

Abstract
Objective. To assess salivary gland ultrasonography (US) as a diagnostic tool for secondary Sjögren syndrome (sSS) in patients with rheumatoid arthritis (RA).
Methods. Salivary gland US images from 30 patients with RA were graded using a validated semiquantitative scoring system. Sicca symptoms, oral health, and RA disease activity were assessed.
Results. US changes consistent with SS were found in 40% of patients. Patients with higher US scores had more sicca symptoms as well as higher RA activity and poorer oral health.
Conclusion. Salivary gland US may aid the diagnosis of sSS in patients with RA.
Sjögren syndrome (SS) is a chronic autoimmune disease characterized by lymphocytic infiltration of the lacrimal and salivary glands resulting in clinical symptoms of keratoconjunctivitis sicca and xerostomia. It may be primary (pSS) or secondary (sSS), and may occur in other rheumatic diseases such as rheumatoid arthritis (RA)1. The reported prevalence of sSS in patients with RA has varied from < 4% to > 40%1,2,3,4; with variation probably related to patient populations, diagnostic criteria, and testing used. In RA, sSS has been associated with more severe disease, higher risk for lymphoma, and worse outcomes5,6,7.
Diagnosing SS can be challenging. The 2002 American European Consensus Group (AECG) classification criteria8 and the 2012 American College of Rheumatology (ACR) classification criteria9 include as diagnostic tests minor salivary gland biopsy, Schirmer’s test/ocular staining, sialography, salivary flow, and scintigraphy. These modalities can be invasive, expensive, painful, and hard to access. The diagnostic utility of serologies [e.g., rheumatoid factor (RF), Ro/SSA, and La/SSB antibodies] is limited in isolation. There has been increasing interest in using salivary gland US to aid SS diagnosis10,11,12,13, and studies have shown good correlation with other imaging modalities14 and minor salivary gland pathology15. Salivary gland US has been suggested to increase the performance of the AECG and ACR criteria10,16. While many studies have focused on pSS, we examined salivary gland US in patients with RA.
MATERIALS AND METHODS
Design
Our study was a cross-sectional observational study in a university-based, rheumatology specialty clinic.
Study population
The subjects were a convenience sample of patients diagnosed with RA according to the 1987 ACR criteria. Exclusion criteria included head and neck malignancies and previous irradiation. The study was approved by the University of California San Diego Human Research Protection Program; all patients provided written informed consent prior to procedures.
Measurements
Standard demographic information was obtained. Functional status was quantified with the multidimensional Health Assessment Questionnaire (HAQ) and RA disease activity by the Routine Assessment of Patient Index Data (RAPID3) score17. Ocular and oral dryness were assessed using a sicca syndrome questionnaire based on questions proposed by the AECG 2002 criteria for SS8. Oral health-related quality of life was measured using the validated Oral Health Impact Profile (OHIP-14)18.
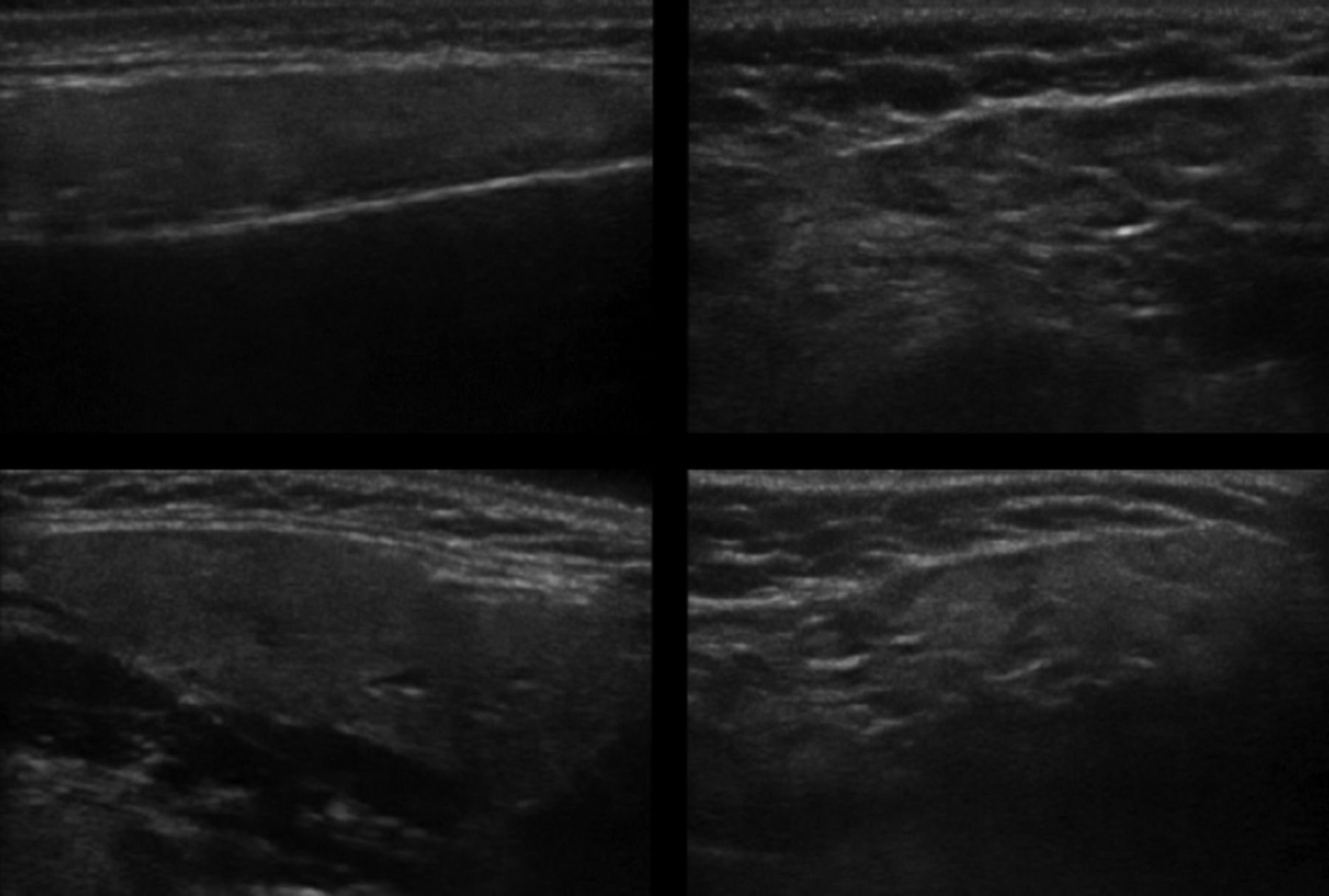
Imaging of the salivary glands was performed using a Sono-Site M-turbo US scanner with an 8–13 MHz (small parts) linear transducer. Thyroid gland US was used as an individual reference. The parotid and submandibular glands were scanned bilaterally in longitudinal and transverse planes and assigned a score based on the system validated by Hočevar, et al11,12. Briefly, 5 variables were semiquantitatively assessed for each gland: parenchymal echogenicity relative to the thyroid gland, homogeneity, presence of hypoechoic areas, presence of hyperechoic foci, and glandular borders (Figure 1). Grades for all 4 glands in each of the 5 variables were summed (maximum score of 48). US images were obtained and scored by 3 observers (SD, DH, and HY). To assess interrater reliability, random sets of ultrasonographic images were scored. With individual scores treated as continuous data, the correlation among raters was high: Pearson correlation coefficient 0.912, p < 0.001. When data were transformed into binary variables (scores < 17 or ≥ 17), correlation using Cohen’s κ was 0.625 (p = 0.03).

Ultrasound images of parotid and submandibular glands. Normal parotid (upper left) and submandibular gland (bottom left), compared to abnormal parotid (upper right) and submandibular gland (bottom right) with structural changes consistent with Sjögren syndrome. The images on the right show gland inhomogeneity, hypoechoic areas, hyperechoic stranding, and poorly defined borders.
Analysis
Standard descriptive statistics were used for demographic and RA characteristics. The population was divided into 2 groups based on their US scores. A cutoff of ≥ 17, validated by Hočevar, et al11,12, classified patients as having ultrasonographic changes consistent with SS. The independent samples t test was used to compare the number of sicca symptoms between those with and without ultrasonographic changes. ANOVA was used to compare the distribution of US scores based on the number of sicca symptoms. Independent samples t-test was applied to compare different measures of RA severity between those with and without ultrasonographic changes. For all statistical tests, α level was set at 0.05. All statistical analyses were performed using SPSS 20 software (IBM Corporation).
RESULTS
Thirty patients with RA were enrolled. Ninety percent (n = 27) of the participants were women with RA with a mean age (± SD) of 57 ± 13 years. Most were nonsmokers (67%, n = 20) or former smokers (27%, n = 8); only 2 (7%) currently smoked. Of 29 patients with available results, 69% were RF-positive; 82% of 28 had antibodies to citrullinated proteins; and 65% of 17 were antinuclear antibody–positive. Results for antibodies to SSA and SSB were only available for 13 and 14 participants; none were positive.
Twelve of 30 participants (40%) had US scores ≥ 17; higher scores indicate more structural changes and scores ≥ 17 are consistent with SS (Figure 1). Those with scores ≥ 17 answered positively to more questions on the sicca syndrome questionnaire (3.3 vs 1.3, p = 0.009). Further, when divided into groups based on the number of sicca questions answered positively, higher numbers of positive responses corresponded with higher US scores (ANOVA, F = 3.13, p = 0.026; Figure 2). Those with US scores ≥ 17 also had significantly worse periodontal health (higher OHIP questionnaire scores; mean scores 14.8 vs 3.2, p = 0.007).

Mean ultrasound (U/S) score grouped by number of positively answered American European Consensus Group (AECG) sicca questions.
When divided by US scores, patients with scores ≥ 17 had significantly higher disease activity (RAPID3 scores). HAQ scores, erythrocyte sedimentation rate, and C-reactive protein were not significantly different between those with and without substantial ultrasonographic changes (Table 1).
Comparison of those with and without changes on ultrasonography. T test of means used for all statistical tests, except where denoted by *, where Fisher’s exact test was used.
DISCUSSION
SS results in structural changes in the salivary glands such as hypoechoic regions and hyperechoic stranding, which are readily detected with US. Several studies have assessed salivary gland US for the diagnosis of pSS10,11,12,13. Our goal was to assess the utility of US in diagnosing sSS among patients with RA. We found that 40% of patients with RA, recruited without knowledge of sicca symptoms, had sonographic salivary gland changes consistent with SS.
Previous studies have reported prevalences of sSS in RA ranging from 4% to 40%2,3,4. Our study, using a sonographic scoring system, found a prevalence of 40%. De Vita, et al assessed salivary gland US in both pSS and sSS and found sonography less sensitive in sSS (53.8% against asymptomatic controls; 46.2% against symptomatic controls) compared to pSS (sensitivity 81.5%), although specificity was still ∼90%19. Notably, their scoring system assessed only 1 variable (gland homogeneity) and validated the diagnosis using older SS criteria. We used a scoring system and cutoff score approach incorporating 5 different US variables, developed by Hočevar, et al and validated against the 2002 AECG criteria11. Subsequently, that group demonstrated reproducibility as well as high specificity (98.7%), with higher sensitivity (58.8%)12.
Cornec, et al demonstrated that using salivary gland US in addition to standard testing used in the 2002 AECG criteria improved sensitivity in diagnosing SS from 77.9% to 85.7%. Because no gold standard exists for SS diagnosis, Cornec, et al used 3 experts as the reference standard. They suggested salivary gland US be used initially to avoid salivary gland biopsy10. It has been proposed that new criteria for SS might incorporate US instead of more invasive modalities13. Our findings further support the potential utility of US in sSS.
Our study demonstrates that not only the severity of reported sicca symptoms correlated significantly with sonographic changes seen on US, but also that patients with changes on salivary gland US had significantly worse oral health-related quality of life. This is an important practical observation because those with SS are known to be more prone to dental caries, oral candidiasis, and periodontal disease1. Periodontal disease has been suggested to correlate with or even contribute to the pathogenesis of RA20. Thus, sonographic diagnosis of sSS in patients with RA may potentially help to identify the patients who need routine assessment and management of their oral health.
In our study, patients with changes on salivary gland US had higher RAPID3 scores than those without changes, indicating more active RA. This contrasts with the findings of Haga, et al and Antero, et al that RA patients with sSS did not have more active disease (using the Disease Activity Score)2,3. It is possible that the RAPID3, consisting of 3 patient-reported outcomes, may better identify this aspect of extraarticular disease.
Although the US changes corresponded well to sicca symptoms, a limitation of our study is that it did not include the more established objective measures of lacrimal and salivary gland structure and function, including salivary gland biopsy, sialography, salivary flow, and scintigraphy. Therefore, this study was not able to make a comparison to currently accepted classification criteria of SS, and it was limited to determining which participants had ultrasonographic changes consistent with the disease. While interrater reliability between 2 of the observers was high, intrarater reliability was not assessed in our study.
Our data support salivary gland US as a potential noninvasive imaging tool for diagnosing sSS in patients with RA.
- Accepted for publication March 4, 2015.








{kind=link}
{kind=link}