
Abstract
Objective. To characterize cumulative joint damage (CJD) patterns in rheumatoid arthritis (RA) and determine their associations with demographic/clinical features and HLA-DRB1 gene polymorphism.
Methods. Hand and foot radiographs were obtained from 404 patients with RA. CJD patterns were determined by 3 derivations from Sharp/van der Heijde scores, obtained by the mathematical division of scores for hands/feet (Sharp-h/f score), fingers/wrists (Sharp-f/w score), and erosion/space narrowing (Sharp-e/sn score), respectively. DNA and serum were obtained for determination of HLA-DRB1 polymorphism, rheumatoid factor (RF), and anticitrullinated protein antibodies (ACPA).
Results. Patients with wrist-dominant CJD pattern were more likely to have severe RA than those with finger-dominant pattern (68.4% vs 46.0%; p = 0.036) as were those with foot-dominant vs hand-dominant CJD pattern (76.5% vs 56.4%; p = 0.044). HLA-DRB1 shared epitope (SE) alleles were associated with erosion-dominant CJD pattern (p = 0.021). Patients with erosion-dominant CJD pattern had higher levels of RF and ACPA than those with space-narrowing–dominant CJD pattern (median RF 71.35 U/ml vs 22.05 U/ml, respectively; p = 0.003; median ACPA 187.9 U/ml vs 143.2 U/ml, respectively; p < 0.001). The majority of triple-positive patients (SE+, RF+, ACPA+) had erosion-dominant CJD pattern (62.3%) while the majority of triple-negative patients (SE–, FR–, ACPA–) had space narrowing–dominant CJD pattern (75%; p = 0.017). ACPA was associated with HLA-DRB1 SE alleles (p < 0.05). Patients with foot-dominant CJD pattern were taller than those with hand-dominant CJD pattern (p = 0.002); those with erosion-dominant CJD pattern had higher weight and body mass index than those with space narrowing–dominant CJD pattern (p = 0.014, p = 0.001).
Conclusion. CJD patterns were associated with disease severity, HLA-DRB1 SE status, presence and titer of ACPA and RF, and morphometric features.
- RHEUMATOID ARTHRITIS
- DIAGNOSTIC IMAGING
- JOINT EROSIONS
- RHEUMATOID FACTOR
- ANTICITRULLINATED PROTEIN ANTIBODIES
Rheumatoid arthritis (RA) is a heterogeneous disease in terms of joint damage. Some patients present mild joint involvement and others develop progressive joint destruction and severe functional impairment1. Despite recent progress, the available therapeutic options are not entirely satisfactory for all patients. Pathophysiological definition and therapeutic management of RA might be improved if it were possible to identify more homogeneous disease subphenotypes. One possible way to identify RA subphenotypes is the definition of distinct patterns of cumulative joint damage (CJD). Radiographic analysis allows the identification of distinct patterns of joint involvement regarding the topography of joint damage (hands vs feet and fingers vs wrists) and the type of lesion (erosion vs space narrowing; Figure 1). Total joint damage in RA can be estimated by the Sharp/van der Heijde (SvdH) method2, which yields a composite score for overall erosion and joint space narrowing at hands and feet. Although very useful for estimating disease severity and global joint damage in hands and feet, this method does not allow discrimination of the different patterns of CJD.

Patterns of cumulative joint damage (CJD). Panels A and B: sets of radiographs from distinct patients with hand-dominant (A) and foot-dominant (B) CJD pattern. Panel C: radiographs from distinct patients with wrist-dominant (left) and finger-dominant (right) CJD patterns. Panel D: erosion-dominant (left) and space narrowing–dominant (right) CJD pattern. Filled single arrows: erosion sites; double arrows: space-narrowing sites; unfilled single arrows: preserved sites.
Several studies have addressed the heterogeneity in joint involvement patterns in RA. Hulsmans, et al prospectively studied a large cohort of patients with recent-onset RA and observed that erosions occurred at a higher rate than joint space narrowing, and that erosions in the feet were more frequent and earlier than in the hands, especially at the fifth metacarpophalangeal joint3. Smolen and colleagues compared the progression of hand and foot joint erosion versus space narrowing in patients with early RA under treatment with infliximab/placebo and methotrexate and found that the appearance of erosions was more frequent than joint space narrowing, especially in the placebo group4. Landewé, et al confirmed these observations based on 4 large databases of patients with RA and showed that joints of the wrist tended to worsen over time in terms of joint space narrowing5. Finally, Dirven, et al found an association between large joint damage, as assessed by Larsen score, and small joint damage, as assessed by the SvdH method, in patients with RA6.
In our present study we used derivative SvdH scores to determine the dominant topography of joint damage (hands vs feet and fingers vs wrists) and the dominant type of lesion (erosion vs space narrowing), thereby identifying 3 distinct CJD patterns. We used these derivative scores to describe the distribution of CJD patterns in a multicenter cohort of patients with RA and studied possible associations between CJD patterns and demographic variables, disease phenotypic traits, autoantibody profile, and HLA-DRB1 gene polymorphism.
MATERIALS AND METHODS
Patients
Patients with RA (n = 404) met American College of Rheumatology classification criteria7 and were sequentially enrolled at 4 university centers in Brazil. Patients were ethnically self-classified as follows: European-derived or African-derived when both parents and the 4 grandparents were equally self-classified as European- or African-derived, respectively; Mulattos, when there were European-derived and African-derived members in the second-generation relatives; Asian-derived when both parents and the 4 grandparents were self-classified as Asian-derived. All patients signed the informed consent form approved by the ethics committee at each participating center, donated blood samples for autoantibody and gene polymorphism determination, had hand and foot radiographs taken, and filled out a standard clinical questionnaire, including data for the Health Assessment Questionnaire–Disability Index (HAQ-DI)8.
Laboratory procedures
Anticitrullinated protein antibody (ACPA) levels were determined using the QUANTA-Lite CCP-ELISA (INOVA Diagnostics), according to the manufacturer’s instructions. Rheumatoid factor (RF) was measured by nephelometry (Dade Behring Marburg-GmbH). Genomic DNA was extracted from peripheral blood cells using a standard salting-out extraction method or the GFX (Amersham). HLA-DRB1 typing was performed by polymerase chain reaction followed by hybridization with sequence-specific oligonucleotides using HLA genotyping kit (One Lambda), according to the manufacturer’s instructions.
Radiographic assessment
Images were obtained under standard conditions established at the Muscle-Skeletal Division of the Imaging Department at Federal University of São Paulo Medical Hospital. Briefly, hands and wrists were imaged as postero-anterior incidence and the anterior part of feet was imaged at antero-posterior incidence. Radiographic exposures followed these standards: 42 kV, 5–10 milliamperes/s, distance focus-film of 100 cm. Images were digitalized with a Multicassette CR 975 Carestream system. Hand and foot radiographs were blindly scored by an experienced radiologist, according to the SvdH method2. Intraobserver reproducibility was determined on 50 randomly chosen pairs of hand and foot radiographs scored twice by the same investigator, yielding an intraclass correlation coefficient between 2 readings of 0.94. Because there was considerable variation in disease duration, disease severity could not be appropriately estimated from the raw SvdH scores. Instead, a linear regression analysis was used to determine the trend of SvdH score in relation to disease duration. An arbitrary interval deviation from the central trend line was established as representative of average joint destruction along disease duration. This interval corresponds to 95% probability for the distribution of the central trend line in this cohort of patients. Individuals scoring above and below these boundaries were considered representative of severe and mild disease, respectively (Figure 2). Those within these boundaries were not considered in the analysis of disease severity.

Distribution of patients with rheumatoid arthritis (RA) according to total Sharp-van der Heijde (SvdH) score and disease duration. The thin line represents the central trend of SvdH score progress over the years based on the total cohort of patients, and the thick continuous and dashed lines represent the upper and lower interval boundaries, respectively. This interval corresponds to 95% probability for the distribution of the central trend line in this cohort of patients. Dots scattered above the thick continuous line represent patients who were considered to have severe RA and those scattered below the thick dashed line represent patients who were considered to have mild RA.
To determine CJD patterns, derivative SvdH scores were calculated through the mathematical division of hand/foot SvdH scores (Sharp-h/f score), finger/wrist scores (Sharp-f/w score), and erosion/space-narrowing scores (Sharp-e/sn score) for each patient. This analysis included only patients with disease duration less than 15 years, to minimize potential secondary distortions due to longstanding disease. Aiming to achieve enough magnitude for calculation of derivative scores, only those with total SvdH score over 44 (10% of the maximum total SvdH scale) were included in the analysis of Sharp-h/f and Sharp-e/sn scores; those with SvdH score of hands over 28 (10% of the maximum SvdH scale for hands) were included in the analysis of Sharp-f/w scores. The distribution of derivative score values in the cohort was used to determine the prevalent behavior, termed “balanced,” and zones of deviation from the prevalent behavior (< 30% and > 70% percentile, respectively), termed “imbalanced.” Thus, for each of the 3 derivative scores considered, 40% of the patients had balanced CJD pattern and 30% had imbalanced CJD pattern in each pole.
Statistical analysis
Categorical variables were analyzed using the chi-squared test or Fisher’s exact test when appropriate. Quantitative variables were tested for the distribution pattern by the Kolmogorov-Smirnov test and the appropriate statistical test was used according to this preliminary analysis: ANOVA and Student t test for variables with normal distribution; Kruskal-Wallis test and Mann-Whitney U test for variables with non-normal distribution. Correlations between quantitative variables were analyzed by the Spearman method. Univariate logistic regression analyses were used when appropriate. Significant p value was set at p < 0.05.
RESULTS
Clinical and laboratory characteristics of patients with RA are summarized in Table 1. Extraarticular manifestations were found in one-third of the patients: 23 with ocular manifestations (22 with xerophthalmia and 1 with uveitis), 24 with xerostomia, 77 with rheumatoid nodules, 8 with pulmonary manifestations, and 1 with vasculitis. As expected, SvdH score correlated positively with disease duration (r = 0.49, p < 0.001). Figure 2 depicts the linear regression model used to determine the trend of SvdH score in relation to disease duration. According to this model, 297 patients were classified as having either mild (n = 150) or severe (n = 147) RA, and 107 patients were classified within the general trend of disease severity.
Demographic, clinical, and laboratory characteristics of rheumatoid arthritis patients. Unless otherwise stated, the number of patients analyzed was 404.
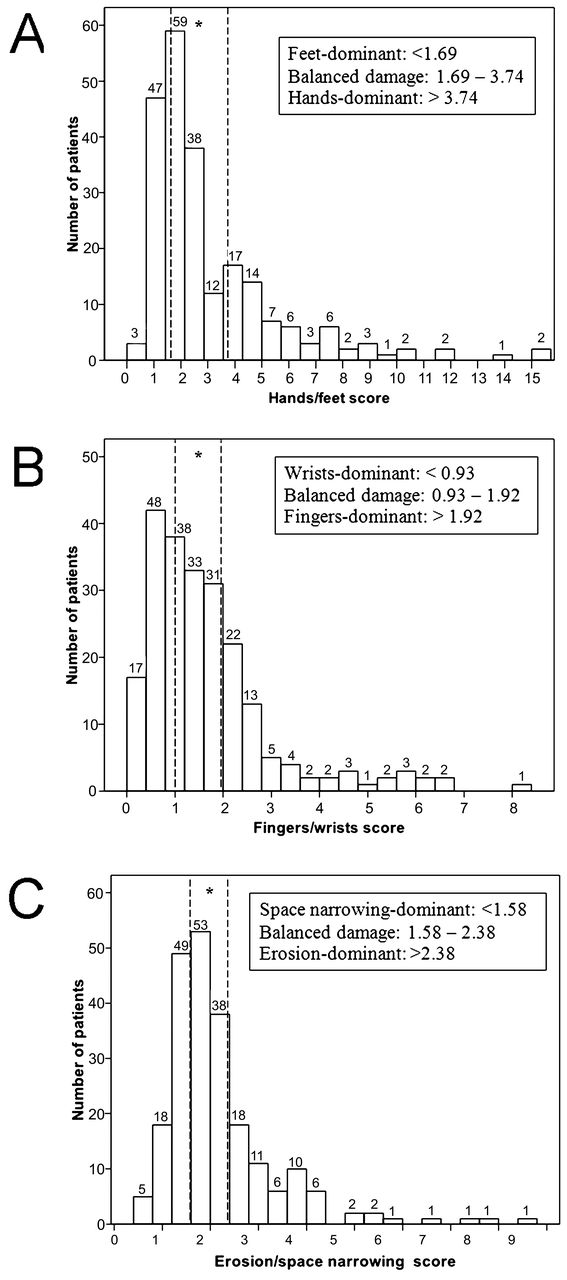
The Sharp-h/f and Sharp-e/sn scores were calculated for 230 patients and the Sharp-f/w score for 243 patients. The distribution of patients according to derivative scores did not follow a Gaussian configuration (Figure 3). The central trend and variation in CJD patterns, represented by the median and range of derivative scores, was 2.29 (0.33–15.0) for the Sharp-h/f score, 1.38 (0.06–8.0) for the Sharp-f/w score, and 1.85 (0.59–8.44) for the Sharp-e/sn score. Patients below the 30th and those above the 70th percentile for each derivative score were classified as having an imbalanced CJD pattern in the collective cohort distribution. Those lying within the 30th–70th percentile interval were classified as having a balanced CJD pattern. The general trend was for predominant erosion over space narrowing, and hand over foot involvement (Figure 3).
{kind=link}
{kind=link}
{kind=link}
Distribution of rheumatoid arthritis patients according to (A) hand/foot score, (B) finger/wrist score, and (C) erosion/space-narrowing score. Imbalanced patterns of cumulative joint damage were defined as those areas below the 30th and above the 70th percentile distribution of derivative Sharp-van der Heijde scores, respectively. *Intervals between dashed vertical lines correspond to balanced patterns of cumulative joint damage (≥ 30th and ≤ 70th percentile).
Association between joint damage and phenotypic features
Patients with severe and mild RA did not differ with respect to sex (p = 0.458) and ethnicity (p = 0.364). There was higher frequency of prednisone use in the severe RA group (p = 0.001). Prednisone was used by 68% of patients with severe disease and by 50.5% of those with mild disease. Patients with severe RA had a higher frequency of RF (74.8%) and ACPA (90.1%) compared to those with mild RA (56.6%, p = 0.001; and 72.1%, p < 0.001, respectively).
CJD patterns were associated with disease severity but not with disease duration. The frequency of severe RA, as assessed by total SvdH score, was higher in patients with foot-dominant versus those with hand-dominant pattern (76.5% and 56.4%, respectively; p = 0.044). Accordingly, SvdH score was higher in patients with foot-dominant pattern (median 117.5, range 45–379) versus those with hand-dominant pattern (median 81.0, range 46–184; p = 0.002). In addition, patients with wrist-dominant pattern had higher frequency of severe RA (68.4%) versus those with finger-dominant pattern (46.0%; p = 0.036). Hence, there was a strong trend for higher SvdH score in patients with wrist-dominant pattern (median 95.0, range 38.0–237.0) as compared to those with finger-dominant pattern (median 78.0, range 38.0–282.0; p = 0.089). CJD patterns had an effect on quality of life, as assessed by the HAQ-DI. HAQ-DI was higher in patients with hand-dominant pattern (mean and SD: 0.79 ± 0.65) than in those with foot-dominant pattern (0.51 ± 0.52; p = 0.012), and higher in patients with wrist-dominant pattern (0.75 ± 0.61) versus those with finger-dominant pattern (0.55 ± 0.60; p = 0.044). No association was observed between HAQ-DI and erosion/space-narrowing CJD patterns.
Imbalanced erosion/space-narrowing pattern was associated with the presence of RF and ACPA. Erosion-dominant pattern was more frequent in RF-positive than in RF-negative patients (56.7% vs 36.2%; p = 0.023) and RF serum levels were higher in patients with erosion-dominant pattern than in those with space narrowing-dominant pattern (median 71.35 U/ml, range 0–2280; vs 22.05 U/ml, range 0–750, respectively; p = 0.003). Erosion-dominant pattern was also more frequent in ACPA-positive than in ACPA-negative patients (54.0% vs 30.4%; p = 0.04) and ACPA serum levels were higher in patients with erosion-dominant pattern than in those with space narrowing–dominant pattern (median 187.9 U/ml, range 5–256 vs 143.2 U/ml, range 4–254, respectively; p < 0.001).
CJD patterns were also associated with some morphometric variables. Height was associated with imbalanced hand/foot pattern, because patients with foot-dominant pattern were taller than those with hand-dominant pattern (1.60 ± 0.07 m vs 1.56 ± 0.07 m; p = 0.002). Weight and body mass index (BMI) were associated with imbalanced erosion/space-narrowing pattern, as patients with erosion-dominant pattern had greater weight (71.5 ± 15.0 kg vs 64.8 ± 11.3 kg, p = 0.014) and BMI (28.4 ± 5.0 vs 25.3 ± 3.5, p = 0.001) than patients with space narrowing–dominant pattern.
Association between joint damage and DRB1 shared epitope alleles
SE-containing HLA-DRB1 alleles were present in 251 (63.1%) of 398 patients, 48 (12.1%) of whom had 2 SE alleles. The frequency of individuals with mild and severe disease was similar in patients with single (45.9% vs 51.0%) and double copy SE alleles (13.0% vs 9.7%; Table 2). There was also no difference regarding the presence of specific SE alleles. There were some interesting associations between DRB1 gene polymorphism and CJD patterns (Table 3). Imbalanced erosion/space-narrowing CJD pattern was associated with the presence of SE alleles, because patients with SE alleles had higher frequency of erosion-dominant pattern (57.1% vs 36.7%; p = 0.021) and higher erosion/space-narrowing scores than patients without SE alleles (median 2.0; 0.6–8.4 and 1.74; 0.6–6.8, respectively; p = 0.023). No association was found with the number of SE alleles (Table 3) and with individual SE alleles (data not shown).
Frequency of HLA-DRB1 shared epitope (SE) alleles in the total number of patients (291) with mild and severe rheumatoid arthritis (RA).
Association between patterns of cumulative joint damage (CJD) and the presence of DRB1 shared epitope (SE) alleles in patients with rheumatoid arthritis.
Because of the observed correlation of ACPA and RF serum levels (r = 0.452, p < 0.001) and the observed association of ACPA and SE alleles (p < 0.001), the previously observed associations of these 3 factors with erosion/space-narrowing score needed to be validated by segregation of these variables. After segregation, the statistical significance of the association of individual variables with the erosion/space-narrowing score was lost, probably owing to the small number of individuals in each stratum. However, it should be noted that the 61 triple-positive patients (SE+, RF+, ACPA+) had predominance of bone erosion-dominant pattern (62.3%) while the 12 triple-negative patients (SE–, RF–, ACPA–) had predominance of space narrowing–dominant pattern (75.0%; p = 0.017). Accordingly, the Sharp-e/sn score was higher in the triple-positive patients (median Sharp-e/sn score 2.06, range 0.67 to 7.71) as compared to the triple-negative patients (median Sharp-e/sn score 1.68, range 0.91 to 6.80; p = 0.035).
Logistic regression analysis for determination of risk factors for joint damage
Baseline variables with association at p <0.05 level were analyzed in separate univariate logistic regression models in which the variables related to disease severity were the independent variables. CJD scores could not be analyzed as independent factors at the same model because there was collinearity among them (data not shown). Risk factors for more severe RA were a positive RF test (OR 2.52; 95% CI 1.53–4.15; p < 0.001); foot-dominant CJD pattern (OR 2.51; 95% CI 1.02–6.21; p = 0.046); and wrist-dominant CJD pattern (OR 2.54; 95% CI 1.05–6.14; p = 0.038). In addition, high-titer ACPA (OR 1.008; 95% CI 1.004–1.013; p < 0.001) and high BMI (OR 1.196; 95% CI 1.071–1.337; p = 0.002) were predictive factors of erosion-dominant pattern.
DISCUSSION
Our present study explores the heterogeneity in qualitative aspects of joint damage in RA by defining and investigating CJD patterns (preferential topography and preferential type of joint damage). The traditional SvdH scoring method provides a composite measurement of these dimensions, but does not emphasize each one separately. Here we present a novel scoring approach that allows us to segregate patients according to CJD patterns. Three secondary SvdH scores were mathematically derived to assess the balance between bone erosion versus space narrowing, finger versus wrist involvement, and hand versus foot involvement. These derivative scores were calculated for each individual in a large multicenter series of patients with RA. For each of the 3 CJD comparisons, patients were divided into 3 groups: those exhibiting a balanced CJD pattern (between 30% and 70% percentiles) and those exhibiting an imbalanced pattern in either pole (below 30% percentile or above 70% percentile). Because the maximum SvdH scores are greater for hands (280) than feet (168), for erosion (280) than for space narrowing (168), and for fingers (172) than for wrists (108), there is an inherent bias for overrepresentation of hands over feet (hmax/fmax = 280/168 = Sharp-h/f score 1.67), erosion over space narrowing (emax/snmax = 280/168 = Sharp e/sn score 1.67), and fingers over wrists (fmax/wmax = 172/108 = Sharp f/w score 1.59). In the present cohort we observed that patients exhibiting balanced patterns (percentile 30–70%) showed more pronounced bias toward hands than feet (Sharp-h/f score 1.69–3.74) and erosion than space narrowing (Sharp-e/sn score 1.58–2.38) than predicted from the inherent bias. This was not the case for the finger versus wrist evaluation (Sharp-f/w score 0.93–1.92).
Once the CJD patterns were defined, we investigated potential correlations of each CJD pattern with demographic, clinical, and serologic measurements of the disease, as well as with the presence of SE-containing HLA-DRB1 alleles. The frequency of patients carrying SE alleles was consistent with several other studies in Brazilian patients with RA and probably reflects the ethnic composition of the Brazilian population9,10,11. Our analyses showed that erosion-dominant CJD pattern was associated with the presence of RF, ACPA, SE alleles, and high BMI. Additionally, severe disease was associated with foot-dominant and wrists-dominant CJD patterns. Univariate analysis indicated that the presence of RF, foot-dominant CJD pattern, and wrist-dominant CJD pattern are possible predictors of severe disease. High ACPA levels and high BMI were predictors of erosion-dominant CJD pattern. Finally, the strong influence of hand and wrist involvement on quality of life was highlighted by the elevated HAQ-DI scores in patients with hand-dominant and wrist-dominant CJD patterns.
Several authors have investigated the relationship between RA severity and the presence of DRB1 SE or RA-related autoantibodies12,13,14,15,16. In our present study, we observed interesting associations of CJD patterns with SE alleles and autoantibodies. The predominance of erosion over space narrowing was associated with SE alleles as well as with the presence and titer of RF and ACPA. Interestingly, predominance of erosion was observed in 65% of RF-positive, ACPA-positive, SE-positive patients (triple-positive) while predominance of space narrowing was observed in 69% of patients with none of these markers (triple-negative). This marked phenotypic difference may indicate different pathophysiologic pathways in these 2 RA subphenotypes, which may indeed represent distinct diseases.
The associations of CJD patterns and morphometric characteristics may also provide intriguing insights. It is known that obese patients are at increased risk of developing RA (OR 3.74)17, and that proinflammatory activity of cytokines and adipokines has been observed in obesity-associated systemic inflammatory states18. It is possible that proinflammatory cytokines and adipokines contribute to a pattern of predominant bone destruction over joint space narrowing in patients with RA who have high BMI.
The well-known correlation between total SvdH score and disease duration represented a potential difficulty in classifying patients according to disease severity because there was a wide variation in disease duration in the cohort. This difficulty was handled by establishing a central interval for the correlation between disease duration and total SvdH score: patients whose data were outside the central interval boundaries in a 2-dimensional plot of disease duration versus total SvdH score were defined as having either mild or severe forms of RA relative to those whose data were within the central interval limits. Therefore, patients classified as having severe RA had SvdH scores higher than disease duration–matched patients classified as having mild disease. This classification was validated by the observed correlations (under this classification scheme) between severe RA and presence of ACPA and RF, correlations that have been established and extensively reported in the literature19,20,21,22,23. In addition, patients classified as having severe RA under this scheme used higher doses of prednisone than those classified as having mild RA. RA severity was not associated with the distribution of DRB1 alleles. The lack of association of SE alleles and disease severity may have been influenced by the unique and highly blended ethnic composition of the Brazilian population, because it is known that the association of SE alleles and disease severity varies according to ethnicity24. In addition, all patients were attending tertiary university centers, which probably contributed to a bias toward underrepresentation of benign forms of the disease. Finally, many of our patients had disease duration of more than 8 years, when the association between SE alleles and disease severity is less evident25. Another peculiarity of the present series is the low rate of use of immunobiological therapy. The use of this type of therapy is lower in Brazil than in North America and Europe. At the time this series of patients was sampled, use of biologicals was very low in Brazil.
Our present study has introduced the concept of patterns of CJD in RA and proposed an objective approach to distinguish these patterns. Despite some inherent limitations, including the transversal approach, heterogeneous therapeutic regimens and wide range of disease duration, this preliminary study has allowed us to define and characterize the distribution of 3 CJD patterns in a large cohort of patients with RA. We identified intriguing associations between CJD patterns and morphometric measurements, clinical features, autoantibody profile, and SE alleles, which might provide important clues to the mechanisms underlying the development of preferential CJD patterns in RA. Future studies will aim to confirm these findings and explore the relationship between CJD patterns and additional aspects of RA heterogeneity, such as the response to therapy and the effect of environmental factors on the modulation of disease phenotype.
Acknowledgment
We thank Valdecir Marvulle, PhD, for guidance and assistance with statistical analyses, and Mary Chaiken, PhD, for expert English review.
- Accepted for publication November 14, 2014.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.