

Abstract
Objective. Uric acid (UA) has antiosteoporotic effects in postmenopausal women. This study investigated the association between serum UA levels and bone mineral density (BMD) in young male patients with ankylosing spondylitis (AS).
Methods. One hundred fifty patients who fulfilled the modified New York criteria for the classification of AS were analyzed. All patients were male and under 50 years of age. BMD, serum UA concentrations, clinical variables, and radiographic progression were assessed. The associations between UA and BMD at the lumbar spine and hip were evaluated using multiple linear regression analysis. Multivariate logistic regression analyses were performed to identify risk factors associated with low BMD.
Results. Mean serum UA concentration in the 150 patients with AS was 5.5 ± 1.3 mg/dl. BMD at the lumbar spine, but not at the total hip and femoral neck, increased with increasing serum UA tertiles (p = 0.033). The significant positive association between serum UA and BMD at the lumbar spine remained after adjustment for confounding factors (β = 0.185, p = 0.014, adjusted R2 = 0.310). Multiple logistic regression analyses showed that lower UA concentrations (OR 4.02, 95% CI 1.34–12.3) and body mass index and increased erythrocyte sedimentation rate were independently associated with the risk of low BMD.
Conclusion. Lower serum UA levels are associated with lower BMD in young male patients with AS. UA may be a novel predictive marker or therapeutic target in patients with AS.
Uric acid (UA) is an end product of purine metabolism. Because purines are among the main essential components of DNA and RNA, UA is closely related to the life of an organism. UA has double-edged characteristics, acting as a proinflammatory agonist in diseases and as an antioxidant and antiinflammatory agent. Hyperuricemia is associated with gout, renal disease, cardiovascular disease, and metabolic syndrome1,2,3,4. Although UA in its crystalline state has proinflammatory properties, the biological roles of soluble UA are unclear. Circulating serum UA has been shown to strongly and positively affect human resistance to oxidative stress5. The antioxidant activity of UA is much higher than that of other antioxidants, including vitamins and enzymatic antioxidants6, with UA accounting for about half of the antioxidant activity in human plasma7.
Oxidative stress has been found to play a role in the pathogenesis of osteoporosis8. UA was reported to have antiosteoporotic properties. For example, a population-based study among older men found that higher serum UA concentrations were significantly associated with a lower prevalence of osteoporosis and fracture9. In addition, a prospective case-cohort study of fracture in elderly men showed that higher serum UA levels were associated with increased bone mineral density (BMD) and reduced nonspinal fracture rate10. Further, large cross-sectional studies in postmenopausal women showed an association between higher UA and higher BMD11 and that the association of lower UA levels with decreased BMD was also associated with a higher prevalence of vertebral fractures in healthy postmenopausal women12.
The association between UA and BMD is thought to be related to the antioxidant effects of normal serum UA concentrations. Hyperuricemia has been found to increase the risk of cardiovascular disease, in which oxidative stress plays an important pathophysiologic role7. Whereas normal serum UA concentrations may have an antioxidant effect, supersaturation in blood may result in UA becoming a pro-oxidant13. Therefore, depending on its concentration, UA may be a protective antioxidant or a detrimental pro-oxidant14. In addition, UA was found to dose-dependently reduce osteoclastogenesis and the production of reactive oxygen species (ROS) in osteoclast precursors in vitro, suggesting that UA may directly affect osteoclastogenesis12.
Ankylosing spondylitis (AS) is characterized by low BMD and bone loss in the spine and hips, which begin at an early stage of the disease15. Aging and menopause are important in the pathogenesis of osteoporosis in older aged individuals, whereas increased bone resorption caused by chronic inflammation is the main cause of secondary osteoporosis in patients with rheumatoid arthritis and AS. In both of the latter conditions, multiple proinflammatory cytokines, chemokines, and growth factors of immune system cells activate osteoclasts, leading to periarticular osteopenia and systemic bone loss15. Although the relationship between serum UA and BMD has been assessed in older patients with primary osteoporosis, no study to our knowledge has examined this relationship in younger patients with inflammatory arthritis and secondary osteoporosis.
Our study was therefore designed to investigate the association between serum UA concentrations and BMD at the lumbar spine and hip (femoral neck and total proximal femur) in young male patients with AS and to analyze the effect of serum UA concentrations on the development of BMD below the expected range for patient age.
MATERIALS AND METHODS
Study patients
This was a retrospective analysis of medical records obtained from Seoul Saint Mary’s Hospital and Incheon Saint Mary’s Hospital, Seoul, Korea. We enrolled 298 consecutive patients with AS evaluated between January 2009 and February 2013. To exclude the effects of sex and age, 61 female patients and 34 male patients aged 50 years or older were excluded. Of the remaining 203 male patients with AS under age 50 years, 31 without BMD measurements and 22 without laboratory data at the time of BMD measurement were also excluded. Thus, this analysis included 150 male patients with AS who fulfilled the modified New York criteria for the classification of AS16. Other exclusion criteria were psoriasis, inflammatory bowel disease, reactive arthritis, thyroid or parathyroid disorders, chronic liver disease, and chronic kidney disease [glomerular filtration rate (GFR) < 90 ml/min/1.73 m2]. Patients who had taken medicines including allopurinol, fenofibrate, β blocker, and diuretics were also excluded because of their possible effect on serum levels of UA. Our study was approved by the ethics committees of Seoul St. Mary’s Hospital (XC13RIMI0129K) and Incheon St. Mary’s Hospital, Catholic University of Korea (XC13RIMI0129O).
Clinical data
Clinical assessments included demographic data (age, age at diagnosis of AS, presence of HLA-B27), and history of peripheral arthritis, uveitis, and enthesitis. Height and weight were measured at the time of BMD measurements and used to calculate body mass index (BMI). Medications were also recorded, including nonsteroidal antiinflammatory drugs, sulfasalazine, methotrexate, tumor necrosis factor (TNF) inhibitors, calcium, and bisphosphonate; patients who were taking medications for more than 6 months at BMD measurement were considered sustained users. No patient received systemic glucocorticoid agents.
BMD measurements
Areal BMD of the lumbar spine (L1 to L4) and right hip were measured by dual-energy X-ray absorptiometry (Lunar Prodigy densitometer). All measurements were taken by experienced operators on the same machine using standardized procedures for participant positioning. BMD was measured in the lumbar spine (L1–L4) and the right hip (femoral neck and total proximal femur), and was expressed as the number of grams of bone mineral per square centimeter (g/cm2) and as the number of SD above or below the mean for a healthy 30-year-old adult of the same sex and ethnicity as the patient (T score). For patients under age 50 years, a Z score ≤ −2.0 SD (compared with the age-matched mean) was considered below the expected range for age17. Data were compared with the manufacturer’s reference values.
Radiographic scoring
Sacroiliitis was assessed by viewing images of the sacroiliac joint and was graded according to the New York criteria16 by a reader blinded to the clinical details of the patients. Radiographic changes in the lumbar spine related to AS were assessed using the Stokes Ankylosing Spondylitis Spine Score (SASSS). SASSS was calculated by scoring the anterior and posterior vertebral corners of the lumbar spinal segments, from T12 lower to S1 upper, with each segment scored from 0–3 points (0 = normal; 1 = erosion, sclerosis, or squaring; 2 = syndesmophyte formation; and 3 = a bridging syndesmophyte)18. Thus, total scores were ranged from 0 to 72. The number of syndesmophytes was assessed by SASSS.
Laboratory measurements
Laboratory data included the serum UA, calcium, phosphorus, and alkaline phosphatase (ALP) concentrations. GFR was calculated using the Cockroft-Gault formula19. Inflammatory status was assessed by measuring the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) concentration.
Statistical analysis
Analyses were performed using SPSS (version 18.0; SPSS Inc.). The patients were categorized into 3 tertiles according to their serum UA concentration. Continuous data were expressed as mean ± SD and categorical data as percentages. Clinical variables and BMD values were compared in subgroups across tertiles of UA using chi-square tests for categorical variables, ANOVA for normally distributed continuous variables, and Kruskal-Wallis nonparametric tests for nonparametric distributed covariates. Multivariate-adjusted mean BMD at each site, according to serum UA tertiles, was estimated using ANCOVA after adjusting for confounders. The nonparametric, locally weighted scatterplot smoothing (LOESS) method was used to assess the relationship between serum UA and BMD at the lumbar spine.
Multiple linear regression models were used to assess the association between UA (independent variable) and BMD at the lumbar spine (dependent variable). Multiple regression models were adjusted for age (model 1); age and BMI (model 2); age, BMI, and ESR (model 3); and age, BMI, ESR, and serum calcium (model 4). In the multiple analyses, an enter method was used. Binary logistic regression analysis was used to ascertain the association between serum UA and BMD below the expected range for age after adjusting for potential confounders. All variables with a p value < 0.10 in the univariable analysis were incorporated as explanatory variables. p < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
The clinical characteristics of the study patients are shown in Table 1. The mean age of the 150 patients was 32 ± 8 years, and their mean serum UA concentration was 5.5 ± 1.3 mg/dl (range 1.8 mg/dl to 9.1 mg/dl). Only 17 patients (11.3%) had hyperuricemia (serum UA ≥ 7.0 mg/dl). BMI was higher in patients with AS who had higher rather than lower serum UA concentrations, but the difference was not significant. There were no significant differences among the subgroups of patients in the UA tertiles in the presence of HLA-B27, or in the history of peripheral arthritis, uveitis, and enthesitis. Moreover, there was no difference among these subgroups in radiographic progression or treatment agents. Concentrations of calcium were higher in the higher UA tertiles (p = 0.004), but there were no significant differences in ESR or GFR, or in the concentrations of CRP, phosphorus, or ALP.
Patient characteristics, stratified by serum UA tertiles. Values are mean ± SD or n (%) unless otherwise specified.
Relationship between BMD and UA tertiles
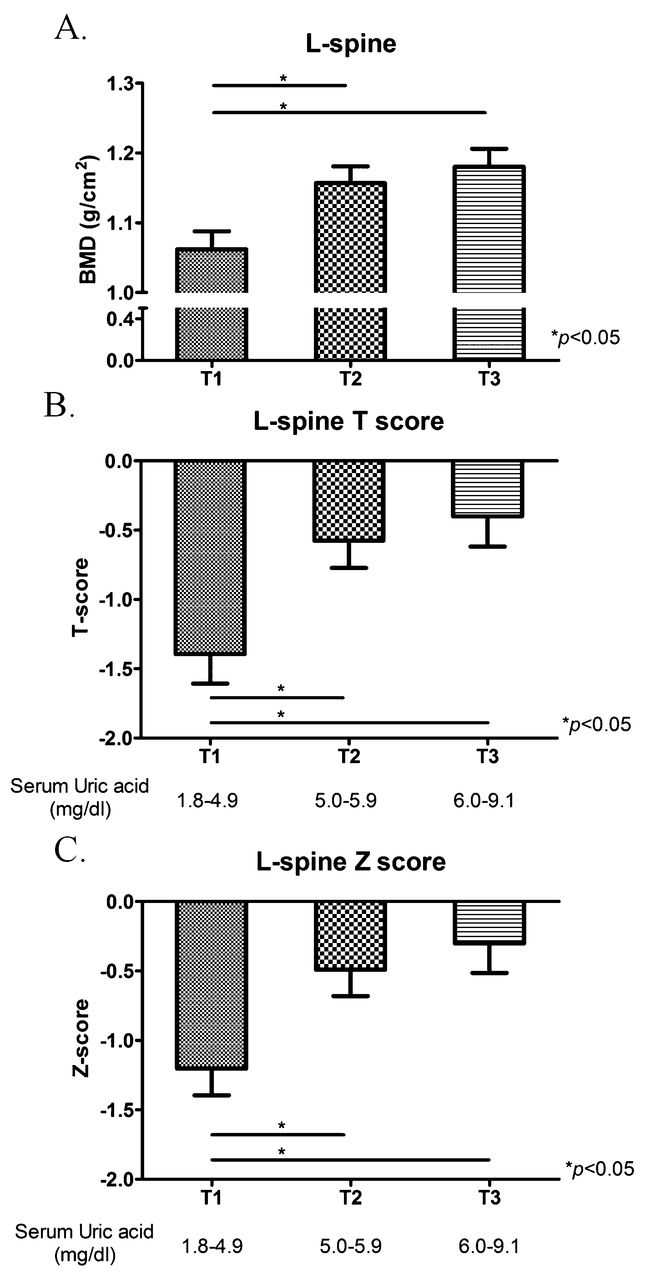
BMD at the lumbar spine, but not at the total hip and femoral neck, increased as serum UA tertiles increased (p = 0.033). The relationship between BMD at the lumbar spine and serum UA tertiles remained significant after adjustment for age, BMI, and ESR (Figure 1). Patients with AS with the lowest tertile of UA concentration tended to have lower BMD than those with higher UA levels (Figure 2). T score (p = 0.002) and Z score (p = 0.004) in the lumbar spine were also significantly higher in the groups with higher UA tertiles.

BMD in the lumbar spine, femoral neck, and total hip as a function of UA tertiles after adjusting for confounding factors, including age, BMI, and ESR. All p values were calculated using an ANCOVA model with BMD as a factor and age, BMI, and ESR at BMD measurement as covariates. BMD: bone mineral density; UA: uric acid; BMI: body mass index; ESR: erythrocyte sedimentation rate.

BMD in the lumbar spine according to serum UA tertiles. A. BMD. B. T score. C. Z score. *Statistically significantly different from the lowest tertile. BMD: bone mineral density; UA: uric acid.
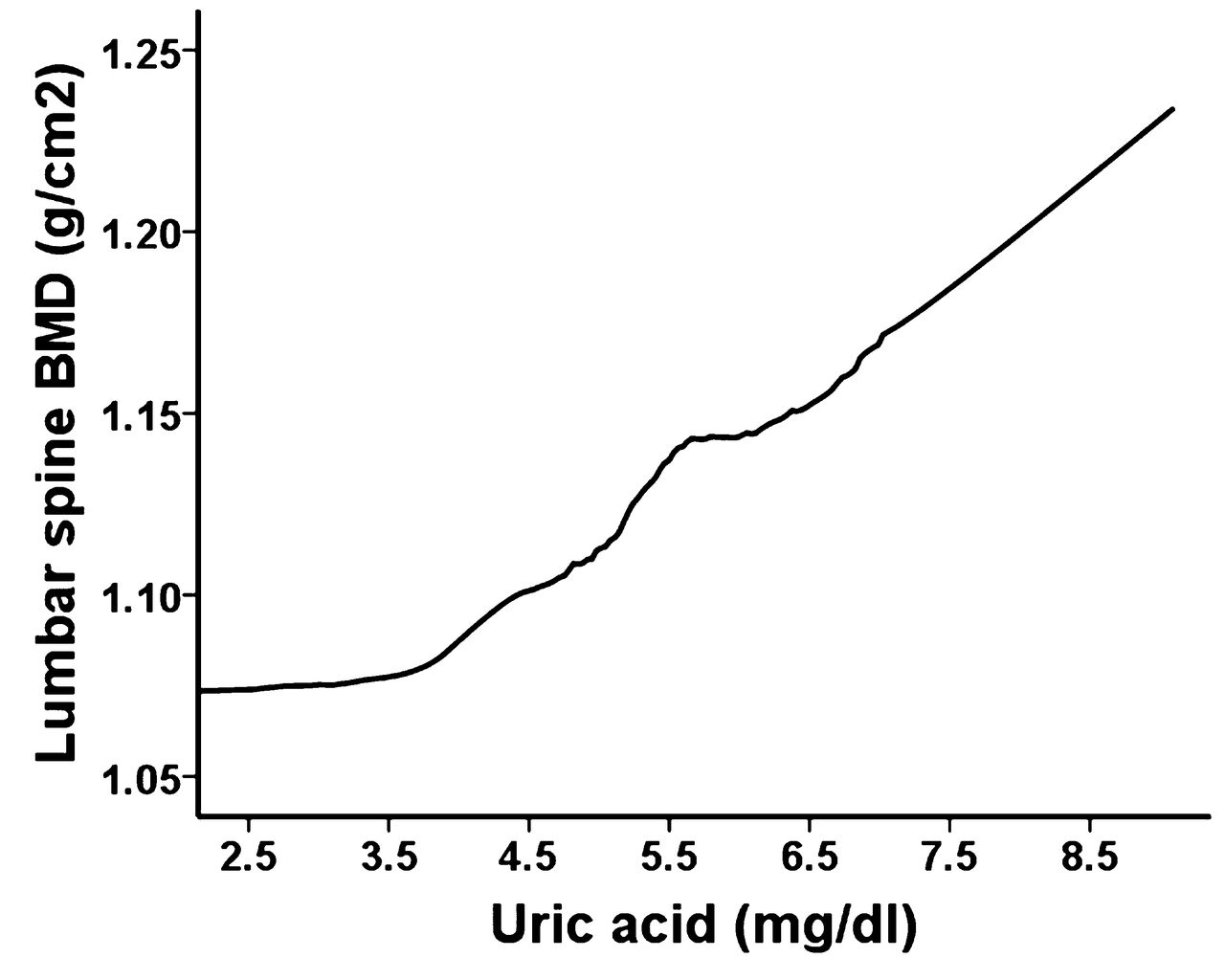
The LOESS method was used to determine whether UA concentration affects BMD at the lumbar spine (Figure 3). LOESS plots of lumbar spine BMD and UA concentration showed that the relationship was piecewise linear, with an inflection around a UA concentration of 4.0 mg/dl and a steeper slope above a UA concentration of 4.5 mg/dl.

The LOESS plot of lumbar spine BMD as a function of UA concentration. LOESS: locally weighted scatterplot smoothing; BMD: bone mineral density; UA: uric acid.
Multiple linear regression analysis
Multiple regression analysis showed that, after adjustment for age (model 1), serum UA concentration was significantly correlated with BMD at the lumbar spine (Table 2). This association remained significant after adjusting for age and BMI (model 2); age, BMI, and ESR (model 3); and age, BMI, ESR, and serum calcium concentration (model 4, β = 0.185, SE = 0.011, p = 0.014, adjusted R2 = 0.310).
Multiple linear regression analysis of the association between serum UA concentration and lumbar spine bone mineral density.
Multiple logistic regression analysis for BMD below expected range for age
Of the 150 young male patients with AS, 39 (26%) had BMD below the expected range for age. Table 3 shows the results of univariable and multivariable logistic regression analyses of the factors associated with low BMD. Univariable analysis showed that factors significantly associated with low BMD included low UA concentrations (OR 3.50, 95% CI 1.34–8.99), high BMI (OR 0.1, 95% CI 0.02–0.49), increased ESR (> 10 mm/h, OR 2.50, 95% CI 1.13–5.51), and the absence of HLA-B27 (OR 4.79, 95% CI 1.08–21.19). The presence of syndesmophytes showed a moderate association (OR 1.87, 95% CI 0.89–3.94). After adjustment for potential confounding factors, UA levels were independently associated with a BMD below the expected range for age. High BMI (≥ 23.0 kg/m2) significantly decreased the risk of low BMD, while elevated ESR also increased the risk of low BMD.
Univariable and multivariable analysis of factors associated with BMD below the expected range for age in young male patients with AS.
DISCUSSION
To our knowledge, this is the first study to investigate the association between serum UA concentration and BMD in patients with AS. In this cross-sectional analysis of young male patients with AS, high serum UA levels were significantly associated with higher BMD at the lumbar spine. Moreover, low serum UA concentrations increased the risk of BMD below the expected range for age. In addition, low BMD in young male patients with AS was associated with BMI and ESR.
Several studies have reported that high serum UA concentrations are associated with a high BMD and a low prevalence of fracture in elderly men9,10 and postmenopausal women11,12. One study in a population aged 25–54 years showed that serum UA was positively associated with BMD at the lumbar spine in men, but not in women20. The results presented here indicate that serum UA levels were associated with BMD at the lumbar spine, but not at the femur, in accordance with previous findings in young healthy males. Although most studies of the relationship between UA and BMD have involved healthy populations, this association had not been analyzed in patients with inflammatory arthritis, a frequent cause of secondary osteoporosis.
Osteoporosis has been reported to develop in 19% to 61% of patients with AS21, including in 37% of Korean patients with AS22. Disease activity in AS contributes to the rate of bone loss, with osteoporosis being not a comorbidity, but rather a manifestation of the disease itself23. New insights into osteoimmunology have helped link inflammation with bone loss in AS. Under chronic inflammatory conditions, TNF-α and interleukin 6 (IL-6) inhibit osteoblasts by inhibiting the Wnt pathway through upregulation of Dickkopf-related protein and sclerostin. TNF-α and IL-6 amplify osteoclastogenesis through the induction of the receptor activator of nuclear factor-κB ligand. Systemic osteoporosis in AS can be explained by the inflammatory activities of TNF-α and IL-6, which inhibit osteoblasts while stimulating osteoclasts24.
Although low BMD is caused by inflammatory conditions, the association of BMD with UA in osteoporosis secondary to AS has not yet been clarified. Among the possible mechanisms is the direct involvement of UA in the pathogenesis of osteoporosis because of its antioxidant properties. UA is an important endogenous antioxidant that chelates metal ions and it can scavenge superoxide, hydroxyl radicals, and singlet oxygen, as well as block the formation of the strong oxidant peroxynitrate25,26.
Oxidative stress has been identified as a potential mechanism that attenuates osteoblastogenesis and bone formation27. Observational studies have found that oxidative stress or plasma antioxidant concentrations are associated with bone health and mass8,28,29. Depletion of antioxidants and elevated production of ROS by oxidative stress have been observed in inflammatory joint diseases30. ROS has been found to play a role in osteoporosis by inhibiting the generation of osteoclasts from osteoprogenitor cells31. ROS levels are increased in patients with AS, and this increase is accompanied by the increased production of proinflammatory cytokines32. A study found that UA reduced the production of ROS in mouse osteoclast precursors, indicating that the positive association between UA and BMD may be related to the antioxidant effect of UA12.
Several clinical studies have shown that UA has beneficial effects on bone metabolism. Serum UA concentrations are negatively associated with the urinary excretion of the aminoterminal cross-linked telopeptide of type I collagen9, as well as with the bone resorption marker, C-terminal telopeptide of type I collagen12,20. An in vitro study in mouse cells showed that UA decreased osteoclastogenesis in a dose-dependent manner12. Additional studies are needed to clarify whether UA acts directly on osteoclasts rather than through oxidative stress.
Other possible mechanisms may explain the association between UA and BMD. In agreement with previous results9, we found a positive correlation between serum UA and calcium concentrations (data not shown). Metabolic changes associated with osteoporosis may influence the clearance of UA. Parathyroid hormone (PTH) is associated with UA clearance, and serum UA and PTH concentrations show positive correlations9,33,34. Serum UA is also associated with serum 1,25-(OH)2D3 levels by regulating 1α-hydroxylase activity35. Because we did not measure serum PTH and Vitamin D levels, these associations could not be evaluated.
Alternatively, UA may affect the urinary excretion of calcium. Patients with AS are known to have higher prevalence of renal stones as a result of hypercalciuria. Hypercalciuria is considered to have a relationship with inflammatory cytokines, such as TNF-α and IL-636. Although we did not measure urinary calcium excretion directly, the results in our study showed that concentrations of serum calcium were higher in the higher UA tertiles. This finding suggests that serum UA may affect the urinary excretion of calcium.
Our study had several limitations. First, several important variables, including bone turnover markers, PTH, and Vitamin D, were not measured. These variables were not matched among 3 groups and could have affected these results. Another limitation of our study was the use of the SASSS system to quantify spinal radiographic progression. This system is limited in that it takes into account the structural changes in the lumbar spine without the assessment of the cervical or thoracic spines. In addition, the study design was cross-sectional; thus, although we could assess associations, we could not determine a cause-effect relationship. Finally, we could not analyze the effects of smoking and alcohol habits on BMD because this information was not available in this retrospective analysis.
Our study also had several strengths. It included only young male patients with AS, which excluded any effects of age and sex. Despite it being a retrospective analysis, our study is, to our knowledge, the first to evaluate the association between UA with BMD and the prevalence of low BMD in patients with inflammatory arthritis.
Serum concentrations of UA were positively correlated with BMD at the lumbar spine in young male patients with AS. Lower serum UA concentrations also increased the likelihood of BMD below the expected range for age. Serum UA may have beneficial effects on BMD in patients with AS. These findings suggest that antioxidants, in addition to controlling inflammation, may be important in bone metabolism in patients with AS. Further prospective longitudinal studies are needed to determine whether UA plays a direct role in bone metabolism in inflammatory arthritis.
Footnotes
-
Supported by a grant from the Korea Healthcare Technology R&D project, Ministry of Health, Welfare, and Family Affairs, Republic of Korea (A092258), and the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science, and Technology (2010-0003446).
- Accepted for publication February 3, 2015.








{kind=link}
{kind=link}
{kind=link}