

Abstract
Objective. Our study aimed to evaluate the longterm efficacy and safety of abatacept (ABA), and to explore factors that increase its longterm efficacy in patients with rheumatoid arthritis (RA) treated in routine clinical practice.
Methods. There were 231 participants with RA treated with ABA who were prospectively registered in a Japanese multicenter registry. They were followed up for at least 52 weeks.
Results. Mean age of the patients was 64.3 years, mean disease duration was 12.1 years, mean 28-joint Disease Activity Score (DAS28)-C-reactive protein was 4.49, and 48.5% of patients were concomitantly treated with methotrexate (MTX). Overall retention rate of ABA was 77.1% at 52 weeks; 14.8% of patients discontinued because of inadequate response and 3.5% because of adverse events. The proportion of patients achieving DAS28-defined low disease activity (LDA) significantly increased from baseline to 52 weeks (7.3% to 43.8%, p < 0.01); 40.9% of patients who did not achieve LDA at 24 weeks had more than 1 categorical improvement in DAS28-defined disease activity at 52 weeks. Multivariate logistic regression revealed concomitant MTX use to be an independent predictor of the categorical improvement in DAS28-defined disease activity from 24 to 52 weeks (adjusted OR 3.124, p = 0.010).
Conclusion. In routine clinical practice, ABA demonstrated satisfactory clinical efficacy and safety in patients with established RA for 52 weeks. The clinical efficacy of ABA increased with time even after 24 weeks, and this was strongly influenced by concomitant MTX use. Our study provides valuable real-world findings on the longterm management of RA with ABA.
Rheumatoid arthritis (RA) is a chronic and systemic autoimmune inflammatory disease that clinically manifests as joint pain and swelling1. Persistent inflammation without sufficient treatment can lead to cartilage damage, bone erosion, joint destruction, and subsequent longterm disability. Methotrexate (MTX) and biological disease-modifying antirheumatic drugs (DMARD) offer an avenue for improving RA treatment. The most recently published strategy, the 2013 European League Against Rheumatism (EULAR) recommendation update, suggests adjusting the therapeutic strategy if no improvement is observed by, at most, 3 months after the initiation of treatment or if the target outcome has not been achieved by 6 months2.
Abatacept (ABA) is the first member of a new class of biological DMARD for RA that inhibits T cell activation by binding to CD80/86, thereby modulating the CD80/86-CD28 interaction. The efficacy and safety of ABA has been reported in several randomized controlled clinical trials (RCT)3,4,5. Although short-term clinical results of ABA treatment in clinical practice have also been reported in Denmark, France, and Japan6,7,8,9,10, only a few reports have addressed longterm clinical results6. Because the treatment of RA is typically a longterm endeavor, it is particularly important to accumulate longterm clinical data for drugs currently in clinical practice, i.e., in the “real-world setting.” Since patients included in RCT undergo strict selection, data from patients treated in routine clinical practice would provide an additional dimension of insight that could supplement RCT results.
We previously reported that the achievement of low disease activity (LDA) at 52 weeks could be predicted using a 28-joint Disease Activity Score (DAS28) cutoff at 12 weeks after ABA therapy11, and that this strategy comports with the 2013 EULAR recommendation update. However, in clinical practice, some patients who improve somewhat wish to continue ABA treatment, even if they fail to achieve the clinical target (e.g., LDA) at 6 months. Thus, insight into the expected course of ABA efficacy after 6 months would be informative. Phase III RCT have shown an increase in the proportion of patients who achieved LDA from half a year to 1 year after ABA treatment as follows: from 30.0% to 42.5% (Abatacept in Inadequate Responders to Methotrexate; AIM trial)5, 20.7% to 35.3% (Abatacept or infliximab vs placebo, a Trial for Tolerability, Efficacy and Safety in Treating rheumatoid arthritis; ATTEST trial)12, and 18.3% to 24.2% (Abatacept Trial in Treatment of Anti-tumor necrosis factor Inadequate Responders; ATTAIN trial)13. If an enhancement in ABA efficacy after 6 months can be truly expected in clinical practice, continuous ABA therapy would likely be beneficial to patients who wish to continue, as well as those who have few options left after ABA.
Against this backdrop, our study aimed to (1) provide longterm clinical efficacy and safety data in routine clinical practice, and (2) provide evidence of enhanced clinical efficacy of ABA after 24 weeks using prospective observational data from a multicenter registry of patients with RA treated with biological DMARD.
MATERIALS AND METHODS
Participants
All eligible patients were registered in and followed by the Tsurumai Biologics Communication Registry (TBCR)14. TBCR was initiated in October 2008 to study the longterm efficacy and safety of biologics used to treat RA. Data were collected retrospectively from 2003 to 2008 and prospectively after 2008. Patient characteristics and disease activity data are available for all patients with RA treated with commercially available biologics at TBCR institutes in Japan. Registered data [e.g., drug continuation, reasons for switching drugs, and adverse events (AE) that resulted in stopping biologics treatment] are updated once a year.
Our present study included all patients who started intravenous (IV) ABA treatment and were prospectively observed for longer than 52 weeks at TBCR-affiliated institutes (n = 254). All patients met the 1987 American College of Rheumatology classification criteria for RA. Patients received IV ABA 3 times at 2-week intervals, and thereafter at 4-week intervals. Patients received a fixed dose of ABA at about 10 mg/kg body weight; patients weighing < 60 kg received 500 mg of ABA, those weighing 60–100 kg received 750 mg, and those weighing > 100 kg received 1000 mg. Patient anonymity was maintained during data collection, and security of personal information was strictly controlled. This study was approved by the Nagoya University Graduate School of Medicine Ethics Committee.
Data collection
Demographic data recorded at the initiation of treatment (baseline, Week 0) included age, sex, disease duration, rheumatoid factor positivity (≥ 20 IU/ml), history of previous treatment with biological DMARD, and concomitant treatment (MTX or prednisolone). Pulmonary comorbidities [interstitial pneumonia (IP), chronic obstructive pulmonary disease (COPD), tuberculosis (TB), or history of serious infection] based on reports from attending physicians were recorded. Bilateral hand radiographs were used to classify the severity of peripheral joint destruction into Steinbrocker classification stages I–IV15. The following disease variables were recorded at baseline and after 4, 12, 24, and 52 weeks of treatment: tender joint count and swollen joint count at 28 joints, patient’s and physician’s global assessment of disease activity, modified Health Assessment Questionnaire score, serum C-reactive protein (CRP) levels, and matrix metalloproteinase 3 levels. Disease activity was evaluated at each timepoint by DAS28-CRP.
The DAS28-CRP is known to significantly underestimate disease activity and overestimate improvement in disease activity compared to the DAS28-erythrocyte sedimentation rate (ESR)16. In our present study, we used criteria that differed from those of DAS28-ESR. Disease activity was categorized as follows: DAS28-CRP remission (REM; DAS28-CRP < 2.3), LDA (2.3 ≤ DAS28-CRP < 2.7), moderate disease activity (MDA; 2.7 ≤ DAS28-CRP ≤ 4.1), and high disease activity (HDA; DAS28-CRP > 4.1). These criteria have been validated in a large Japanese cohort study17.
Statistical analysis
Demographic and disease characteristics are reported using descriptive statistics. All results are expressed as mean ± SD or a percentage. Student t test was used for 2-group comparisons, and the chi-square test for categorical variables. The last observation carried forward method was used in each analysis.
Multivariate analysis (logistic regression) was performed to identify factors that predict improvement of DAS28-CRP from weeks 24 to 52. Variables were considered for the multivariate models if their univariate p value was less than 0.20, with the exception of sex and age, which were included in all models. Adjusted OR with 95% CI were calculated after adjusting for age and sex.
All statistical tests were 2-sided, and p < 0.05 was considered significant. All analyses were performed with SPSS version 20.0.0 software (IBM Corp.).
RESULTS
Demographic data
A total of 254 patients were enrolled in our study; 23 were excluded because of incomplete data, giving a final total of 231 patients (mean age 64.3 yrs, mean disease duration 12.1 yrs) through October 2013. Table 1 summarizes general, clinical, and disease activity-related characteristics of all analyzed patients. Of the 231 patients, 164 (71.0%) were categorized into advanced Steinbrocker stages (III and IV), indicating established RA and joint damage. Disease activity was high, as reflected by a mean DAS28-CRP score of 4.49 and a mean CRP level of 2.3 mg/dl. MTX was concomitantly used in 48.5% of patients. One hundred thirteen patients (48.9%) had been previously treated with anti-tumor necrosis factor (TNF) and/or anti-interleukin 6 receptor biological DMARD, and 47 patients (20.3%) had a history of treatment with multiple biological DMARD. A total of 33 patients (14.3%) had pulmonary comorbidities at baseline, including 25 cases of IP, 6 cases of COPD, 6 cases of TB, and 2 cases with a history of serious infection. Five of the 6 cases with TB were pre- and comedicated with isoniazid and ABA therapy.
Baseline characteristics of patients with RA who received ABA therapy. Values are mean ± SD unless otherwise specified.
Overall clinical efficacy of ABA treatment
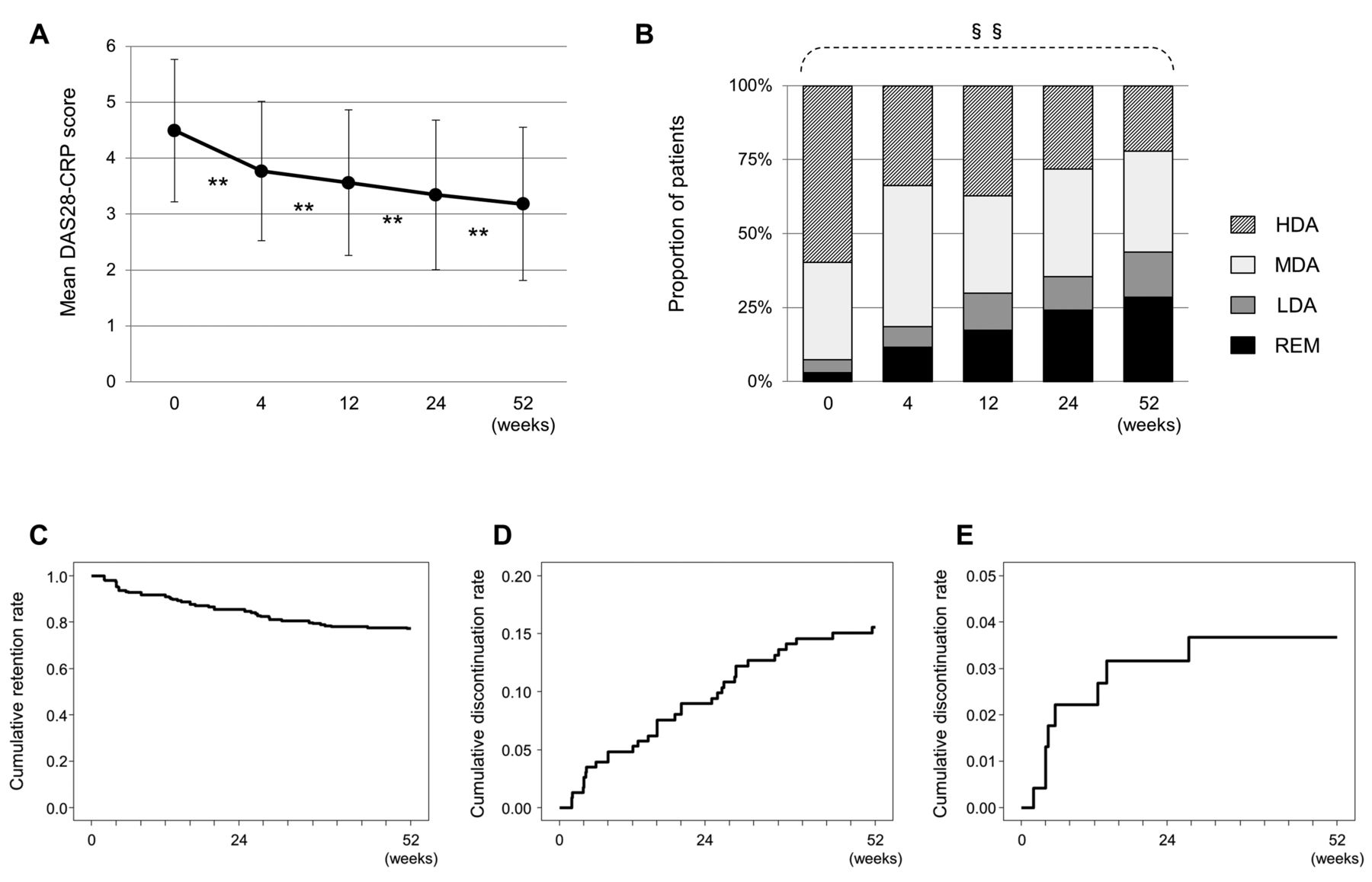
As shown in Figure 1A, the mean DAS28-CRP score significantly decreased from 4.49 ± 1.27 at baseline to 3.77 ± 1.24 at Week 4, 3.56 ± 1.30 at Week 12, 3.34 ± 1.34 at Week 24, and 3.18 ± 1.34 at Week 52 (p < 0.01). Interestingly, the mean DAS28-CRP score significantly decreased from Week 24 to Week 52, as well as from Week 4 to Week 12, and Week 12 to Week 24. The categorical distribution of disease activity status defined by DAS28-CRP is shown in Figure 1B. The proportion of patients who achieved LDA or REM significantly increased from baseline to 52 weeks (LDA 7.3% to 43.8%, REM 3.0% to 28.6%, p < 0.01, Cochran-Armitage trend test). Moreover, the proportion of patients with HDA significantly decreased from 59.7% at baseline to 22.1% at 52 weeks (p < 0.01).

Overall clinical efficacy of ABA in patients with RA over the course of 52 weeks. A. Mean and SD of DAS28-CRP. B. Changes in DAS28-CRP-defined categorical disease activity. C. Drug retention rate with an endpoint of all unfavorable causes. D. Drug discontinuation rate because of inadequate response to endpoint. E. Drug discontinuation rate because of adverse events. ** p < 0.01 in paired Student t test. §§ p < 0.01 in Cochran-Armitage trend test. ABA: abatacept; RA: rheumatoid arthritis; HDA: high disease activity; MDA: moderate disease activity; LDA: low disease activity; REM: clinical remission; DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein.
Patient retention and safety of ABA treatment
Over the course of 52 weeks, 53 patients withdrew from treatment with ABA. The retention rate was 77.1%, as estimated by Kaplan-Meier analysis (Figure 1C). The most frequent reason for discontinuation was inadequate response (34 patients, 14.8%; Figure 1D). There were 8 patients (3.5%) who stopped ABA treatment because of AE (Figure 1E). The remaining 11 patients (4.8%) discontinued ABA for other reasons (e.g., transfer to another hospital, patient’s desire, pregnancy, or economic issue).
Eight patients discontinued ABA therapy because of AE. One had facial flushing at 14 days, 1 had purpura at 28 days, 1 had appendicitis at 28 days, 1 had MTX-related lymphoproliferative disorder at 31 days, 1 had malignant lymphoma at 39 days, 1 had simultaneous interstitial pneumonia and organizing pneumonia at 88 days, 1 had interstitial pneumonia at 98 days, and 1 had palpitations at 193 days. There was only 1 patient who stopped ABA because of AE after 24 weeks. Most severe AE were observed within 24 weeks and the incidence plateaued after 24 weeks, while discontinuation because of inadequate response linearly increased even after 24 weeks. Both of the 2 cases of lymphoproliferative disorder recovered after stopping ABA and MTX without undergoing chemotherapy (including rituximab).
Change in DAS28-CRP score after 24 weeks in patients who failed to achieve LDA at 24 weeks
We studied changes in disease activity after 24 weeks in patients who failed to achieve LDA even at 24 weeks, but who continued ABA treatment to 52 weeks. Eleven of 121 patients (9.1%) with MDA or HDA at 24 weeks discontinued ABA treatment before 52 weeks; 10 patients (8.3%) discontinued because of inadequate response, no patient because of an adverse event, and 1 patient (0.8%) because of other reasons.
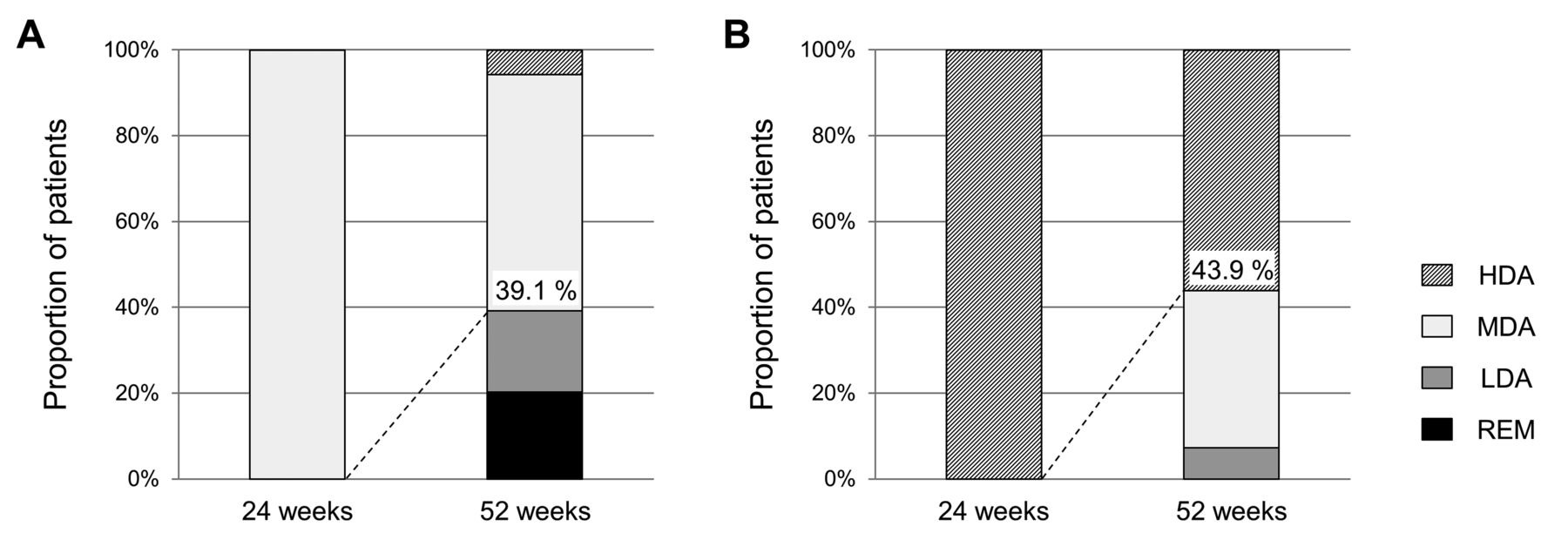
The remaining 110 patients with MDA or HDA at 24 weeks who continued ABA to 52 weeks were further examined. The second column of Table 2 summarizes their characteristics at 24 weeks. Mean DAS28-CRP score significantly decreased from baseline (4.74 ± 1.13) to 24 weeks (3.88 ± 0.92) and from 24 weeks to 52 weeks (3.48 ± 1.11). Forty-five patients (40.9%) achieved “DAS28 categorical improvement” (more than 1 categorical improvement from 24 to 52 weeks, e.g., HDA at 24 weeks to MDA, LDA, or REM at 52 weeks). Twenty-seven patients (39.1%) with MDA at 24 weeks and 18 with HDA at 24 weeks (43.9%) achieved DAS28 categorical improvement at 52 weeks (Figures 2A and 2B).
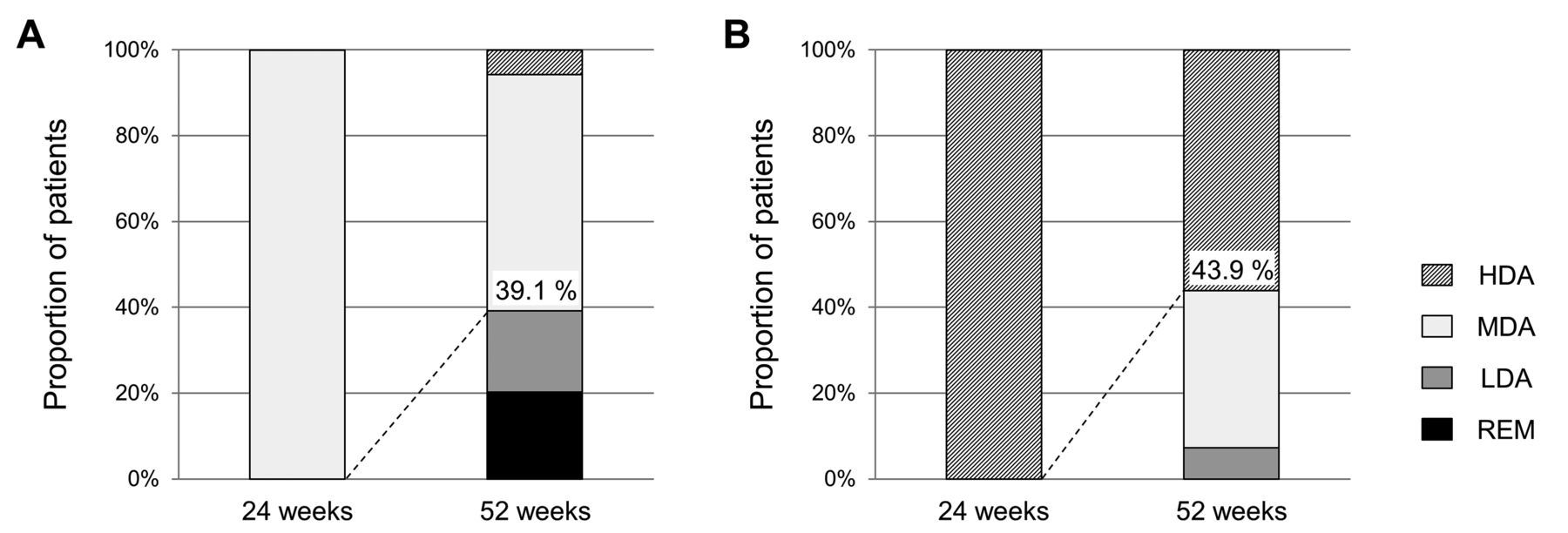
Change in DAS28-CRP-defined categorical disease activity from 24 to 52 weeks of ABA treatment in patients who failed to achieve LDA at 24 weeks. A. Change in disease activity in patients with MDA at 24 weeks. B. Change in disease activity in patients with HDA at 24 weeks. DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein; ABA: abatacept; LDA: low disease activity; MDA: moderate disease activity; HDA: high disease activity; REM: clinical remission.
Characteristics of patients who did not achieve LDA at 24 weeks. Values are mean ± SD unless otherwise specified.
Factors predicting achievement of DAS28 categorical improvement from 24 to 52 weeks
Univariate analysis and multivariate logistic regression were performed to identify predictors of DAS28 categorical improvement at 52 weeks. Univariate logistic regression revealed that only concomitant MTX use was associated with achievement of DAS28 categorical improvement at 52 weeks (Figure 3). Multivariate logistic regression revealed that concomitant MTX use was independently associated with achievement of DAS28 categorical improvement at 52 weeks (Figure 3).
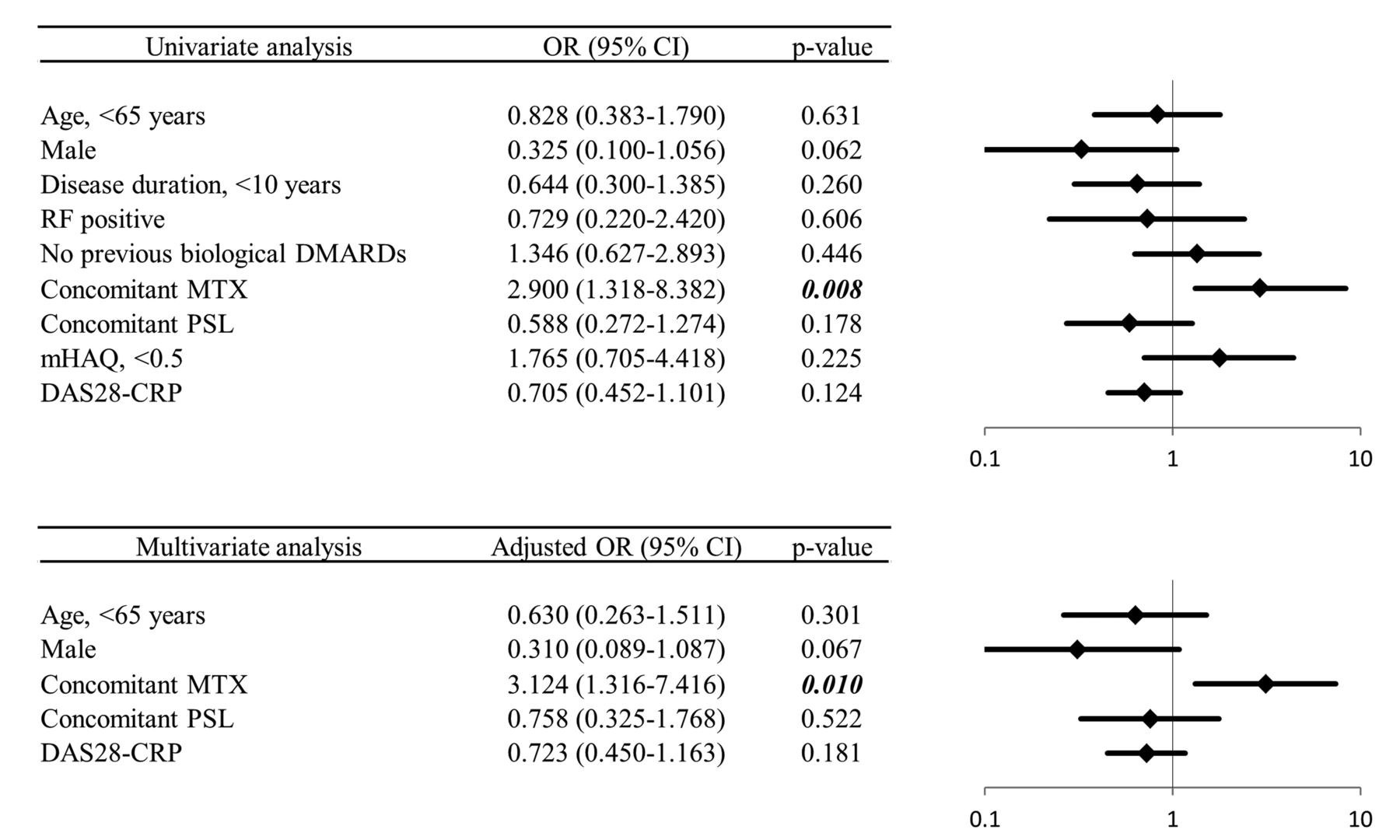
Factors predicting the achievement of DAS28-CRP-defined categorical disease activity improvement from 24 to 52 weeks. Upper panel: univariate logistic regression analysis. Lower panel: multivariate logistic regression analysis. DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein; RF: rheumatoid factor; DMARD: disease-modifying antirheumatic drugs; MTX: methotrexate; PSL: prednisolone; mHAQ: modified Health Assessment Questionnaire.
Comparison of DAS28-CRP scores between patients with and without concomitant MTX use among patients who failed to achieve LDA at 24 weeks
Table 2 summarizes the characteristics at 24 weeks of patients with and without concomitant MTX use who failed to achieve LDA at 24 weeks, but continued ABA to 52 weeks. A significantly higher proportion of pulmonary comorbidity was observed in those without concomitant MTX use. Otherwise, there were no other significant differences, including all disease activity indices.
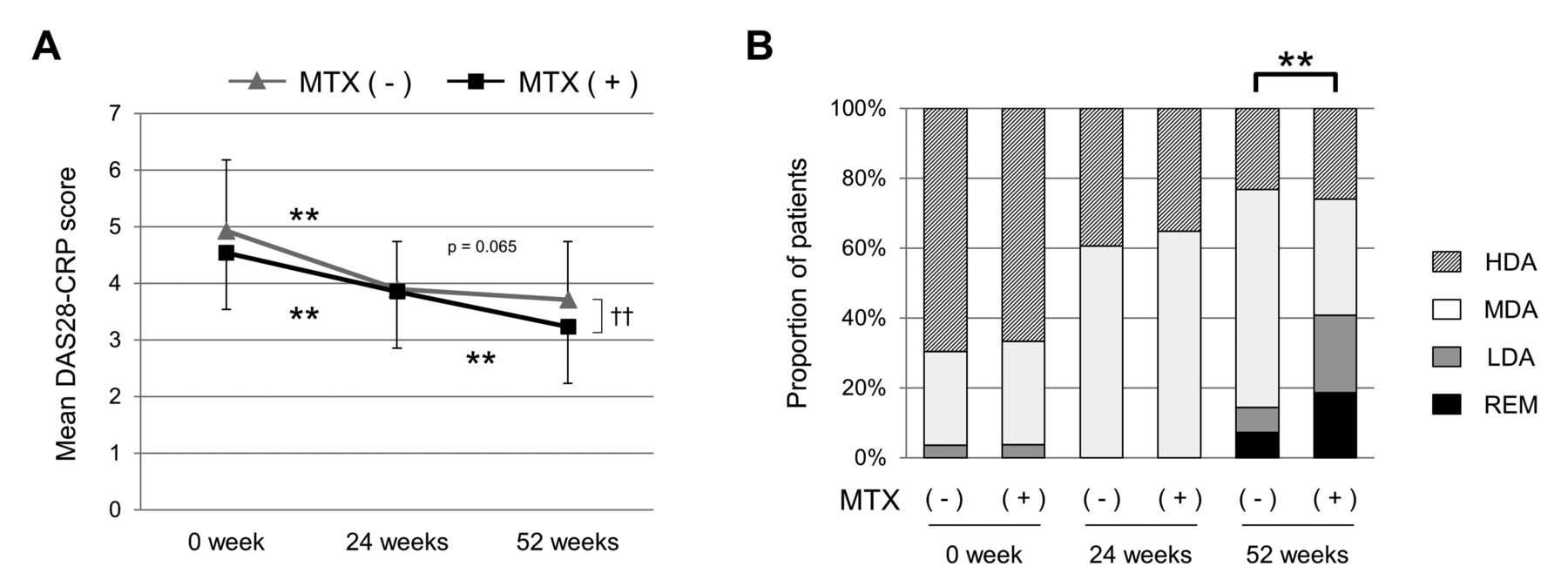
Figure 4A shows changes in mean DAS28-CRP score. Mean DAS28-CRP score significantly decreased in patients with concomitant MTX use from 24 weeks (3.86 ± 0.99) to 52 weeks (3.24 ± 1.15). Among those without concomitant MTX use, the mean DAS28-CRP score did not significantly decrease from 24 weeks (3.90 ± 0.84) to 52 weeks (3.71 ± 1.03), although a decreasing trend was observed (p = 0.065). The categorical distribution of DAS28-CRP scores is shown in Figure 4B. There was no significant difference between patients with and without concomitant MTX use at baseline and 24 weeks. The proportion of patients who achieved LDA at 52 weeks was significantly higher in patients with concomitant MTX use (40.7%) compared to those without (14.3%; p < 0.002). There was no significant difference in the proportion of patients who achieved REM at 52 weeks between those with (18.5%) and without (7.1%) concomitant MTX use (p = 0.074).

Comparison of ABA efficacy between patients treated with and without concomitant MTX among those who failed to achieve LDA at 24 weeks. A. Change in mean and SD of DAS28-CRP. B. Change in DAS28-CRP-defined categorical disease activity. ** (A) p < 0.01 in paired Student t test. †† p < 0.01 in unpaired Student t test. ** (B) p < 0.01, comparing the proportion of patients achieving LDA (Pearson chi-square test). ABA: abatacept; MTX: methotrexate; LDA: low disease activity; DAS28: 28-joint Disease Activity Score; CRP: C-reactive protein; HDA: high disease activity; MDA: moderate disease activity; REM: clinical remission.
DISCUSSION
In our study, we provided longterm clinical data relating to ABA treatment in patients with RA treated in routine clinical practice using data from a multicenter registry. These data demonstrated the satisfactory efficacy and safety profile of ABA for up to 52 weeks. A significant therapeutic response was observed within 4 weeks and gradually increased to 52 weeks. Importantly, clinical efficacy significantly increased even after 24 weeks in patients with concomitant MTX use.
We found that the longterm clinical efficacy and safety of ABA in routine clinical practice are comparable to those reported in RCT. The proportions of patients who achieved LDA in our study (35.5% at 24 weeks and 43.8% at 52 weeks) were comparable to those reported in 2 RCT involving patients with active RA despite concomitant MTX use: the AIM trial (30.0% and 42.5%, respectively)5 and ATTEST trial (20.7% and 35.3%, respectively)12, as well as the ATTAIN trial involving patients with active RA despite TNF inhibitor use (18.3% and 24.2%, respectively)13. Our data also support the longterm safety and tolerability of ABA in clinical practice. Discontinuation rates because of AE were 3.2% at 24 weeks and 3.7% at 52 weeks, with only 1 patient discontinuing after 24 weeks. This suggests the lack of a correlation between longer exposure to ABA and frequency of severe AE. Importantly, the discontinuation rate because of AE in our study is comparable to those reported in RCT: 4.2% at 1 year in the AIM trial5, 5.8% at 1 year in the ATTEST trial12, 3.9% at 0.5 year in the ATTAIN trial12, and 3.4% at 1 year in the AGREE trial (Abatacept trial to Gauge Remission and joint damage progression in methotrexate-naive patients with Early Erosive rheumatoid arthritis)18. Collectively, our results suggest the safety and efficacy of ABA in routine clinical practice, providing a real-world view across patients with various backgrounds. Our results are comparable with those reported in RCT, which involve stringently selected patients.
A number of studies have reported on the short-term clinical efficacy of ABA monotherapy. Indeed, we previously reported that ABA monotherapy had comparable clinical efficacy with ABA in combination with MTX therapy for 24 weeks8. The ORA (Orencia and Rheumatoid Arthritis) registry, a French nationwide cohort study for investigating the longterm safety and efficacy of ABA for treating RA, reported that concomitant treatment with MTX was not an independent predicting factor for achieving EULAR response at 6 months7. In the ARRIVE trial (Abatacept Researched in RA patients with an Inadequate anti-TNF response to Validate Effectiveness), 43 patients received ABA monotherapy, and its efficacy was comparable to that when using background DMARD for 24 weeks19. Further, changes in DAS28-CRP scores were similar with and without concomitant MTX use from baseline to 24 weeks (data not shown). Interestingly, concomitant MTX has little effect on the short-term clinical efficacy of tocilizumab, another class of non-anti-TNF agent20, whereas background MTX therapy is needed to maximize the clinical efficacy of anti-TNF agents21,22. These results appear to suggest that concomitant MTX would do little to improve the short-term clinical efficacy of biologics in patients treated with non-anti-TNF agents. When choosing a class of biologics, an important consideration is whether the patient is currently treated with MTX. In the present study, only 48.5% of patients were treated with concomitant MTX. Interestingly, the French ORA registry also reported less frequent use of concomitant MTX (49%)7. Our study population and that of the ORA registry were distinct from patients involved in controlled trials. Indeed, we believe our population more accurately represents the major population being treated with ABA in real-world settings.
We also found that a significantly higher proportion of patients who were not treated with concomitant MTX had pulmonary comorbidities. When a patient is considered intolerant to MTX, one of the major factors we would look into is the existence of pulmonary comorbidities, including IP and COPD. In such patients, we try to avoid the use of MTX, given its signature lung toxicity23. Instead, we prefer using non-anti-TNF agents with the hope that a good therapeutic effect, at least in the short term, can be achieved without MTX use. This is likely the reason that those treated with MTX had a lower proportion of pulmonary comorbidities. However, no study to date has assessed the longterm effects of concomitant MTX use on ABA efficacy.
To our knowledge, this is the first report to demonstrate that concomitant MTX enhances the longterm clinical efficacy of ABA after 24 weeks in routine clinical practice; a similar tendency was observed in several RCT5,12,13. The most recently published strategy is the 2013 EULAR recommendation update that suggests a therapy should be adjusted if the target has not been achieved by 6 months2. In the present study, 64.5% of patients failed to achieve the target outcome (i.e., LDA) at 6 months. When indicated and possible, we recommend to our patients a switch from ABA to another agent. However, patients with some clinical improvement (but not sufficient improvement to achieve LDA) within 6 months may wish to continue ABA therapy. In other cases, there may be no choice but to continue ABA treatment if no reasonable alternative exists. Nevertheless, gaining insight into the expected course of clinical efficacy of ABA after 24 weeks would be highly informative. Our findings suggest that concomitant MTX use increases the clinical efficacy of ABA after 24 weeks in patients who failed to achieve LDA at 24 weeks. Although it might be possible for some patients undergoing ABA monotherapy to achieve LDA within 24 weeks, for those who do not reach this goal, longterm ABA treatment with concomitant MTX should be considered.
In the AVERT study (Assessing Very Early Rheumatoid arthritis Treatment), Emery, et al recently reported the tendency of superior clinical response of subcutaneous (SC) ABA plus MTX treatment compared to SC ABA monotherapy, even in the short term, in MTX-naive patients with early RA24. Although concomitant MTX had no effect on the short-term clinical response of ABA in patients with established RA in our study, it is possible that concomitant MTX may augment the short-term clinical efficacy of ABA in some specific populations (e.g., those with early disease or those who are MTX-naive). Further studies are warranted, aimed at identifying the specific patient group that may benefit from concomitant MTX to obtain a quick and satisfactory clinical response to ABA.
Our study has several limitations. First, given the retrospective observational setting, a future prospective study would be necessary to make conclusions regarding the effect of concomitant MTX on longterm ABA efficacy. Second, the Steinbrocker stage classification may have been underestimated in our patients, because these classifications were based on reports from attending physicians and no data were available on when the radiographs used for evaluation were taken relative to participant entry into our study. Third, sequential radiographic data were not available. Given the importance of joint protective effects in demonstrating clinical efficacy, evaluating radiographic changes in patients treated with ABA will be necessary in the future. Finally, our findings were based on the use of IV ABA. However, the use of a new SC formulation is now widespread and further studies will be necessary to determine whether our results also apply to SC ABA.
In routine clinical practice, ABA demonstrated satisfactory clinical efficacy and safety in patients with established RA at 52 weeks. Clinical efficacy of ABA increased with time even after 24 weeks, which was strongly influenced by concomitant MTX use. Although further detailed studies on safety are needed, our study provides valuable real-world findings on the longterm management of patients with RA treated with ABA.
Acknowledgment
We thank Dr. Toshihisa Kanamono (Department of Orthopedic Surgery, Nagano Red Cross Hospital, Nagano, Japan), Dr. Yukiyoshi Oh-ishi (Department of Rheumatology, Toyohashi Municipal Hospital, Toyohashi, Japan), Dr. Naoki Fukaya (Department of Orthopedic Surgery, Kariya–Toyota General Hospital, Kariya, Japan), and Dr. Seiji Tsuboi (Department of Orthopedic Surgery, Shizuoka Kosei Hospital, Shizuoka, Japan) for their kind suggestions.
- Accepted for publication January 23, 2015.








{kind=link}
{kind=link}
{kind=link}
{kind=link}