

Abstract
Objective. To investigate the probable pathogenesis, clinical features, diagnosis, and therapy of patients with pulmonary hypertension (PH) in Takayasu arteritis (TA).
Methods. A total of 48 patients with TA who had PH, 20 patients with TA who had pulmonary arterial involvement (PA) without PH, and 30 patients with idiopathic pulmonary arterial hypertension (IPAH) were enrolled in the study from 2009 to 2013.
Results. Among the 48 patients with TA who had PH, 36 (75.0%) had PA, and left heart disease (LHD) was present in 12 (25.0%). Serum levels of big endothelin 1 (ET-1) were independently correlated with pulmonary arterial systolic pressure (r = 0.33, p = 0.04). Compared to patients with IPAH, patients with PH because of PA who underwent right heart catheterization had lower average cardiac indexes (2.0 ± 0.5 vs 3.0 ± 1.2 l/min/m2, p = 0.05), and they all developed favorable responses to acute vasodilator testing (100%) in comparison to 10 of the patients with IPAH (33.3%). During a mean followup of 36.0 ± 13.2 months (12.0–65.0 mos), of the patients with PH associated with PA, 3 died of heart failure. Six patients who underwent pulmonary artery revascularization were found to have good prognoses after followup for a mean duration of 6.2 ± 1.9 months. Additionally, 12 patients with PH with LHD were followed for 38.4 ± 15.6 months (12.0–60.0 mos), and 1 patient died of heart failure during the followup period.
Conclusion. Patients with TA are at increased risk for PH. Early screening of patients with TA with unexplained symptoms related to PH should be applied. PH-specific therapies or revascularization may be effective treatments in the early stages of patients with PA, PH, and severe pulmonary artery stenosis.
Takayasu arteritis (TA) is a systemic inflammatory disease involving the aorta and its main branches, resulting in luminal stenosis and aneurysmal changes in the large vessels1,2.
Involvement of pulmonary arteries with the development of pulmonary hypertension (PH) is a rare condition in the course of TA3,4,5,6. The rate of PH in patients with TA is about 12%–13% in various reports7,8. PH is a life-threatening complication itself, perhaps even more serious in the context of underlying vasculitis. Pulmonary manifestations of PH associated with TA are not specific and may be masked by the involvement of other large vessels4,5. In light of the poor prognosis of PH and the fairly frequent involvement of the pulmonary arteries in TA4, it is important to describe the clinical presentation of this rare condition.
Our current series included 48 patients with TA with PH, 20 patients with TA with pulmonary arterial involvement (PA) without PH, and 30 patients with idiopathic pulmonary arterial hypertension (IPAH). We aimed to characterize the clinical, laboratory, and imaging data from the patients, and to discuss the potential possibility of diagnosis and therapy of this rare condition.
MATERIALS AND METHODS
Patients and methods
The clinical data were assessed of 48 patients with TA with PH, 20 patients with TA who had PA without PH, and 30 patients with IPAH hospitalized at Fuwai Hospital from 2009 to 2013. Medical records including clinical, laboratory, angiographic, imaging, and echocardiographic data were analyzed retrospectively. The study protocol was approved by the Fuwai Hospital ethics committee. All of the patients with TA satisfied the 1990 American College of Rheumatology criteria9, which fulfilled at least 3 of the following: an age at disease onset ≤ 40 years, claudication of the extremities, a decreased brachial artery pressure, a blood pressure difference between both arms ≥ 10 mmHg, bruit over the subclavian arteries or aorta, and abnormalities on arteriography. PH was defined as a mean pulmonary arterial pressure (mPAP) of > 25 mmHg at rest by right heart catheterization (RHC)10 or estimated pulmonary arterial systolic pressure (PASP) exceeding 40 mmHg by echocardiography in patients without RHC11. PH was categorized as severe if the PASP was > 65 mmHg, moderate if 55–64 mmHg, and mild if 40–54 mmHg11. All of the patients were classified as New York Heart Association (NYHA) functional class II to IV.
Blood electrolytes were measured using the ion-selective electrode technique (UniCel DxC 800, Beckman Coulter Inc.). Erythrocyte sedimentation rate (ESR) and plasma C-reactive protein (CRP) were detected with Westergren method (Vacuette SRS100, Greiner Bio-One) and immunoturbidimetry (Immage 800, Beckman Coulter Inc.), respectively. Measurements of arterial blood gases were performed using a blood-gas analyzer (Radiometer). The levels of big endothelin 1 (ET-1) were measured using an ELISA kit (ELx800 Absorbance Reader, BioTek Instruments Inc.). N-terminal probrain natriuretic peptide (NT-proBNP) levels were measured using the electrochemiluminescence immunoassay (Cobas E601, Roche Diagnotics).
The pulmonary vasculature was evaluated using various imaging modalities: computerized tomography (CT), echocardiography, and pneumoangiography. The CT obstruction index was used to quantify the obstructive degree of pulmonary arteries with CT. The CT obstruction index can be expressed as:
 where n is the value of the proximal obstruction in the pulmonary arterial tree equal to the number of segmental branches arising distally (minimum 1, maximum 20), and d is the degree of obstruction (minimum 0, maximum 2)12. All spiral CT images were systematically read during the course of clinical workup by senior radiologists. Each imaging examination was reinterpreted by consensus between 2 chest radiologists who were blinded to both echocardiographic and clinical data. Similarly, in the echocardiography studies, all echocardiography studies were systematically read by senior sonologists, and each examination was reinterpreted by consensus between 2 sonologists who were blinded to the patient’s diagnosis and clinical data.
where n is the value of the proximal obstruction in the pulmonary arterial tree equal to the number of segmental branches arising distally (minimum 1, maximum 20), and d is the degree of obstruction (minimum 0, maximum 2)12. All spiral CT images were systematically read during the course of clinical workup by senior radiologists. Each imaging examination was reinterpreted by consensus between 2 chest radiologists who were blinded to both echocardiographic and clinical data. Similarly, in the echocardiography studies, all echocardiography studies were systematically read by senior sonologists, and each examination was reinterpreted by consensus between 2 sonologists who were blinded to the patient’s diagnosis and clinical data.
Of the 78 patients with PH included in the study, 25 of 30 patients with IPAH and 30 of 48 patients because of PA underwent cardiopulmonary exercise testing, and peak oxygen uptake (peak VO2) was measured during exercise. RHC was performed according to standard procedures in all 30 patients with IPAH and in 12 patients with PH who had PA. Baseline hemodynamic variables were measured, including right atrial pressures, pulmonary arterial pressures, pulmonary vascular resistance (PVR), pulmonary to systemic flow, mixed venous oxygen saturation, cardiac output, and cardiac index. Vasoreactivity testing was performed at the time of diagnostic RHC to identify patients who could benefit from longterm therapy with calcium channel blockers (CCB). A significant acute response to iloprost was defined as a fall in both mPAP and PVR of at least 20% relative to the baseline value13.
Statistical analysis
Mean levels of variables were compared by ANOVA, and the chi-square test was used for categorical variables. Comparisons between each combination of 2 groups were conducted using the Student-Newman-Keuls test. The associations between 2 different variables were examined using Pearson correlation analysis after adjusting for age, body mass index, and other related confounding factors. A p value < 0.05 using a 2-sided test was considered statistically significant. All statistical analyses were conducted with the SPSS 19.0 statistical package (IBM SPSS Inc.).
RESULTS
Among the 48 patients with TA who had PH included in this series, the female-to-male ratio was 7:1, and the average age was 43.5 ± 13.5 years (18–60 yrs). Thirty-six patients (75.0%) had PA [including 4 patients with PA (8.3%) with in situ thrombus formation]. Left heart disease (LHD) was the cause of PH in 12 patients (25.0%). Patients with PA-related PH tended to present at a younger age than patients with PH due to LHD; the mean age of the patients with PA was 39.2 years compared to 48.2 years for patients with LHD. Clinical characteristics and laboratory variables are described in detail in Table 1.
Clinical characteristics of patients with PH in TA and patients with IPAH. Values are mean ± SD or % unless otherwise specified.
Clinical characteristics
In 36 patients with PH because of PA, PA was an initial presenting feature of TA in 30 patients, and the mean duration from the onset of symptoms to the diagnosis of PH was 31.0 months (6–96 mos). Clinical symptoms presented mainly as dyspnea on exertion (n = 30), hemoptysis (n = 13), and central cyanosis (n = 6). Leg edema (n = 20) and pericardial effusion (n = 6) were late symptoms. Two patients had symptoms of coronary involvement, and another 6 patients with PA developed the signs of systemic vasculature damage typical for TA as the initial symptoms. These clinical manifestations included hypertension (HTN; n = 5), pulseless disease (n = 3), and dizziness or syncope (n = 1). The mean duration from the onset of symptoms of TA to diagnosis of PH was 12.3 ± 4.8 years (6–20 yrs). The mean age for patients with systemic signs of TA and vascular signs other than PA was significantly lower at diagnosis of TA than those patients who presented initially with PA as the first sign of TA (28.6 ± 4.8 vs 35.4 ± 8.6 yrs, p = 0.03).
In 10 of the 12 patients with PH due to LHD, systemic signs of TA were the main presenting feature, and the clinical manifestations of these patients were stated as follows: HTN (n = 9), pulseless disease (n = 6), and dizziness or syncope (n = 5). The other 2 patients with PH due to LHD demonstrated symptoms of PH as the initial symptoms, and the intervals from the onset of symptoms to the diagnosis of PH were 12 and 18 months, respectively.
All 48 patients with TA who had PH and 20 patients with PA without PH were treated with glucocorticoids (prednisone). The mean dose of prednisone was 18.6 mg in patients with PH because of PA and 24.2 mg for patients with PH because of LHD. No other immunosuppressive agents or biologics were used in treating any of the patients. The treatment of patients with PH associated with PA included the following: sodium ferulate, a traditional Chinese medicine widely used in the treatment of cardiovascular or cerebrovascular diseases or PH (n = 36); a diuretic agent (n = 36); digoxin (n = 30); aspirin (n = 28); and warfarin (n = 8). In addition, 10 patients with PH with PA and who had positive responses to vasoreactivity testing were treated with CCB. Seven patients with PH with PA were treated with PH-specific therapies (bosentan or sildenafil) after diagnosis by severe mPAP (mPAP > 60 mmHg) measured by RHC, and all these 7 patients noted improvements in their PH-related symptoms. The treatment of patients with PH because of LHD included a diuretic agent (n = 12), aspirin (n = 12), β blockers (n = 10), and angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blocker (ARB; n = 7); none of the patients were treated with warfarin or PH-targeted drugs. In addition, 6 of the patients with PH who had PA underwent pulmonary artery stent implantation. All received aspirin therapy prior to the stent implantation and a combination of dual antiplatelet therapies (aspirin and clopidogrel) after stent implantation; all other treatment measures remained the same following stent implantation.
Laboratory findings
Elevated ESR levels (n > 21 mm/h) and CRP levels (n > 0.9 mg/dl) were found in 33.3% (12/36) and 36.1% (13/36) of the patients with PH attributable to PA, respectively. Nine of the patients with PH with PA had hypoxemia (PaO2 < 60 mmHg) compared with 1 patient with PH due to LHD. Additionally, patients with PH due to PA were more hypoxemic than patients with PH from LHD (PaO2 71.2 ± 13.3 vs 79.2 ± 12.6 mmHg, p = 0.001). However, patients with PH associated with LHD showed a higher tendency for hyponatremia (serum sodium level < 135 mmol/l) compared to patients with PH because of PA (50.0% vs 11.1%, p = 0.009). The mean serum sodium level was 138.6 mmol/l in patients with PH because of PA compared to 135.8 mmol/l for patients with PH because of LHD (Table 1B). Serum levels of big ET-1 were significantly higher in patients with PH associated with PA than in those patients with PA without PH (1.0 ± 0.7 vs 0.3 ± 0.1 pg/ml, p < 0.001; Table 2). In addition, big ET-1 levels independently correlated with PASP (r = 0.33, p = 0.04; Appendix 1) and right ventricular dimension (r = 0.40, p = 0.02; Appendix 2) in patients with PH with PA.
Laboratory variables and drug treatments of patients with PH in TA and patients with IPAH. Values are mean ± SD or n (%) unless otherwise specified.
Characteristics of patients with pulmonary artery involvement. Values are mean ± SD or n (%) unless otherwise specified.
All 48 patients with TA hospitalized with PH had abnormal levels of NT-proBNP (> 400 pg/ml). NT-proBNP levels were higher in patients with PH because of LHD in comparison to patients with PH with PA, and the mean NT-proBNP level for patients with TA with PH because of LHD was 4693.8 pg/ml compared to 2062.1 pg/ml for PH due to PA, and 838.6 pg/ml for patients with TA with PA who did not have PH. Hypoxemia (n = 10), hyponatremia (n = 10), pericardial effusion (n = 9), or a combination were found in 9 patients with PH due to LHD and 10 patients with PH associated with PA. Moreover, the mean levels of NT-proBNP in patients with TA with PH who had hypoxemia, hyponatremia, or pericardial effusion were higher than in those patients who did not (4266.2 vs 1656.3 pg/ml, p < 0.001). In addition, serum NT-proBNP levels were independently associated with NYHA functional classification in TA-related patients with PH (r = 0.27, p = 0.01). However, no significant association was found between NT-proBNP levels and PASP in patients with PA with PH (r = 0.26, p = 0.10).
Imaging findings
Reduced or absent uptake on pulmonary perfusion scans was demonstrated in 36 patients with PH attributable to PA. Moreover, lung perfusion scans revealed segmental, large and right-sided, or bilateral defects. However, in all 30 patients with IPAH, the lung perfusion scans were nearly normal. All 36 patients with PH who had PA underwent enhanced CT scanning, and 16 of those patients underwent pneumoangiography. Changes in the central and peripheral right-sided pulmonary arteries were more common than left-sided changes, and lobar vessels were more commonly involved than segmental or subsegmental vessels. Moreover, the upper and lower branches were more frequently involved than the middle branches.
The main imaging findings for patients with PH due to PA were summarized as follows: pulmonary arterial occlusion or near occlusion (88.9%, n = 32), pulmonary arterial stenosis (58.3%, n = 21), and poststenotic dilation (27.8%, n = 10). Right main pulmonary artery lesions were found in 24 patients, of whom 16 patients had pulmonary artery stenosis, 6 patients had occlusion or near occlusion, and 2 patients had poststenotic dilation. There was involvement of the left main pulmonary artery in 10 patients, of whom 4 had pulmonary arterial stenosis, 2 had occlusion or near occlusion, and 4 had poststenotic dilation. Lesions of stenosis (12 vs 6), occlusion or near occlusion (66 vs 10), and poststenotic dilation (12 vs 26) were found in the right and left upper lobe segmental arteries, respectively. Among the lesions of the right middle lobe segmental arteries, there were 2 lesions of stenosis, 50 of occlusion or near occlusion, and none of poststenotic dilation. Eight stenotic lesions, 16 of occlusion or near occlusion, and 4 of poststenotic dilation were found in the left lingular segmental artery. Lesions of stenosis (28 vs 40), occlusion or near occlusion (56 vs 64), and poststenotic dilation (30 vs 8) were found in the right and left lower lobe segmental arteries, respectively (Table 3). Additionally, a weak correlation was found between the CT obstruction index and the degree of PASP in patients with PA with PH (r = 0.24, p = 0.02; Appendix 3).
Computed tomography or pulmonary angiographic findings. Data refer to numbers of patients.
In 36 patients with PH who had PA, 7 patients (19.4%) had isolated pulmonary vasculitis, and the rest had aortic and large artery involvement. The involved segments of the aorta were as follows: the abdominal aorta (25.0%), the descending aorta (22.2%), the arch (19.4%), and the ascending aorta (16.7%). The left common carotid artery (36.1%) was the most frequently involved branch, followed by the left subclavian artery (30.5%), the right subclavian artery (16.7%), and the right common carotid artery (13.8%). Two patients had coronary artery involvement. In 12 patients with PH who had LHD, the involved segments of the aorta branches were as follows: the abdominal aorta (66.7%), the descending aorta (41.7%), and the ascending aorta (33.3%). The left common carotid artery (83.3%) was the most frequently involved branch, followed by the left subclavian artery (75.0%), the right common carotid artery (58.3%), and the right subclavian artery (33.3%).
Echocardiographic findings
Patients with PH associated with PA and patients with IPAH showed relatively normal left ventricular ejection fractions (LVEF; 65.9 ± 5.6 vs 67.2 ± 8.3%, respectively), while patients with PH because of LHD demonstrated reduced left ventricular systolic function (LVEF 41.3 ± 16.6%). Severe PH was observed in most of the patients with PH due to PA (88.9%) and in the patients with IPAH (90.0%), while mild to moderate PH was more frequently found in patients with PH attributable to LHD (91.6%). In addition, of the 36 patients with PH due to PA, tricuspid valve regurgitation (TR), mitral valve regurgitation (MR), and aortic valve regurgitation (AR) were found in 36 (100%), 8 (22.2%), and 9 (25.0%) patients, respectively. TR, MR, and AR were found in 12, 10 (83.3%), and 9 (75.0%) patients, respectively, in the 12 patients with PH due to LHD (Table 4).
Echocardiographic variables in patients with TA and patients with IPAH. Values are mean ± SD or n (%) unless otherwise specified.
Findings of RHC and cardiopulmonary exercise testing
RHC and vasoreactivity testing was performed according to standard procedures in all 30 patients with IPAH and 12 patients with PH due to PA. Patients with PH due to PA who were undergoing RHC developed higher incidence of right-to-left shunts (0.8 ± 0.3 vs 1.0 ± 0.3, p = 0.02) and lower average cardiac index (2.0 ± 0.5 vs 3.0 ± 1.2 l/min/m2, p = 0.05) compared to patients with IPAH. And patients with PH who had PA had lower average peak VO2 during exercise (11.5 ± 1.7 vs 13.4 ± 2.8 ml/kg/min, p = 0.04) than patients with IPAH. After administration of iloprost inhalation, all 12 patients with PH who had PA and who underwent RHC (100%) and 10 of the patients with IPAH (33.3%) had favorable responses to acute vasodilator testing (Table 5).
Hemodynamic variables of PH associated with patients with PA and patients with IPAH. Values are mean ± SD or n (%) unless otherwise specified.
Patient outcomes
After discharge from the hospital, 36 patients with PH caused by PA were followed for 36.0 ± 13.2 months (12.0–65.0 mos) and 3 patients were lost during followup. A total of 3 patients died of heart failure. Additionally, 6 patients with PA underwent pulmonary artery revascularization and were followed for a mean duration of 6.2 ± 1.9 months; during followup, all of the patients’ clinical symptoms improved significantly and all of the patients had good prognoses and significantly decreased levels of NT-proBNP (1376.8 ± 205.9 vs 640.0 ± 90.9 pg/ml, p < 0.001). Twelve patients with PH because of LHD were followed for 38.4 ± 15.6 months (12.0–60.0 mos); 1 patient died of heart failure during the followup period.
DISCUSSION
TA is associated with several forms of PH. It can cause PH through pulmonary vasculopathy, LHD, and chronic thromboembolic pulmonary hypertension (CTEPH). On autopsy of patients with TA, the rate of PA can reach 20–56%8,14, and the rate of PH in patients with TA is about 12–13% in various reports7,8. Our data showed that respiratory symptoms such as shortness of breath and hemoptysis were often the initial symptoms in patients with PH because of PA. Systemic signs related to TA are not specific and may be masked by symptoms originating from the involvement of other large vessels that may result in delayed or incorrect diagnoses. There should be a high index of suspicion, especially when there is reduced or absent uptake on pulmonary perfusion scans in young women with general signs of systemic vasculature damage, and recognition of specific pulmonary lesions on imaging studies (CT, magnetic resonance imaging, pulmonary angiography) will lead to early and accurate diagnosis and proper treatment with steroids. Vessel wall thickening, lumen narrowing, and/or dilation observed in CT or angiography studies were characteristics of TA15. In addition, our data showed that occlusion of the main pulmonary artery was frequently found and smaller distal pulmonary arteries were often preserved. The right-sided pulmonary arteries, both central and peripheral, were more often involved than the bilateral or left-sided arteries, and the upper and lower branches were more frequently involved than the middle branches. Additionally, vascular occlusion was found more frequently than vascular stenosis and dilation.
PH associated with PA had been thought to occur exclusively as a result of mechanical obliteration of the vascular bed and was a major determinant of the severity of PH3. A few cases and our data indicated that a significant decrease in PVR was induced by the administration of vasodilators16, suggesting that increased pulmonary vascular tone may also be an important contributing factor in increasing PVR. The pathogenesis of this increased pulmonary vascular tone was unknown; hypoxic vasoconstriction, neurohormonal activation, and endothelial cell dysfunction may play a role17,18,19. Our data suggested that 9 patients with PH due to PA presented with hypoxemia. The main causes of hypoxemia were the presence of lung units with low ventilation-perfusion ratios, right-to-left shunts, or diffuse dysfunction; when severe airway obstruction was present, alveolar hypoventilation contributed to decreased PaO2 values20. A few cases had reported that high inspired oxygen tension failed to significantly reduce PVR in the patients with TA16; therefore, other factors could be involved in the pathogenesis and development of patients with PH due to PA.
Studies have shown that the ET system is activated not only in IPAH, but also in other forms of PH, and big ET-1 was thought to be a more reliable indicator for the activation of the ET-1 system because of a longer plasma half-life and much less tissue extraction21,22. Though there is a paucity of research on the mechanisms of TA-related PH specifically, there are several lines of evidence that point to a particular endothelial focus23,24. Our data showed that levels of big ET-1 were higher in patients with PH due to PA than in patients with PA without PH, and moreover, serum levels of big ET-1 independently correlated with PASP and right ventricular dimensions, suggesting a potential role in risk stratification for patients with PA who have PH. At present, the mechanism underlying this finding is not fully understood, but it likely includes mechanical and immunological factors. A previous study about the altered regulation of the ET-1 cascade in lambs with increased pulmonary blood flow and PH found that the relatively high flow of blood through the non-occluded pulmonary vascular bed and the existing PH may increase the expression of ET-A receptor mRNA and protein, decreasing the expression of ET-B receptor mRNA and protein; the net result of these gene alterations is an increased production of ET-1, which could in turn contribute to the development of PH and its associated enhanced pulmonary vascular reactivity18.
Persistent obstruction of pulmonary arteries may result in distal pulmonary vasculopathy, likely similar to that encountered in IPAH and CTEPH25,26. The weak correlation between the extent of the central obstruction of the pulmonary vasculature and the degree of PASP in our data showed some evidence in support of this hypothesis. In our study, PH caused by PA and IPAH showed higher incidences of severe PASP, while PH associated with LHD showed a higher frequency of mild to moderate PASP. One explanation for this phenomenon may be that the combination of persistent vascular obstruction, persistent increases in PVR, and right ventricular pressure overload may typically result in severe PASP. In addition, as previously mentioned, higher levels of big ET-1 and chronic hypoxia may be involved in the pulmonary vascular remodeling in PA-related PH. Recent studies showed that peak VO2 was 1 of the most powerful prognosticators in chronic heart failure and patients with IPAH27,28,29. Compared to patients with IPAH, our data suggested that peak VO2 and cardiac index were significantly reduced in patients with PH due to PA, suggesting a worse right ventricular function and an underlying worse prognosis.
As previously mentioned, TA-associated PH could also occur secondary to LHD. In the patients with TA, the left ventricular (LV) filling pressure could be elevated by HTN, LV hypertrophy, LV systolic dysfunction, LV diastolic dysfunction, and AR30. Our data showed that the levels of NT-proBNP were elevated in patients with IPAH and patients with PH associated with PA, and were on average higher in patients with PH because of LHD. In addition, patients showed a higher frequency of hyponatremia, a marker of neurohormonal activation, in PH associated with LHD. Patients in our study who had hypoxemia, hyponatremia, or pericardial effusion had higher levels of NT-proBNP, a finding invariably related to a poor prognosis31,32,33,34. All of these findings aggravated the progression of heart failure.
The prognosis of patients with PH is often poor because the disease may become even more aggravated by the underlying PA. The management of PH due to LHD should be aimed at the optimal treatment of the underlying disease35. The treatment of patients with PH attributable to LHD in our data included steroids, aspirin, diuretics, β blockers, and ACEI or ARB; no patients were treated with PH-specific therapies and warfarin. The primary treatment of PH due to PA was steroids therapy. Other therapeutic approaches included diuretics, digoxin, aspirin, and/or warfarin, which is similar to the treatment for IPAH36. Moreover, longterm aspirin therapy contributes to prevent thrombus formation in vessels with endothelial damage in TA37. Accordingly, other than oral anticoagulation in IPAH, aspirin was commonly used in patients with PA who had PH, and warfarin therapy would be specifically recommended in these patients with pulmonary artery thrombosis. Positive acute responders to vasoreactivity testing are most likely to show a sustained response to longterm treatment with high doses of CCB, and they are the only patients who can safely be treated with this type of therapy. However, at present, the usefulness of acute vasoreactivity tests and longterm treatment with CCB in patients with other PAH types is less clear than in IPAH36.
Additionally, our data showed that all patients with PA-related PH who underwent RHC developed favorable responses to acute vasodilator testing. Therefore, CCB may be an alternative treatment for patients with PH who have PA and positive responses to vasoreactivity testing. Seven patients with PH with PA and severely elevated mPAP on RHC were treated with PH-specific therapies (bosentan or sildenafil), and all of these patients had significant improvements in PH-related symptoms. Additionally, 6 patients underwent stent implantation in the pulmonary arteries, all with good results and obviously decreased levels of NT-proBNP after several months of followup. Thus, oral therapy with PH-specific therapies and revascularization could be considered in patients with PA who have PH and severe pulmonary artery stenosis.
One limitation of our study is that it was a retrospective study, and therefore some of the clinical data are not complete. Three patients were lost to followup, which may lead to an underestimation of mortality. In addition, the followup period was very short.
TA is associated with several forms of PH. It can cause PH through PA, LHD, and CTEPH. In patients with unexplained PH, screening should be performed for pulmonary vasculitis including systemic illness such as TA. Serum levels of big ET-1 were independent predictors of PASP in patients with PH due to PA, suggesting a potential role in risk stratification and a possible marker for followup, while higher serum levels of NT-proBNP implied a worse prognosis. In addition, PH-specific therapies (such as endothelin receptor blockers and sildenafil) or pulmonary artery revascularization could be considered in the early stages of patients with PA-related PH with severe pulmonary artery stenosis. Further studies should address the potential predictive prognostic value of serum levels of big ET-1, as well as the therapeutic benefit of ET receptor antagonists in patients with PA-related PH.
APPENDIX 1.

Correlations between the serum level of big ET-1 and PASP in patients with TA who have PH attributable to PA. ET-1: endothelin 1; PASP: pulmonary arterial systolic pressure; TA: Takayasu arteritis; PH: pulmonary hypertension; PA: pulmonary arteritis.
APPENDIX 2.
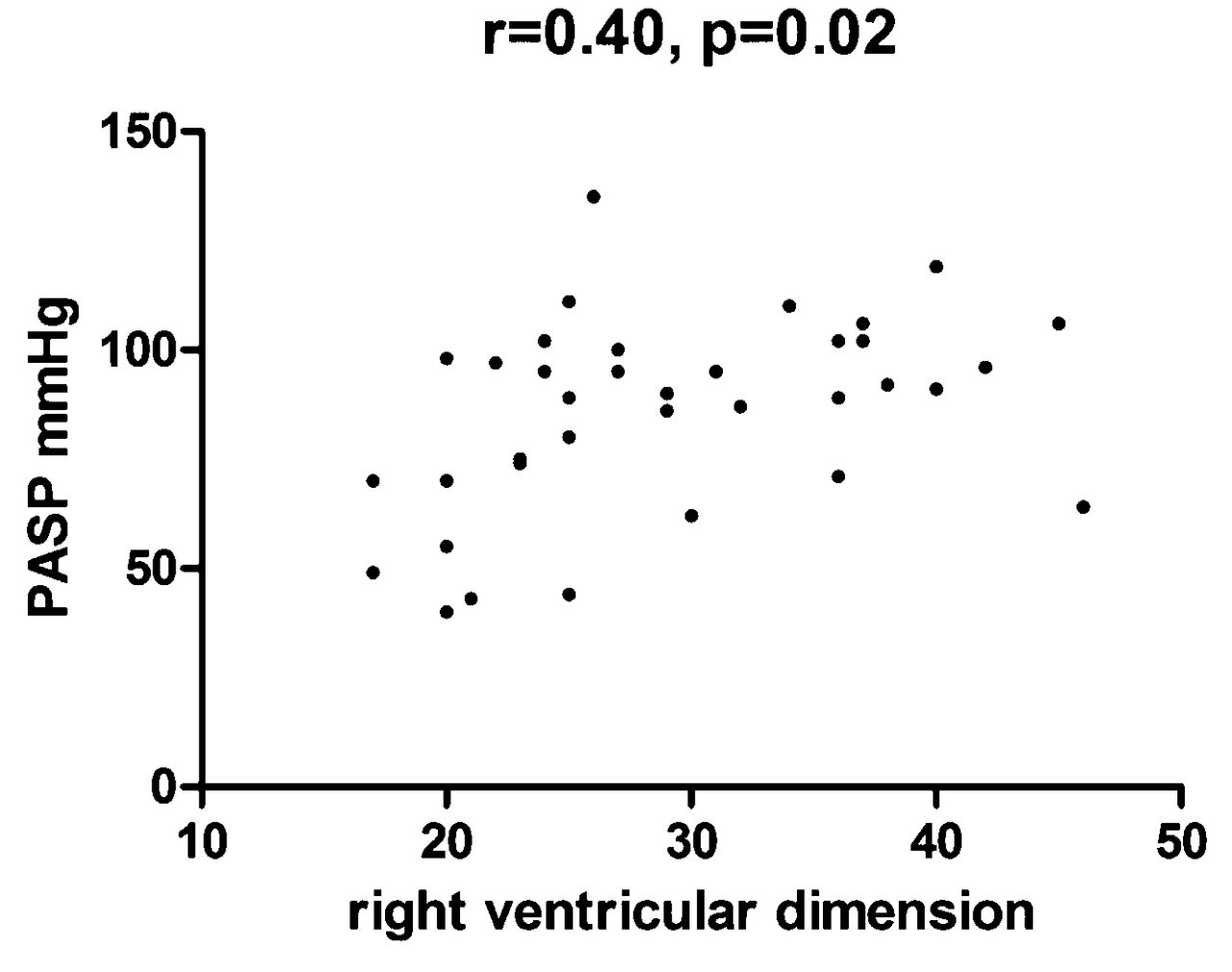
Correlations between the serum level of right ventricular dimension and PASP in patients with TA who have PH due to PA. PASP: pulmonary arterial systolic pressure; TA: Takayasu arteritis; PH: pulmonary hypertension; PA: pulmonary arteritis.
APPENDIX 3.

Correlations between the CT obstruction index and PASP in patients with TA who have PH due to PA. CT: computed tomography; PASP: pulmonary arterial systolic pressure; TA: Takayasu arteritis; PH: pulmonary hypertension; PA: pulmonary arteritis.
Footnotes
-
Supported by the National Natural Science Foundation of China (grant number: 81170285) and the Research Fund for the Doctoral Program of Higher Education of China (grant number: 20101106110012)
- Accepted for publication November 18, 2014.








{kind=link}
{kind=link}
{kind=link}