

Gout can occur in an unusual location without hyperuricemia and with heterogeneous T1 and T2 hyposignal.
A 44-year-old male patient consulted for an isolated and firm swelling of the pretragal region. A 72-year-old female patient presented with left pretragal tenderness and limited mouth opening. Both patients presented with multiple temporomandibular joint (TMJ) calcifications on computed tomography (CT), and heterogeneous T1 and T2 hyposignal TMJ lesions on magnetic resonance imaging (MRI; Figure 1 and Figure 2). Fine needle aspiration was performed for the first patient, but was not conclusive. Both patients underwent tumor resection. The pathological analysis allowed identifying gouty tophi. Both patients had normal serum uric acid concentration.

Heterogeneous hyposignal on T1 MRI sequences in the left temporomandibular joint. MRI: magnetic resonance imaging.

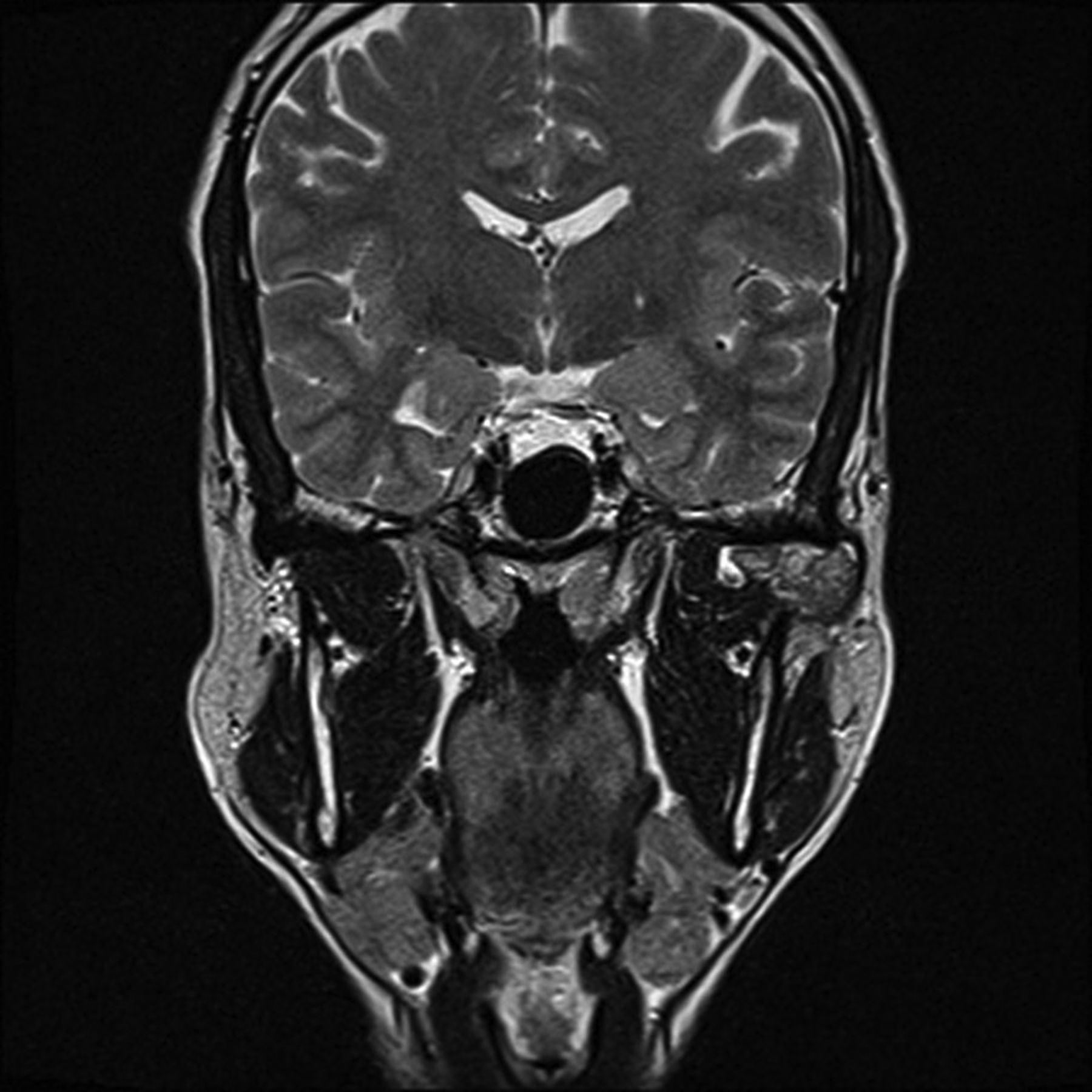
Heterogeneous hyposignal on T2 MRI sequences in the left temporomandibular joint. MRI: magnetic resonance imaging.
To our knowledge, only 8 out of the 11 previously reported cases of TMJ gouty tophi were proven histologically1. None of the 6 fine needle aspirations performed in these cases (including ours) were conclusive, whereas the sensitivity and specificity of tophus aspirates commonly range from 63% to 78% and from 93% to 100%, respectively2. Six patients (including ours) were tested for uric acid concentration, which was always in the normal range. Hyperuricemia is the most important risk factor for gout, but some individuals may present with gout without hyperuricemia2. Imaging is not specific. A CT scan usually shows intra- or extraarticular calcified bodies that most often suggest chondromatosis in this location. The MRI presentation of tophi is nonspecific (intermediate T1 and variable T2 signal) and can appear similar to other soft tissue masses3.
Our cases demonstrate the heterogeneous presentation of gout in an unusual and single location without hyperuricemia and with heterogeneous T1 and T2 hyposignal.








{kind=link}
{kind=link}