Footnotes
This investigation was solely funded by Augurex Life Sciences Corp., North Vancouver, British Columbia, Canada.
- Accepted for publication May 14, 2015.








{kind=link}