

Abstract
Objective. Monocytes of children with enthesitis-related arthritis (ERA) show Toll-like receptor 4 (TLR4) overexpression. Tenascin-C (TNC) is an extracellular matrix glycoprotein and acts as an endogenous TLR4 ligand. Thus, we studied the serum and synovial fluid (SF) levels of TNC in children with ERA.
Methods. TNC was measured in the serum of 80 children with ERA satisfying the International League of Associations for Rheumatology criteria. Fifteen children were followed up while being treated with regular nonsteroidal antiinflammatory drug (NSAID) therapy and levels were reassessed at 3 months. Seventeen paired serum-SF samples and 25 healthy control serum samples were also analyzed. Disease activity was assessed by physician’s global assessment (PGA), early morning stiffness (EMS), tender (TJC) and swollen joint counts (SJC), enthesitis score, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).
Results. The mean serum TNC level in patients with active disease (67.1 ± 44.9 ng/ml) was significantly higher than in those with inactive disease (40.6 ± 36.7 ng/ml, p = 0.01) and healthy controls (21 ± 15.2 ng/ml, p < 0.001). Levels of TNC were higher in HLA-B27–positive (58.4 ng/ml) versus −negative disease (20.4 ng/ml, p = 0.01). TNC levels correlated moderately with disease activity: PGA r = 0.4, EMS r = 0.34, TJC r = 0.4, SJC r = 0.46, ESR r = 0.42, and CRP r = 0.32. In receiver-operation characteristic analysis for active versus inactive diseases, TNC [area under the curve (AUC) = 0.754] was equivalent to ESR (AUC = 0.787) and CRP (AUC = 0.789). Regular NSAID therapy led to a significant fall in serum TNC levels at 3 months (p = 0.0003). The SF TNC level was 17.39 ng/ml, significantly lower than the paired serum values (p = 0.01).
Conclusion. Serum TNC levels are significantly raised and correlate with various clinical and laboratory variables of disease activity in children with ERA. Regular NSAID therapy reduces the TNC levels, probably related to controlling disease activity.
Juvenile idiopathic arthritis (JIA) is a chronic inflammatory disorder with diverse articular and extraarticular manifestations. It affects 1 in 1000 children and is a leading cause of acquired disability among children1. According to the International League of Associations for Rheumatology (ILAR) classification, there are 7 categories2. Even though oligoarticular is the most common subset worldwide, enthesitis-related arthritis (ERA) is the most common category in Southeast Asia3.
The pathogenesis of ERA is not known; however, unlike other rheumatic diseases, no autoantibodies or autoreactive T cells have been detected, although a strong association with HLA-B27 is reported. It is suggested that HLA-B27 unfolded protein response in conjunction with the activation of Toll-like receptor 4 (TLR4) by lipopolysaccharide results in a cross-talk leading to secretion of interleukin (IL) 234. Thus, it is believed that an interaction between microbial trigger and HLA-B27 probably leads to chronic immunoinflammation in joints5. Microbes activate the immune system through TLR and increased expression of TLR has been seen in various immunoinflammatory disorders, including JIA-ERA6. The basic question is that after the microbial trigger, how is the inflammation sustained? Is it because of the presence of endogenous ligands for TLR and the continued stimulation of the innate immune system by the endogenous ligands?
Tenascin-C (TNC) is a large extracellular matrix glycoprotein and consists of N-terminal TNC assembly domain, 14.5 epidermal growth factor–like repeats, fibronectin type III repeat domains (8 constant and up to 9 alternatively spliced), and the C-terminal fibrinogen-like globular domain. Further, it forms a trimer by twisting at the N-terminal and is bound by disulfide bonds to exist as a hexamer in tissues7. It is expressed by myeloid cells in response to pathogen-associated molecular patterns, mechanical strain, reactive oxygen species, certain cytokines, and growth factor, and acts as a danger-associated molecular protein. C-domain of TNC interacts with TLR4 on monocyte, monocyte-derived macrophages, and dendritic cells and leads to the secretion of proinflammatory cytokines, like tumor necrosis factor-α, IL-6, and IL-8 production in a dose-dependent manner8. It is normally repressed as soon as the process of inflammation and repair in the tissue is completed and is undetectable in healthy tissues. However, its uncontrolled expression can lead to an autocrine loop involving myeloid cells that amplifies chronic inflammation in the absence of pathogens8,9. It is shown that dendritic cells from TNC-deficient mice produced lower levels of cytokines and exhibited specific defects in Th17 cell polarization10. Thus, after initial microbial trigger, TNC can act as an endogenous ligand for TLR4 that, in conjunction with unfolded HLA-B27 protein, can contribute to sustained chronic inflammation.
Injection of TNC in joints of wild-type mice induces inflammation. In the zymosan-induced–arthritis mice model, TNC-knockout mice exhibit accelerated resolution of arthritis and are protected from persistent inflammation and erosive disease11. There is a sustained expression of TNC in the synovium of patients with rheumatoid arthritis (RA) where it correlates with other inflammatory cytokines such as IL-6, suggesting that it has a role in synovial inflammation9. The serum levels are raised in RA, correlate with bony erosion counts using ultrasound, and show change with therapy12.
We have shown increased TLR4 RNA and protein expression in peripheral blood as well as in synovial fluid (SF) monocytes of children with JIA-ERA6. Being an endogenous ligand of TLR4, TNC is likely to play an important role in the pathogenesis of sustained inflammation in JIA-ERA. However, to our knowledge, no data are available regarding TNC in JIA-ERA. Thus, we studied TNC levels in the serum and SF of children with JIA-ERA and changes with nonsteroidal antiinflammatory drug (NSAID) therapy.
MATERIALS AND METHODS
Patients
Our study was conducted at the Sanjay Gandhi Postgraduate Institute and was approved by the institutional ethics committee. Diagnosis of JIA-ERA was made based on the ILAR classification criteria2. In addition, children with a history of diarrhea or urinary tract infection 4 weeks prior to onset of arthritis were diagnosed with reactive arthritis and those with isolated spine involvement without a history of peripheral arthritis were diagnosed with juvenile ankylosing spondylitis (AS). These 2 groups of patients were not considered JIA-ERA and were excluded from the study. Age limit for inclusion was up to 18 years. A total of 80 patients were enrolled from September 2013 to March 2014. Each participant was given an information sheet in regional language and a consent form was signed. Twenty-five young adults with a median age of 22 years (range 16–25) and similar sex were enrolled as controls. Blood samples were collected from all the subjects. Paired SF was collected from 17 children requiring intraarticular injection of corticosteroid for control of symptoms as decided by the treating physician. During the procedure, SF was collected after consent. Fifteen newly diagnosed patients were treated with regular NSAID (naproxen sodium 20 mg/kg twice daily or indomethacin 3 mg/kg daily) and were followed up at 3 months to collect a second blood sample. All the samples were stored at −80°C.
Clinical assessment
All patients were evaluated and these variables were measured: physician’s global assessment (PGA; 0–10 scale); duration of early morning stiffness (EMS); presence or absence of inflammatory back pain, sacroiliitis, or uveitis; tender, swollen, and damaged joint counts (TJC-68 joints, SJC-66 joints, DJC-68 joints); Maastricht Ankylosing Spondylitis Enthesitis Score (range 0–13); and other enthesitis site counts. The use of NSAID, oral steroids, or disease-modifying antirheumatic drugs at the time of enrollment was also noted.
Laboratory tests
Acute-phase proteins, erythrocyte sedimentation rate (ESR; Westergren method), and C-reactive protein (CRP; nephelometry) were estimated as laboratory markers of disease activity. DNA was extracted from EDTA blood samples using the salting out method. Amplification refractory mutation system PCR was used for HLA-B27 typing13 applying 3 B27-specific primers: 1 forward B1 (5′-GCT ACG TGG ACG ACA CGC T-3′), and 2 reverse B2 (5′-CTC GGT CAG TCT GTG CCT T-3′) and B3 (5′-TCT CGG TAA GTC TGT GCC TT-3′). A conserved intronic region of HLA-DR was also amplified as an internal control using 2 primer sets: C1 (5′-TGC CAA GTG GAG CAC CCA A-3′) and C2 (5′-GCA TCT TGC TCT GTG CAG AT-3′). TNC levels in serum and SF were measured using Human TNC Large (FNIII-C) Assay ELISA Kit from IBL International (code number 27751). It detects TNC high molecular weight variant using 2 different kinds of highly specific antibodies: the coating antibody against fibronectin III-C domain, and the labeled antibody against epidermal growth factor–like domain. The measurement range of the kit was 0.38–24 ng/ml, and sample dilution was done in 1:4 ratios with the enzyme immunoassays buffer provided in the kit (1% bovine serum albumin, 0.05% Tween 20 in phosphate buffered saline). IL-6 levels were similarly measured in the serum and SF using an ELISA kit (BD Bioscience).
Statistical analysis
The data were analyzed and graphically projected using IBM SPSS Statistics Software, version 16 and GraphPad Prism, version 6.00 for Mac (trial version; GraphPad Software).
RESULTS
Patient characteristics
Among the 80 patients, most were boys (9:1) with an average age at disease onset and presentation of 11.2 ± 3 years and 15.7 ± 3 years, respectively. The duration of disease was 4.4 ± 3.5 years. Eighty percent had active arthritis and 63% had active enthesitis. All the children had a progressive disease duration for at least 3 months with nearly half having a history of episodic arthritis. Most of the children were HLA-B27–positive (n = 71, 89%) and 29% had a positive history of JIA-ERA or spondyloarthritis (SpA) in the family. At the time of study inclusion, most patients were receiving NSAID off and on, 12 were receiving weekly methotrexate (MTX) therapy (15%), and 7 were receiving low-dose oral prednisolone (9%, < 10 mg/day).
The average PGA (0–10) was 4.5 ± 2.2. Average EMS was 50 ± 57 min with TJC 4 ± 4 and SJC 3 ± 3. Thirty-nine percent had inflammatory back pain, 43% had sacroiliitis clinically, and 8% had a history of acute anterior uveitis. Average ESR and CRP were 72 ± 37 mm at 1 h and 6.9 ± 5.6 mg/dl, respectively. Twenty-five percent of children had documented damaged joints with an average count of 2 ± 2. Sixteen children out of 80 had no tender or swollen joints and were classified as having inactive disease.
Children who received intraarticular injections were similar in age of onset and duration of disease to those not receiving intraarticular injections. All children had active arthritis as well as swelling and pain in the knee joint, interfering with activities of daily living. Patient characteristics, disease activity variables, and proportion of patients with active and inactive disease were not different in the HLA-B27–positive (n = 71) and −negative groups (n = 9), except that the duration of EMS among the groups showed a significant statistical difference [HLA-B27–positive 30 min (0–180) and HLA-B27–negative 0 min (0–45), p = 0.042].
Fifteen patients treated with regular NSAID showed an average global improvement of 54%, a decrease in EMS from 60 min to 24 min, TJC from 4 to 2, SJC from 3 to 1.5, ESR from 90 mm to 59 mm at 1 h, and CRP from 8.1 mg/dl to 3.6 mg/dl at the end of 3 months.
Circulating TNC levels were raised in children with JIA-ERA
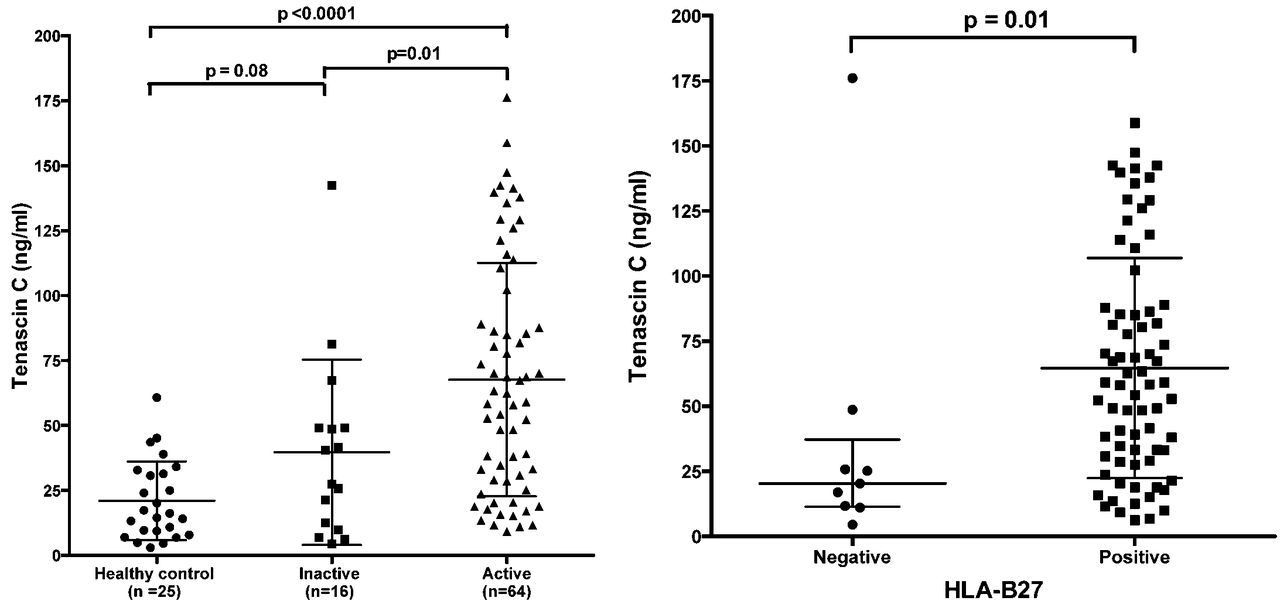
TNC levels were significantly raised in patients with JIA-ERA (62.1 ± 44.2 ng/ml) compared to healthy controls (21 ± 15.2 ng/ml, p < 0.0001). The mean serum level in children with active disease (67.1 ± 44.9 ng/ml) was significantly higher than in children with inactive disease (40.6 ± 36.7 ng/ml, p = 0.01) and in healthy controls (p < 0.0001; Figure 1, left panel). Median levels were higher in HLA-B27–positive 58.4 ng/ml [interquartile range (IQR) 22.1–111.3] versus −negative disease 20.4 ng/ml (IQR 10–37.2, p = 0.003; Figure 1, right panel). The levels did not correlate with age (r = −0.2, 95% CI −0.4–0.02, p = 0.06).

Tenascin-C levels in JIA-ERA (left panel; active and inactive disease) and healthy controls (mean and SD). Tenascin-C levels in HLA-B27–positive and –negative JIA-ERA (right panel; median and IQR). JIA: juvenile idiopathic arthritis; ERA: enthesitis-related arthritis; IQR: interquartile range.
Circulating TNC levels were predictive of activity
Serum levels correlated positively with disease activity variables such as PGA (r = 0.4, 95% CI 0.15–0.58, p = 0.001), EMS (r = 0.34, 95% CI 0.1–0.55, p = 0.005), TJC (r = 0.4, 95% CI 0.2–0.6, p = 0.0003), SJC (r = 0.46, 95% CI 0.27–0.6, p < 0.0001), ESR (r = 0.42, 95% CI 0.21–0.6, p = 0.0002), and CRP (r = 0.32, 95% CI 0.1–0.5, p = 0.007), and negatively with duration of disease (r = −0.33, 95% CI −0.5 to −0.7, p = 0.003). The levels did not correlate with the number of sites with active enthesitis and DJC. In receiver-operation characteristic (ROC) analysis for active versus inactive disease, TNC (AUC = 0.754) was equivalent to ESR (AUC = 0.787) and CRP (AUC = 0.789; Figure 2).

ROC analysis for active versus inactive disease using tenascin-C, ESR, and CRP. ROC: receiver-operation characteristic curve; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein.
Circulating TNC levels changed with therapy
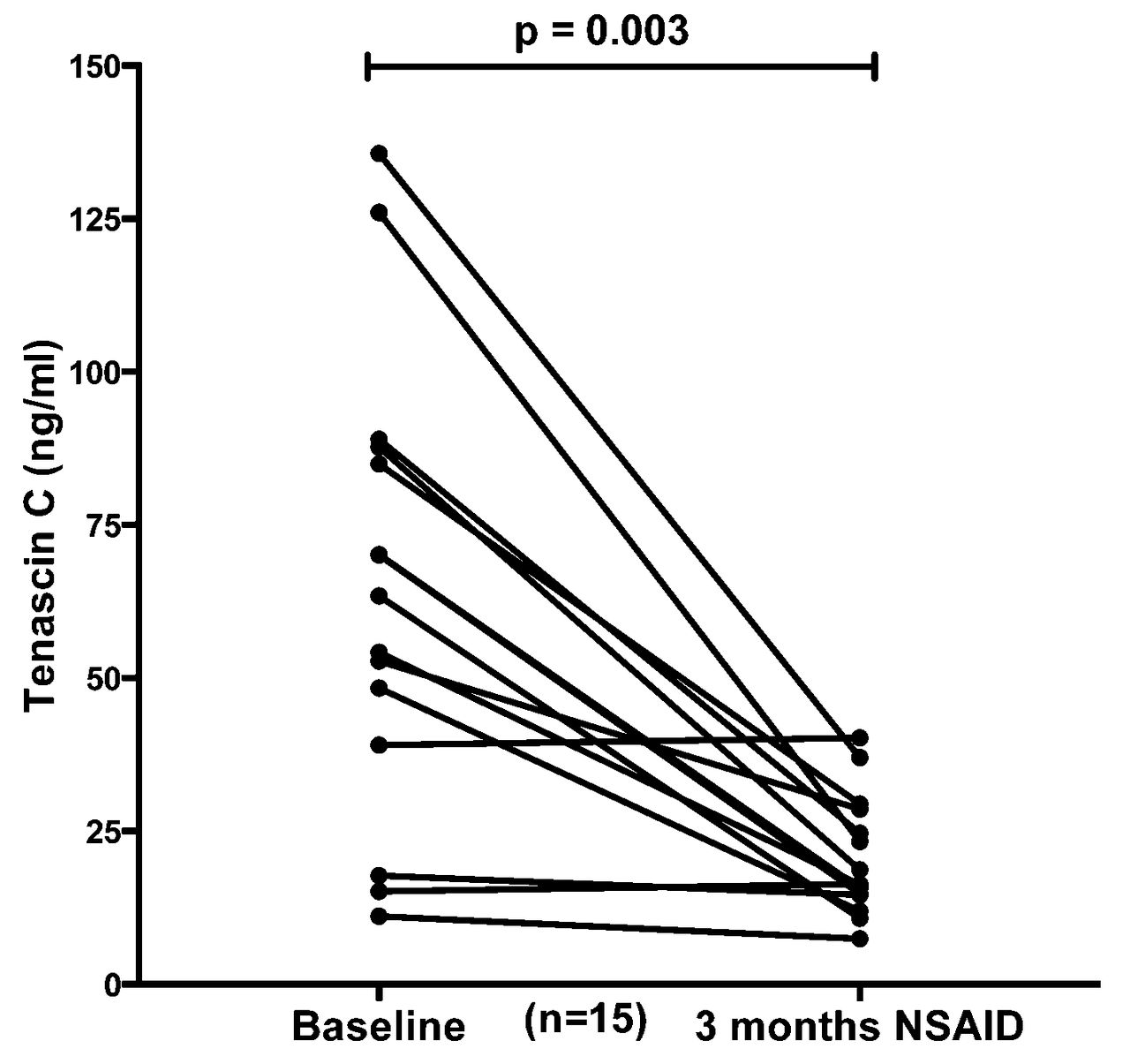
Treatment with regular and full dose of NSAID led to a significant fall in the serum TNC levels at 3-month followup (p = 0.0003; Figure 3). Three patients had low TNC levels at baseline and showed no significant changes at 3 months; 1 of these patients was HLA-B27−negative. In a cross-sectional study, the levels were not different among the patients receiving regular treatment with MTX and steroid compared to those receiving NSAID on and off.

Tenascin-C levels at baseline and at 3-month followup during regular treatment with NSAID. NSAID: nonsteroidal antiinflammatory drug.
SF TNC levels were lower than the serum levels
The median SF TNC level in JIA-ERA was 17.39 ng/ml. The levels were significantly lower than the paired serum values (p = 0.01; Figure 4). In contrast to TNC, levels of proinflammatory cytokine IL-6 were many times higher in SF (range 865–1063 pg/ml) compared to paired serum (range 3–272 pg/ml; Figure 4, right panel). The levels of TNC and IL-6 did not correlate in the SF.
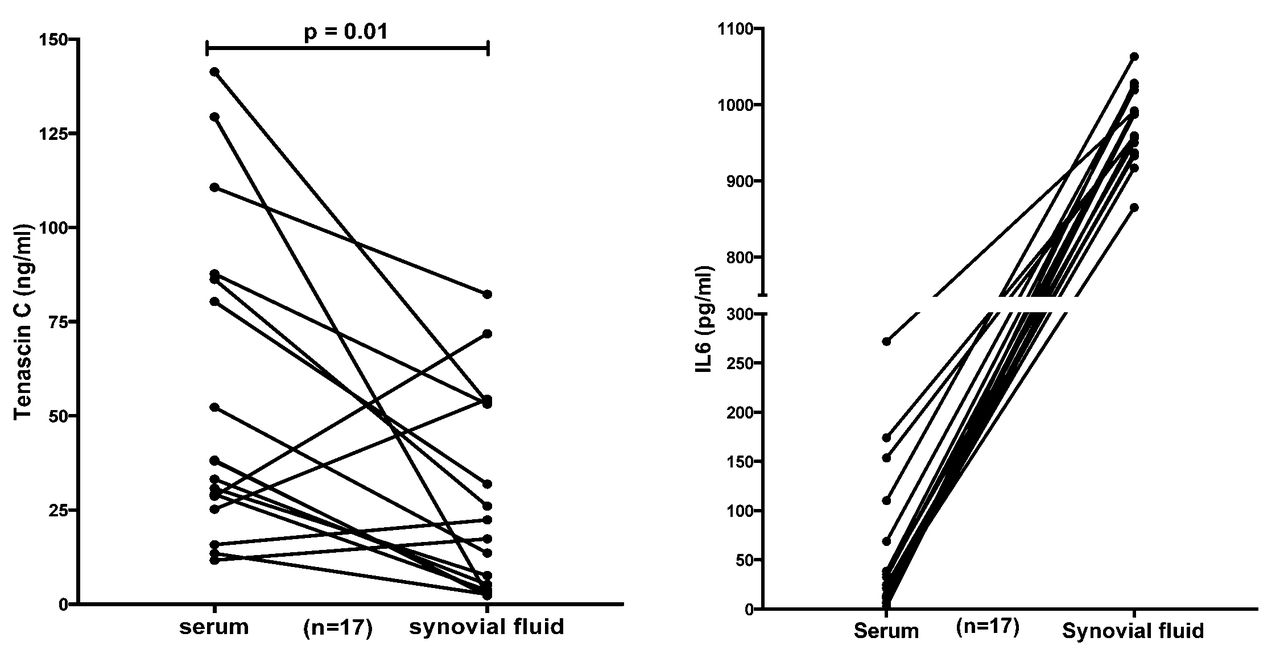
Tenascin-C levels in paired serum-synovial fluid of children with JIA-ERA (left panel). IL-6 levels in paired serum-synovial fluid of children with JIA-ERA (right panel). JIA: juvenile idiopathic arthritis; ERA: enthesitis-related arthritis; IL-6: interleukin 6.
DISCUSSION
JIA-ERA is a disease characterized by sustained joint and entheseal site inflammation in the absence of known infectious agents or exact autoimmune triggering factors. It has similarities with AS and a family history of SpA is often positive. An interaction between HLA-B27, TLR on monocytes, and their ligands appears to play a predominant role in a sterile chronic inflammatory state. In our study, we found that circulating levels of TNC, a TLR4 ligand, are raised in children with JIA-ERA, and correlate with clinical and laboratory variables of disease activity. As a marker of disease activity, it was comparable to ESR and CRP. The levels in HLA-B27–positive children were higher than those in HLA-B27–negative children with JIA-ERA. The children with JIA-ERA, similar to patients with AS, show a high response to full-dose NSAID treatment. Regular NSAID therapy leads to control of disease activity and a fall in circulating TNC levels at the end of 3 months.
We found raised levels of circulating TNC in children with JIA-ERA. High serum TNC levels are shown in adults with inflammatory arthritis such as RA, AS, psoriatic arthritis, and systemic lupus erythematosus12. Rise in serum levels has been demonstrated with pathological inflammation and tissue remodeling in diseases such as ulcerative colitis14, Crohn disease14, and idiopathic inflammatory myositis12. Thus, increased serum levels are not specific to childhood arthritis, but are more related to a systemic inflammatory state.
The serum levels were significantly higher in HLA-B27–positive compared to HLA-B27–negative children. Though the HLA-B27–negative children seemed to have lower disease activity, these differences were not statistically significant except for the duration of EMS. HLA-B27–positive patients are known to have more severe and prolonged joint symptoms15. It is possible that unfolded HLA-B27 heavy chains induce endoplasmic reticulum stress that causes the activation of the nuclear factor-κB pathway and leads to increases in TNC expression by myeloid cells4,9. Because we had a small number of HLA-B27–negative children, these data need to be validated in a larger cohort.
The circulating levels in JIA-ERA correlated moderately with various clinical and laboratory variables of disease activity, and ROC analysis showed AUC comparable to ESR and CRP. The serum level of TNC in inflammatory bowel disease (IBD) correlates with clinical and histological measures of activity. It has been proposed as a marker for monitoring relapse in patients with IBD14. In patients with RA, no correlation was found with any of the clinical or laboratory activity markers. Page, et al demonstrated a correlation with ultrasound erosions of metacarpophalangeal joints suggestive of an association with damage rather than activity12. We found no correlation with DJC and a negative correlation with the duration of disease, a surrogate marker of damage. However, the pathogenesis of RA is quite different from that of JIA-ERA or IBD; in those 2 diseases, gut inflammation mediated by microbes is thought to play an important role.
There was a significant fall in serum TNC levels in children with JIA-ERA receiving regular and full doses of NSAID. This finding reflects the fall in TNC level that comes with control of disease activity. In patients with RA, a fall in serum TNC level was observed with infliximab therapy, while there was no change with MTX treatment. Page, et al found a correlation with baseline high TNC levels and unresolved joint tenderness despite infliximab therapy12. Levels in patients with IBD showed a significant fall after restorative surgeries and correlated with disease activity on conservative treatment14. TNC serum levels in cross-sectional analysis did not differ based on the treatment being given: MTX, low-dose steroid, or on-demand NSAID. This may be because they had an active disease despite the treatment. Treatment with regular and full-dose NSAID therapy controlled the disease activity and resulted in the fall. In a study that included patients with RA, serum TNC levels did not show any changes with MTX therapy12.
Paired SF levels were much lower compared to serum levels and did not correlate with levels of IL-6, a proinflammatory cytokine in SF. SF TNC has been studied in RA and osteoarthritis (OA)16,17,18. RA SF levels were found to be 4-fold higher than in patients with OA and did not correlate with serum CRP levels16. The TNC levels of OA samples were about 5-fold higher than the control values and showed an association with radiographic disease progression17,18. Paired serum-SF level studies are not available in patients with RA and OA. The TNC SF levels in children with JIA-ERA were lower than those shown in patients with RA and OA; this may be because of the nonerosive nature of inflammation in SpA, particularly in children. The SF was mainly tapped from acutely inflamed joints for intraarticular injections and there was no documented radiographic damage in the injected joints. Consumption of SF TNC in an acute inflammatory state or decreased release of TNC from the extracellular matrix in the absence of erosions or damage may explain the lower levels seen in the SF of children with ERA.
This raises the question of the source of raised serum TNC in JIA-ERA. TNC is produced by myeloid cells in the extracellular matrix at sites of inflammation8. In various chronic inflammatory diseases, its expression increases at sites such as the intestinal mucosa in IBD19, synovium in RA9,16, and hypertrophic synovium in OA20. In JIA-ERA, the chronic inflammation occurs at 3 sites: synovium, entheses, and to some extent in the intestinal mucosa. Thus, it is possible that any or all of these 3 sites contribute to raise serum levels. However, a tissue analysis to assess the expression of TNC would help to confirm its source in JIA-ERA.
Our study has shown high serum values of the endogenous TLR4 ligand TNC that correlate moderately with various clinical and laboratory measures of disease activity. Regular NSAID therapy leads to a fall in TNC levels as a reflection of controlling disease activity. TNC is not specific for JIA-ERA and may indicate a degree of inflammation, as do ESR and CRP, but along with the previous observation of increased TLR4 expression on monocytes6, these findings support that TNC may play a role in augmenting the process of inflammation in JIA-ERA. In addition to activity, relation with HLA-B27 positivity may suggest a synergistic interaction between these 2 important pathogenic pathways (TNC-TLR4 pathway and unfolded HLA-B27-cytokine pathway), leading to a state of chronic joint inflammation. Further, in vitro work on the myeloid cells of patients with JIA-ERA might help to validate this hypothesis.
Footnotes
-
Supported by a research grant to Prof. Aggarwal.
- Accepted for publication January 16, 2015.








{kind=link}
{kind=link}
{kind=link}
{kind=link}