

Abstract
Objective. To identify modifiable patient and provider factors associated with allopurinol adherence and the achievement of a serum urate acid (SUA) goal in gout.
Methods. We identified a retrospective cohort of patients with gout, newly treated with allopurinol. All patient data came from administrative datasets at a large integrated health delivery system. Patients were ≥ 18 years old at time of initial allopurinol dispensing, and had 12 months or more of membership and drug eligibility prior to the index date. Allopurinol adherence was defined as a proportion of days covered ≥ 0.80, evaluated during the first 12 months of observation after the initial dispensing. Multivariable logistic regression was used to examine factors associated with allopurinol nonadherence and attaining an SUA concentration < 6.0 mg/dl.
Results. We identified 13,341 patients with gout with incident allopurinol use (mean age 60 yrs, 78% men). Of these, 9581 patients (72%) had SUA measured both at baseline and during followup. Only 3078 patients (32%) attained an SUA target of < 6.0 mg/dl during followup. Potentially modifiable factors associated with treatment adherence and obtaining the SUA goal in the multivariable analysis included concomitant diuretic use, prescriber specialty, and allopurinol dosing practices. Adherent patients were 2.5-fold more likely than nonadherent patients to achieve an SUA < 6.0 mg/dl during observation.
Conclusion. Among patients with gout initiating allopurinol in our study, 68% did not reach the SUA goal and 57% of patients were nonadherent. Modifiable factors, including allopurinol dose escalation, treatment adherence, rheumatology referral, and concomitant medication use, could be important factors to consider in efforts aimed at optimizing gout treatment outcomes.
Given the central role of hyperuricemia in the etiology of gout, urate-lowering therapy (ULT) has become the corner-stone treatment in chronic gout. A serum urate (SUA) level of < 6.0 mg/dl has been widely accepted as the therapeutic target for patients with gout. It is the primary endpoint in randomized controlled trials1,2,3,4 and has been endorsed by all internationally recognized, evidence-based gout management guidelines to date5,6,7,8. Each of the published guidelines includes a treat-to-target strategy with gradual ULT titration until SUA levels reach < 6.0 mg/dl (or < 5.0 mg/dl in select circumstances). Studies have consistently demonstrated improvements in longterm patient outcomes after achieving a target SUA < 6.0, including reduction in flares1,2,3,4,9,10, reduction in tophus size1,4,10, and depletion of urate stores in synovial tissues10.
Available for more than 40 years, allopurinol remains the most frequently prescribed ULT in all studies examining practice patterns in gout management11,12,13,14, accounting for 97% of ULT prescriptions in at least 1 study12. Allopurinol can be dosed once daily, is inexpensive, and is potentially effective and well tolerated in a vast majority of patients with gout.
Despite its many advantages as a ULT, numerous studies have indicated poor patient adherence to allopurinol therapy11,12,13,14,15,16,17. In addition to medication adherence, quality of care in gout is far from optimal17,18,19,20,21 and a limited number of prior studies have examined the direct link between ULT adherence and SUA goal achievement. None have simultaneously accounted for the many confounders that could affect this relationship. The primary objective of our study was to examine potentially modifiable patient and provider factors associated with allopurinol adherence and SUA goal attainment among patients with gout initiating allopurinol treatment. Our goal from our study was to provide some basis for prioritization of factors amenable to future quality improvement initiatives focused on gout outcomes.
MATERIALS AND METHODS
Setting and dataset
We examined data from Kaiser Permanente Southern California (KPSC), a large integrated healthcare delivery system with about 3.6 million members. Available administrative data included patient demographics, diagnoses, medication dispensing, laboratory results, and medical and hospital encounters. KPSC had no known policies that would have directly affected the type of care provided to patients with gout during the time of our study. Specifically, there were no restrictions or other disincentives for providers with regards to specialist referral or use of non-allopurinol ULT in patients with gout. The health system membership currently represents 15% of the underlying population in the Southern California region and closely mirrors the area’s demographic characteristics; it is racially diverse and includes the entire socioeconomic spectrum22. The KPSC institutional review board approved our study.
Design and study population
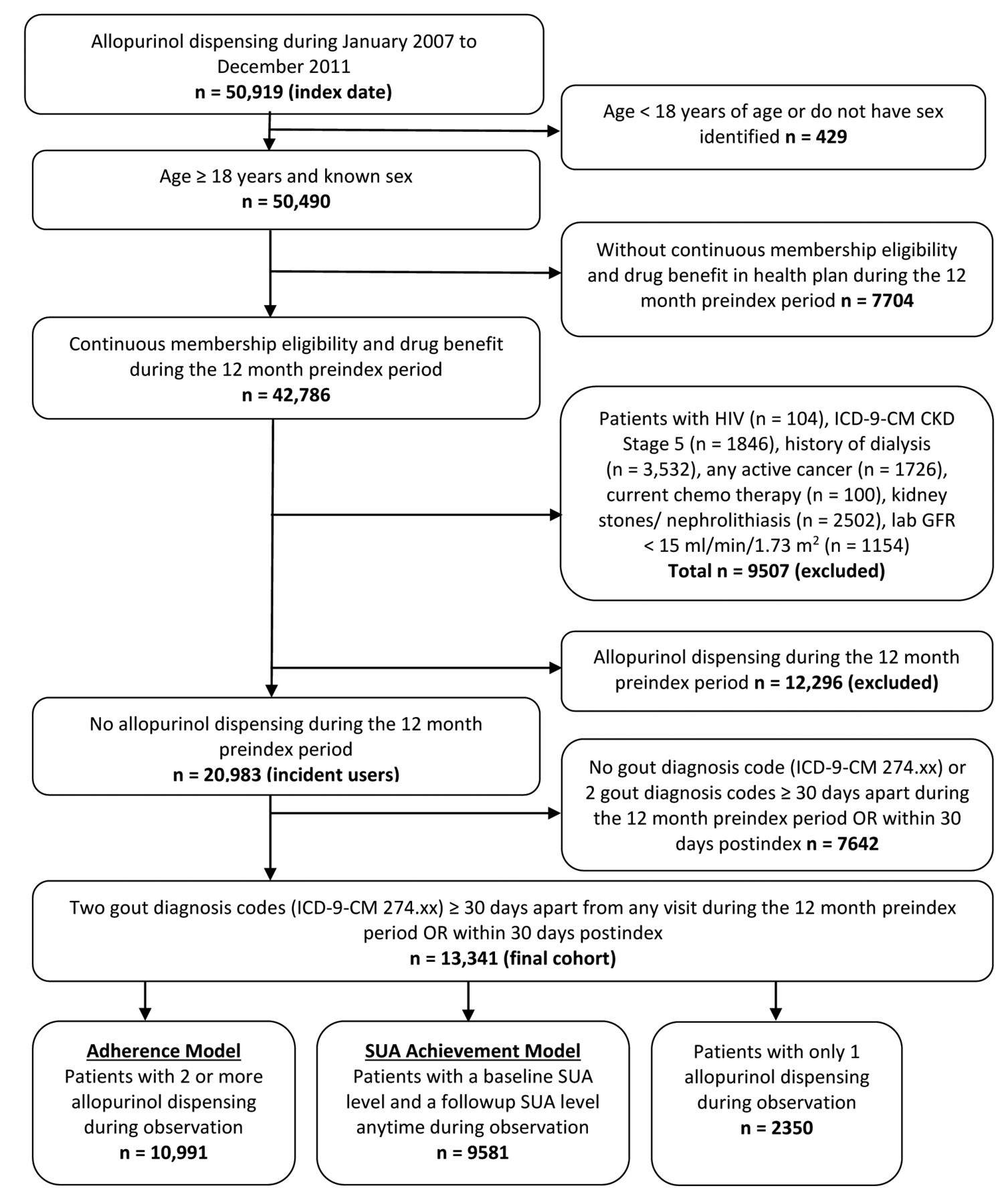
A retrospective cohort database analysis was conducted for the study enrollment period of January 1, 2007, through December 31, 2011. Patients were selected if they received a new allopurinol dispensing during the study enrollment period, were ≥ 18 years of age at the time of initial allopurinol dispensing during the study period, and had at least 12 months of membership eligibility including drug benefits prior to the initial allopurinol dispensing. Enrollment gaps of ≤ 30 days were considered continuous enrollment. The index date was defined as the first allopurinol dispensing identified during the study enrollment period. Eligible patients were required to have 2 gout diagnoses ≥ 30 days apart coded at any outpatient or inpatient visit during the 12-month preindex period and extending to 30 days postindex (International Classification of Diseases-9-Clinical Modification code 274.xx). Patients were excluded if, during the preindex period, they had an allopurinol prescription, history of human immunodeficiency virus, a diagnosis code for chronic kidney disease (CKD) stage 5 or an estimated glomerular filtration rate (eGFR) < 15 ml/min/1.73 m2, a history of dialysis, active cancer or currently receiving chemotherapy, or kidney stones/nephrolithiasis. Each exclusion criterion was included to limit the patient population to those whose primary indication for allopurinol was gout. Patients were followed from index allopurinol dispensing until disenrollment from the health plan or the end of the study period (December 31, 2012), whichever came first (Figure 1). This observation period provided a minimum of 12 months for followup after the index allopurinol dispensing.
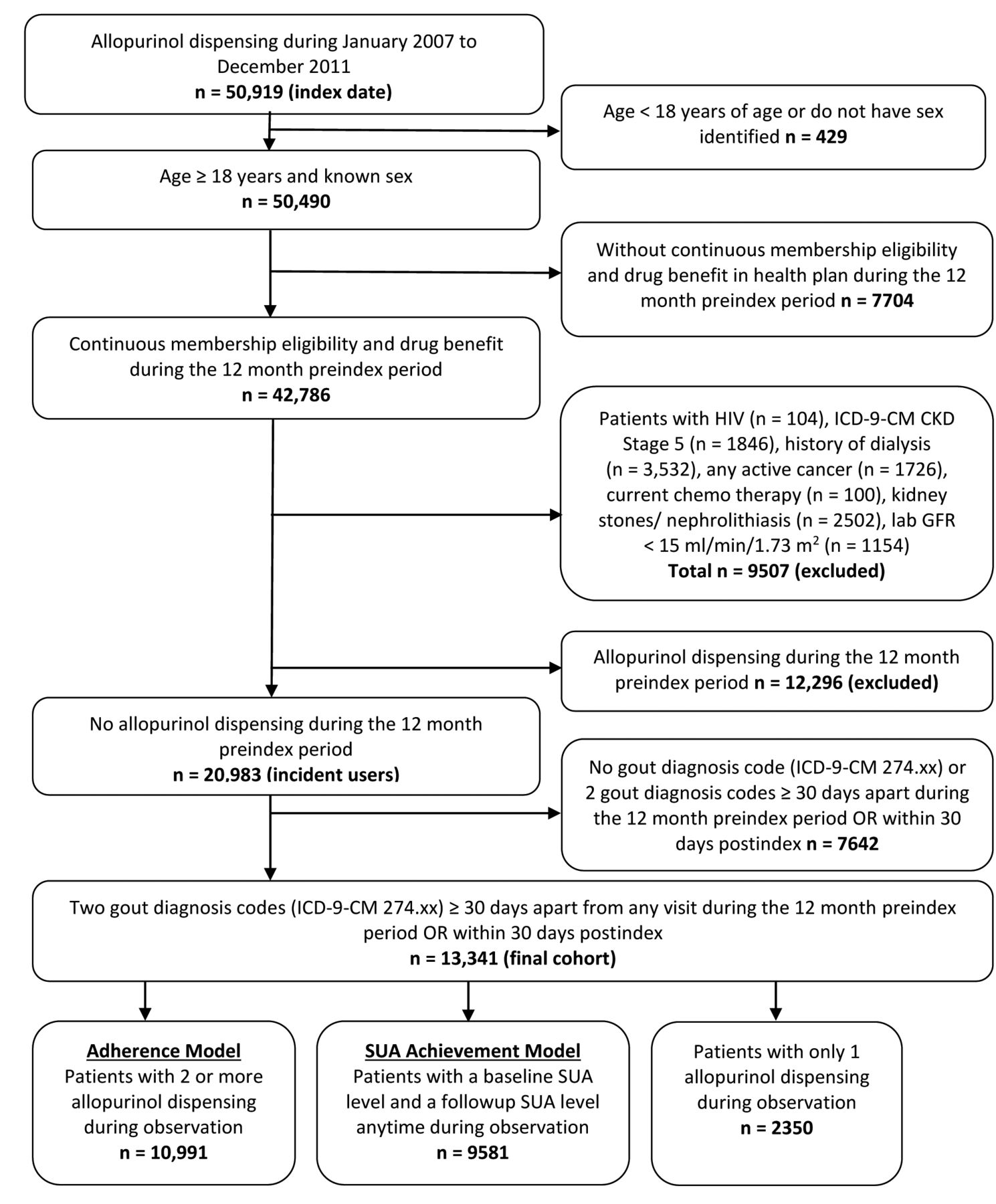
Sample selection flowchart. HIV: human immunodeficiency virus; ICD-9-CM: International Classification of Diseases-9-Clinical Modification; CKD: chronic kidney disease; GFR: glomerular filtration rate; SUA: serum urate.
Covariates and measures
Baseline characteristics such as age, sex, race, comorbid conditions, concomitant medication use, renal function, and prescriber specialty were evaluated 12 months prior to and including the index date. Prescription antiinflammatory medication use [defined throughout as nonsteroidal antiinflammatory drugs (NSAID), colchicine, or glucocorticoids] was evaluated over the 60-day period spanning 30 days preindex and 30 days postindex. Baseline SUA levels were measured up to 12 months prior to the index date or within 30 days after the index date. For a majority of patients (82%), a baseline SUA level was obtained at least once during the 12-month period prior to the index date, and 18% had an SUA level obtained only during the 30-day postindex period. For those patients with multiple potential baseline SUA values available, the measurement obtained most proximate to the index date was used. Allopurinol treatment information (changes in dose), adherence, and the SUA goal attainment were identified postindex. Patients were considered to have had allopurinol dose escalation if the final observed daily dose was greater than the index dose. Conversely, patients were considered to have had dose decreases if the final daily allopurinol dose was less than the initial dose.
Adherence measure
Medication adherence was summarized using proportion of days covered (PDC). The PDC was calculated as the number of days with allopurinol drug on hand divided by the number of days in the specified time interval (360 days). We evaluated the PDC within the first 12 months of initiating allopurinol. A uniform period of 360 days, representing four 90-day allopurinol dispensings, was used in our calculation to ensure comparable and sufficient data to characterize longterm adherence behavior profiles for all patients. The 90-day period represents the most common number of days supplied for an allopurinol dispensing. The PDC was dichotomized for the multivariable analysis, with a PDC of < 80% considered nonadherent and ≥ 80% considered adherent11,12,14,15. We first calculated the PDC for all patients including those receiving only a single allopurinol dispensing. To limit the effect of immediate discontinuation, we also calculated the PDC for patients with gout receiving 2 or more allopurinol dispensings during the 12-month postindex period. Given its rare incidence (estimated at about 1 in 1000 patient-yrs, based on external literature) and imprecision in its identification, we did not examine the effect of severe cutaneous reactions (e.g., Stevens-Johnson syndrome) on allopurinol adherence or outcomes23.
Attainment of the treatment goal
Attainment of the SUA goal was achieved if the last followup SUA level obtained more than 30 days after the index date had a value < 6.0 mg/dl. By this definition, a patient would not be considered to have attained the SUA goal if the final observed SUA was ≥ 6.0 mg/dl even if any prior SUA level more than 30 days after index was < 6.0 mg/dl. This outcome was evaluated only among patients that had both baseline and followup SUA levels available. Taking into account the 30-day buffer period, all patients had at least 11 months or longer of followup during which an SUA level could be recorded.
Statistical analyses
Unadjusted descriptive statistics summarized patient characteristics of the study population, patients who were adherent versus nonadherent, and patients at SUA goal versus not at SUA goal. Two models were developed using the same dataset, one model for the nonadherence outcome and a second for the SUA goal achievement outcome. Each model had a different population subset created from the final cohort as shown in Figure 1. Differences between groups were tested using the 2-sided Student t test for continuous variables and the chi-square test for categorical variables. Multivariable logistic regression models were used to evaluate the association of factors, selected a priori, with nonadherence (PDC of < 80%) and the achievement of an SUA level < 6.0 mg/dl. Factors including age, sex, race, selected comorbid conditions (hypertension, myocardial infarction, congestive heart failure, and diabetes), diuretic use, renal function (by eGFR), care by rheumatologist, antiinflammatory medications, and treatment adherence (only for the model examining SUA goal achievement) were controlled for in the models. Based on the strong association between initial prescribing physician (rheumatologist vs non-rheumatologist) and dose adjustment (no change vs dose escalation vs dose decrease), multivariable models include initial prescribing physician instead of dose adjustment. All data were analyzed using SAS version 9.2 (SAS Institute). P values < 0.05 were considered statistically significant.
RESULTS
Patient population
There were 13,341 patients with gout identified as incident allopurinol users (mean age 60 yrs, men 78%) using our selection criteria (Figure 1). Table 1 summarizes baseline characteristics of incident allopurinol users. Patients were predominantly white (41%), and the most common comorbidities were hypertension (71%) and diabetes (23%). The mean baseline GFR was 63.5 ml/min (SD ± 18.5) with a majority of patients categorized into either CKD stage 2 (46%, eGFR 60–89 ml/min) or CKD stage 3 (38%, eGFR 30–59 ml/min). Considering concomitant medications, 39% of patients were treated with either a thiazide or loop diuretic, and 69% of patients used a prescription antiinflammatory medication (colchicine, NSAID, or glucocorticoid) within the period covering 30 days preindex to 30 days postindex. A majority (87%) of the patients had at least 1 SUA level in the baseline period (mean SUA 8.58 mg/dl, SD ± 1.8 mg/dl).
Baseline patient characteristics for new allopurinol users.
Table 2 summarizes prescriber specialty, allopurinol initial dose and changes in dose, treatment adherence, and SUA levels during followup. Over 80% of physicians who prescribed the index allopurinol were primary care physicians while 6% were rheumatologists. A majority of the patients started allopurinol at a dose of either 100 mg per day (48%) or 300 mg per day (37%). Based on pharmacy claims data, 82% of patients continued with 2 or more allopurinol dispensings with a mean duration of allopurinol therapy of 2.6 years (SD ± 1.6). Of these, less than 2% (n = 202) switched to febuxostat during the 360-day followup. Among the remaining patients (18%) who received only a single allopurinol dispensing, the mean duration of therapy was 93 ± 21 days. Allopurinol doses were not changed for a majority of patients (71%) throughout observation; only 22% had a dose increase from their initial dispensing (Table 2). The mean PDC was 65% (SD ± 23.2%), and for evaluating patients with 2 or more dispensings (n = 10,991), the mean PDC was slightly higher at 74% (SD ± 21.4%). Of patients with gout with both baseline and followup SUA measurements available (n = 9581), 75% had their last followup SUA obtained more than 1 year postindex (Table 2).
Treatment information and related outcomes for new allopurinol users. Values are n (%) unless otherwise specified.
Allopurinol prescribing practices in rheumatologists and non-rheumatologists
In an additional analysis comparing rheumatology to non-rheumatology prescribers, there were striking differences in allopurinol use. Among patients with gout treated by a rheumatologist, 98% received allopurinol dose escalation during their care compared to just 5% of those treated by non-rheumatologists (p < 0.0001). Overall, only 11% of patients received a dose escalation. Rheumatologists were also more likely than non-rheumatologists to initiate allopurinol in daily doses of 100 mg or less (64% vs 48%, p < 0.0001). Although more common in the context of rheumatology care, an ending daily dose of allopurinol > 300 mg/day was uncommon for both rheumatologists and non-rheumatologists (6.3% vs 2.0%, p < 0.0001).
Factors associated with allopurinol adherence and serum urate goal attainment
Adherence was measured in the subgroup of patients who had at least 2 or more allopurinol dispensings during 12 months postindex (n = 10,991, 82% of total). Of these, 4656 patients (42%) were adherent with a PDC ≥ 80% over the first year of allopurinol use (Table 3). In unadjusted analyses, factors significantly associated with allopurinol nonadherence included male sex, younger age, minority racial/ethnic status, the absence of select comorbid conditions, lower eGFR, higher initial allopurinol doses, a non-rheumatology prescriber, a lack of diuretic use, and the use of antiinflammatory drugs (Table 3).
Unadjusted comparisons of patient characteristics for new allopurinol users stratified by adherence.
Among patients with gout with both a baseline and a followup SUA level available (n = 9581, 72% of total), about 1 in 3 patients (32%) attained an SUA level < 6.0 mg/dl (Table 4). Unadjusted comparisons showed that these factors were more common among patients failing to achieve a target SUA level < 6.0 mg/dl: male sex, younger age (< 65 yrs), minority race/ethnicity, congestive heart failure, higher GFR, the use of antiinflammatory agents, non-rheumatologist prescribers, lower initial allopurinol doses (≤ 100 mg/day), and lower treatment adherence (Table 4).
Unadjusted comparisons of patient characteristics for new allopurinol users stratified by SUA goal versus not at SUA goal. All values are n (%) unless specified otherwise.
Using multivariable analyses, we subsequently identified factors that were independently associated with allopurinol nonadherence and the achievement of SUA goal (Table 5). For the multivariable nonadherence model, male sex was no longer significantly associated with nonadherence, and allopurinol dose escalation was removed from the model because of high collinearity with the rheumatologist as the initial prescriber. All other significant associations from unadjusted analysis remained for the multivariable model of nonadherence.
Factors associated with nonadherence to allopurinol and SUA goal attainment from logistic multivariable regression in new allopurinol users. Values are OR (95% CI).
DISCUSSION
It has been widely reported that quality of care for gout is suboptimal17,18,19,20,21. It has also been demonstrated that medication adherence in gout is exceedingly low11,12,13,14,15,17, ranking among the lowest observed of several chronic health conditions examined16. In addition to supporting these earlier studies, our study identifies several modifiable factors associated with treatment adherence and outcomes in gout. To our knowledge, ours is the first study to demonstrate an independent and strong association of allopurinol treatment adherence with SUA goal achievement after accounting for a rich array of confounding factors using a large generalizable population. Among the many patient and provider factors examined, allopurinol treatment adherence was the single strongest determinant of achieving SUA goal over followup with a corresponding OR exceeding 2.5.
Quality improvement initiatives routinely target at-risk patient populations and our results indicate that a similar strategy may be considered in gout management. We found, for instance, that younger patients, males, and individuals reporting minority race/ethnicity may be at an increased risk of nonadherence, even after adjustment for factors including comorbidities and CKD21. Frequent comorbidity and polypharmacy in gout have drawn concerns that patient complexity may be an impediment to optimal care24. However, as reported elsewhere11,12,13,15, we found that select comorbidities were associated with greater medication adherence. We also report a novel observation that current diuretic use is associated with greater allopurinol adherence. It is possible that patients with more comorbidities and concomitant medications such as diuretics have developed more effective self-management behaviors. It is noteworthy that diuretic use also increases urate retention, which may explain the simultaneously observed lower odds of SUA goal attainment among diuretic users.
Our study re-emphasizes the important association of more advanced CKD with lower SUA goal attainment21 and extends the association to lower medication adherence. While residual confounding cannot be excluded with certainty, it is well known that CKD complicates the prescription of NSAID and colchicine for acute gout treatment and antiinflammatory prophylaxis. If CKD limits effective prophylaxis, then resulting “rebound” flares may discourage ULT adherence. Although not examined in our study, both qualitative and retrospective cohort studies have demonstrated a detrimental effect of flares on medication use11,25,26. Advanced CKD further limits SUA goal attainment in 2 ways. Higher serum urate levels are associated with more advanced CKD because uric acid removal is dependent on renal excretion. Moreover, dose titration may not occur owing to inappropriately rigid adherence to previous renal dosing recommendations27,28 that have been refuted in recent studies and evidence-based guidelines5,6,7,29,30.
Provider prescribing practices also appear to influence treatment adherence and outcomes in gout. A rheumatologist as the initial prescriber was significantly associated with improved allopurinol adherence and SUA goal attainment after adjusting for medication adherence, among other factors. Allopurinol dose escalation was very common among rheumatologists, but was extremely uncommon among other providers. It is well accepted that dose escalation is required for most patients to achieve SUA goal, including those with CKD29. Our analysis suggests that dose escalation may help to explain the associations observed between provider specialty and SUA goal attainment.
Starting allopurinol dose and antiinflammatory prophylaxis are increasingly important considerations for prescribing providers. Therefore, our results require careful review. In adjusted analysis, initial allopurinol doses above 100 mg/day were associated simultaneously with greater SUA goal attainment and decreased adherence. This could indicate that higher dose allopurinol is associated with a higher risk of gout attacks, which might result in patients prematurely discontinuing ULT. Indeed, randomized controlled trials (RCT) have demonstrated that higher flare rates correspond with high dropout rates because of flares among users of higher-dose febuxostat1,2,3,4. Likewise, a limited posthoc analysis of multiple RCT indicated that a lower SUA after beginning treatment was significantly associated with the occurrence of flares31. We showed that when adjusting for adherence, a higher dose increased the likelihood of achieving SUA goal. This should not be construed to indicate that a higher starting dose is optimal. Instead, a low starting dose with escalation appeared to balance the benefits of increased allopurinol adherence with the ultimate need for higher doses to achieve SUA goal. Antiinflammatory prophylaxis was unexpectedly associated with decreased allopurinol adherence. However, in the experience of the authors, some patients prefer to treat their gout acutely, and broad access to antiinflammatory medications, including over-the-counter preparations, may actually discourage patients’ adherence to longterm therapeutic options. There are other potential reasons that together might help to explain our results regarding starting dose and prescription antiinflammatory prophylaxis.
Our study has strengths that distinguish it from prior efforts. For instance, we examined only incident allopurinol use by requiring no previous dispensings in the 12-month preindex period. Inclusion of prevalent users in other studies likely overestimates medication adherence11,13,14,21. Additionally, poor adherence or treatment discontinuation among patients with gout may lead to misclassification of patients as incident allopurinol users in studies requiring shorter preindex eligibility periods12,17. We were able to further validate our measure of medication adherence given its close and independent association with SUA goal achievement, while several prior investigations failed to explore this important relationship11,12,13,15. Among the 3 previous studies examining factors associated with SUA goal attainment, 2 did not examine the role of ULT adherence17,21 and the third reported only a crude association between allopurinol adherence and SUA goal attainment stratified by time period14.
Despite its significant strengths, our study also has limitations. Recognizing the diagnostic uncertainty with reliance on administrative data, we attempted to limit misclassification bias by requiring a gout diagnosis, incident allopurinol dispensing, and exclusion of other potential reasons for allopurinol use. Gout severity could not be addressed in our analysis, limiting understanding of differential case mix among specialties. Our analysis also did not incorporate any measure of flares. While a limitation, flares often go unreported to the medical system and attempts to measure flares in the medical records are prone to significant underreporting. Finally, our study represents a large cohort from an integrated healthcare delivery system. While the findings of poor quality of care are broadly reported, the relative importance of different factors represented in our models may not universally apply to other healthcare systems.
Subpopulations of patients with gout are at heightened risk for ULT nonadherence and failure to attain SUA goal. At-risk populations should be targeted for interventions to improve medication adherence and promote appropriate ULT dose titration. Our study demonstrates an unmet need for improvement in gout care and identifies potential factors to target.
Footnotes
-
Supported by a grant from the US National Institutes of Health (NIH)/National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) 1P50AR060772-01A1. Dr. Curtis is supported by the Agency for Healthcare Research and Quality (R01HS018517) and the NIH (AR060772).
- Accepted for publication October 23, 2014.








{kind=link}