

Abstract
Objective. To determine whether a double dose of intraarticular triamcinolone acetonide is more effective for knee arthritis than a 40-mg dose.
Methods. In this 12-week randomized controlled clinical trial, 40 mg and 80 mg of intraarticular triamcinolone acetonide were compared in patients with knee arthritis. Evaluated variables included a Likert burden scale, visual analog scale pain scale, degree of arthritis activity, presence of swelling, and presence of functional limitation.
Results. Ninety-seven patients were randomized. No significant differences were observed between the groups regarding any outcomes.
Conclusion. An 80-mg dose of triamcinolone acetonide had no additional benefit compared with 40 mg as treatment for knee arthritis. Trial registration: Nederlands Trial Register; trial registration number: NTR2298.
Intraarticular corticosteroid injections are a widely used and recommended therapy for either rheumatoid arthritis (RA) or osteoarthritis (OA)1,2. Side effects are mainly related to discomfort from the procedure, localized pain post injection, and flushing3. The knee injection is the best studied intraarticular injection4. Efficacy has been established for knee arthritis associated with RA, OA, and juvenile idiopathic arthritis (JIA) in terms of pain relief and functional improvement for months, up to a year after injection5.
A survey among members of the American College of Rheumatology (ACR) showed variation in corticosteroid dosages used for intraarticular injections6. Although the majority used 40 mg for knee injections, almost 40% used another dosage. A Cochrane metaanalysis on intraarticular steroid injections for JIA and RA stated that “there is some suggestion that the effectiveness of intraarticular steroid may be dose-related.”7 Robinson, et al described a somewhat similar finding when comparing 40 mg and 80 mg of methylprednisolone as treatment for hip OA8. However, the ACR has not given recommendations on intraarticular dosages1,2. The dosages being administered are still determined by clinical tradition.
Because side effects are not an important issue of corticosteroid injections, the main problem is degree and duration of response. We hypothesized that a higher amount of corticosteroid in the target compartment could be related to a greater relief of symptoms and a prolonged local effect. The main objective of our study was to investigate whether a higher dose of intraarticular corticosteroid was related to greater symptomatic relief than a conventional dose as treatment for knee arthritis.
MATERIALS AND METHODS
We conducted a double-blind, randomized, controlled clinical trial in which a usual dose of 40 mg intraarticular triamcinolone acetonide was compared with a double dose of 80 mg as treatment for knee arthritis.
Patients
Adult patients with symptomatic synovitis of 1 knee and having an indication for intraarticular corticosteroid injection, at the discretion of the attending rheumatologist, were consecutively enrolled. Symptomatic was defined as a score of at least 3 on a 5-point Likert patient scale for burden of arthritis symptoms. An additional inclusion criterion was the use of stable antirheumatic medication. Exclusion criteria were the diagnosis of gout, contraindications for intraarticular corticosteroid injection, and use of more than 10 mg prednisone daily.
Study design
This was a 12-week multicenter, double-blind, randomized, controlled clinical trial at 2 investigational centers.
Patients were randomly assigned to either the low-dose group (40 mg triamcinolone acetonide) or the high-dose group (80 mg). Randomization was achieved by means of a randomization list stratified by hospital, based on a random number generator. The injections were prepared by an independent research nurse in a separate room. No anesthetics were added. All syringes had a volume of 2 ml and the content of all syringes was visually concealed, thereby ensuring complete blinding for patient and rheumatologist.
At baseline the following variables were recorded: type of underlying rheumatic condition [RA, psoriatic arthritis (PsA), other (including OA), unknown], duration of the knee arthritis, a 5-point Likert patient scale for burden of arthritis symptoms (none, little, moderate, much, very much), a patient 100-mm visual analog scale (VAS) for pain, a 5-point scale for arthritis activity (none, mild, moderate, active, very active) by the attending rheumatologist, as well as presence of swelling and functional limitation (defined as an inability to extend 0°). During the procedure of injection, the volume of aspirated knee joint fluid was measured. After assessment of baseline variables, the rheumatologist performed the injection. Once weekly, up to Week 12, patients completed a questionnaire with the Likert scale and the VAS, as described. At Week 12, during the second visit to the clinic, the following variables were recorded by the rheumatologist: a 5-point scale for arthritis activity, presence of swelling, and presence of functional limitation. Our 5-point Likert patient scale is analogous to the target joint pain score (pain of a 5-point Likert patient scale), which proved to be a reliable single-joint outcome measure for determining response in inflammatory arthritis9.
The primary endpoint was the percentage of patients with good response, which was defined as a positive change ≥ 2 points on the 5-point Likert scale for burden from baseline at weeks 11 and 12. The main secondary outcomes were the courses over time of Likert burden scores and VAS pain scores. Other secondary outcomes were, at Week 12, the percentages of patients with no arthritis activity on the 5-point scale, loss of swelling, and normalization of functional limitation.
Patient data were excluded for the primary endpoint and other 12-week outcomes when, during the study, patients received an additional intraarticular injection, antirheumatic medication was altered, or knee surgery was performed. Data until the moment of exclusion were used for analysis.
Statistical analysis
Analyses were performed using SPSS Version 22.0. A p < 0.05 was considered statistically significant. We postulated that a 30% difference on the primary endpoint would be clinically significant. Assuming that the proportion of good responders would be 30% in the control group of 40 mg, using a 5% significance level and 80% power, 42 patients were needed in each treatment group. The independent samples t test and Wilcoxon rank-sum test were used for, respectively, normally and non-normally distributed continuous variables. The chi-square test (or Fisher’s exact test) was used for dichotomous variables. Repeated measurements analyses were performed for comparison of Likert burden scores and VAS pain scores over time. The McNemar test was performed for analysis of improvement of both swelling and functional limitation.
Our study was approved by the Medical Ethical Committee Twente in Enschede, the Netherlands. All patients provided written informed consent.
RESULTS
Study population
Ninety-seven patients (mean age 58 yrs, 41% male) were included and randomized. Baseline characteristics are presented in Table 1 and did not differ significantly between the treatment groups. RA and PsA together made up the majority of underlying rheumatic conditions. Median knee arthritis duration was 4 weeks. During the study, 4 patients underwent knee surgery and 8 patients received another intraarticular injection. Of these 8 patients, only 3 received this injection in the same knee. Another 2 patients were lost to followup, 1 immediately and 1 after Week 11. The dropout rate was similar in both groups.
Baseline demographic and disease-related characteristics. Data are n (%) unless otherwise indicated.
Outcomes
There was no difference between the groups on the primary endpoint, with 49% good responders in the 40-mg group and 55% in the 80-mg group (p = 0.586). Both groups showed rapid response to the injection, with good response at Week 1 in more than half of patients in both groups (data not shown).
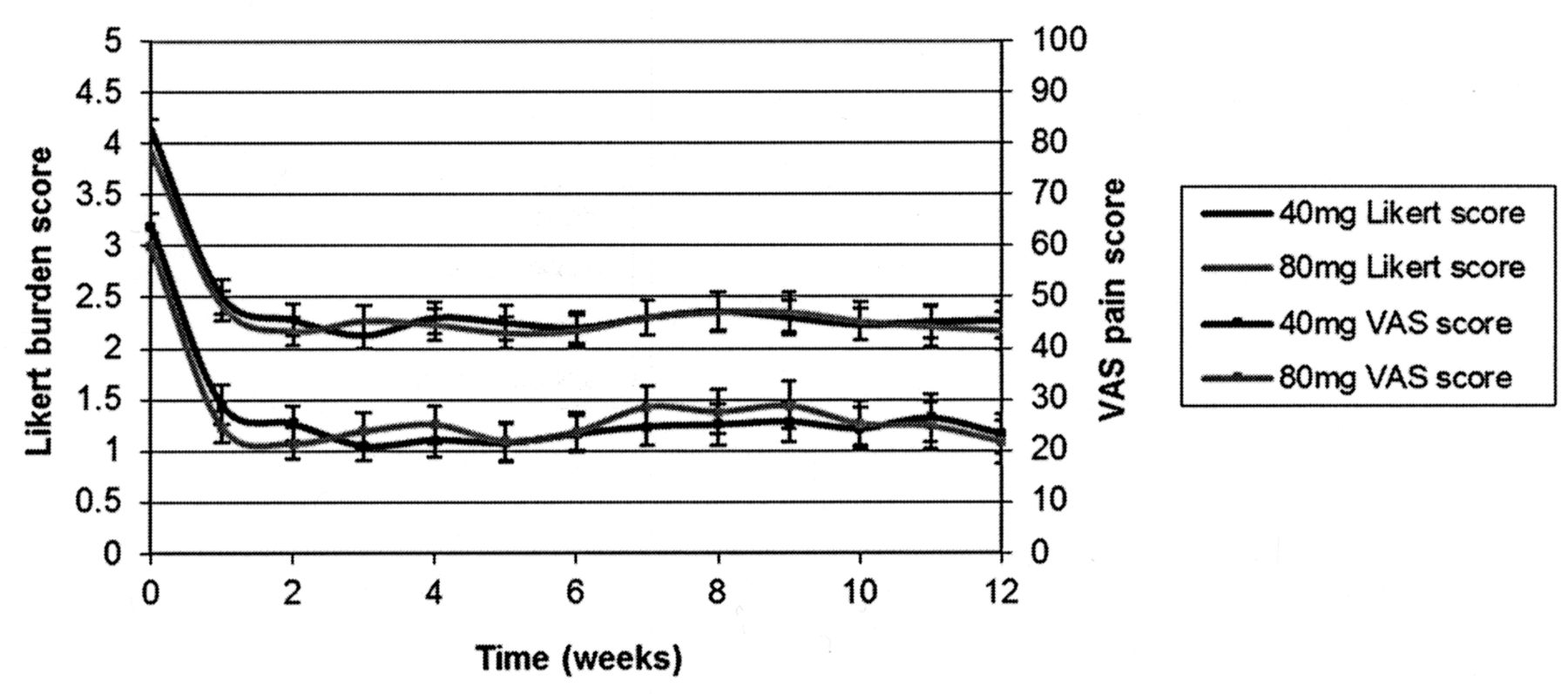
The courses of Likert burden scores and VAS pain scores over time are displayed in Figure 1. The 40-mg curves run the same course as the 80-mg curves. This course of both Likert and VAS scores is characterized by a rapid decline in Week 1 and relative stability from Week 1 through Week 12. Repeated measurements analysis showed no difference between the Likert curves (p = 0.849) and VAS curves (p = 0.572) of both groups.
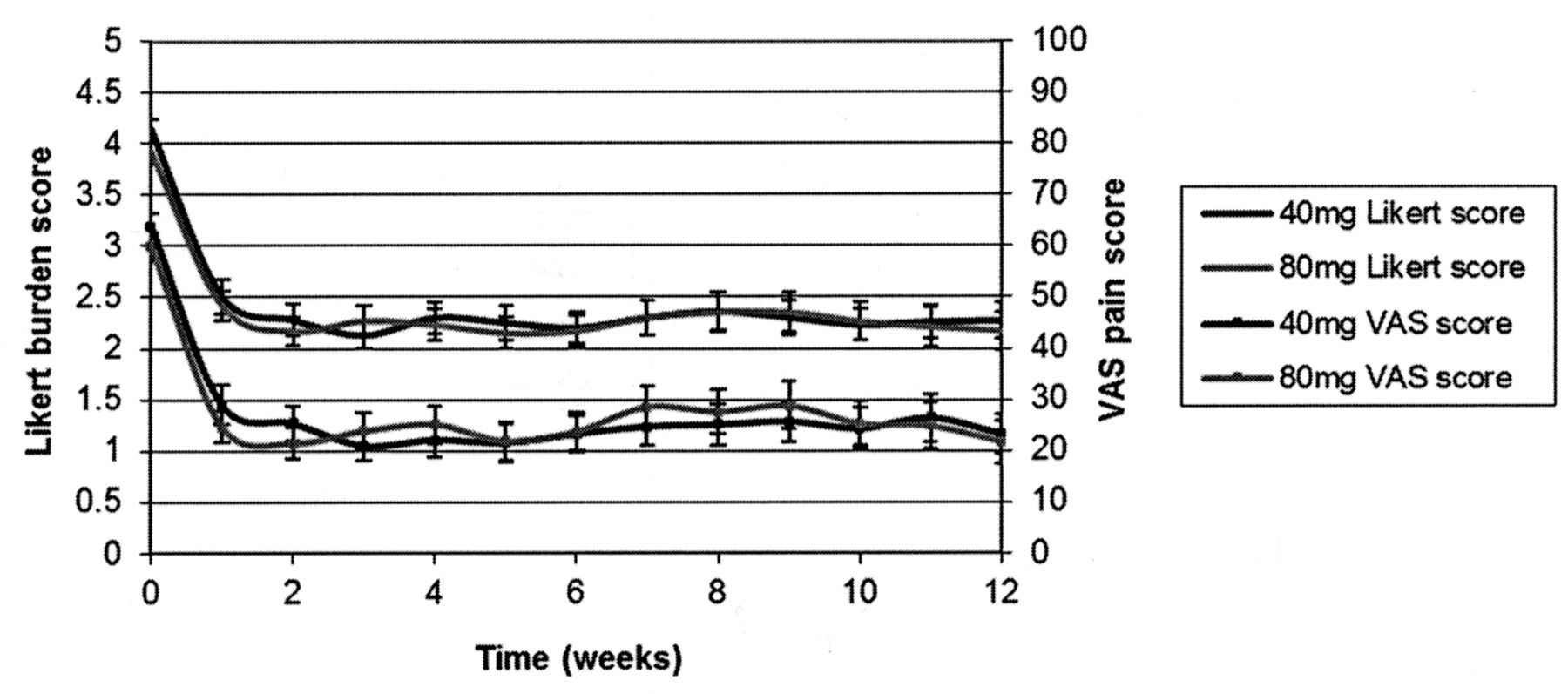
The courses of Likert burden scores and visual analog scale (VAS) pain scores over time.
No significant differences were observed concerning good response at Week 12 regarding arthritis activity, presence of swelling, and presence of functional limitation (Supplementary Tables 1, 2, and 3, available online at jrheum.org). At Week 12, 59% in the 40-mg group had no arthritis activity versus 63% in the 80-mg group (Supplementary Table 1). In the 40-mg group, 63% of patients with baseline swelling had no swelling at Week 12 versus 67% in the 80-mg group (Supplementary Table 4). In functional limitation, those percentages were 70% for the 40-mg group and 60% for the 80-mg group (Supplementary Table 5). The presence of swelling declined over time in both groups (p < 0.001), whereas the presence of functional limitation declined only in the 40-mg group (40 mg, p = 0.180; 80 mg, p = 1.00).
DISCUSSION
Our study demonstrated no difference in efficacy between 40-mg and 80-mg doses of intraarticular triamcinolone acetonide for knee arthritis during a 12-week followup. This suggests that both doses are in the plateau phase of the dose-response relationship of intraarticular triamcinolone acetonide.
Combining our results with preceding studies suggests that the dose-response relationship is linear up to 40 mg of corticosteroid, followed by a plateau phase with higher dosages10,11. Our study is the first, to our knowledge, to compare 40 mg and 80 mg of the same corticosteroid for knee arthritis. It is in line with the study by Robinson, et al, comparing 40 mg and 80 mg of methylprednisolone for hip OA, but we also studied arthritis due to rheumatic conditions other than OA8.
The 5-point Likert patient scale for burden of arthritis symptoms was chosen as primary outcome because the primary goal of intraarticular corticosteroid treatment is symptom reduction, and this is best reflected by a patient score. The classification of a beneficial change ≥ 2 points as good response was arbitrary, but this change seems to be a plausible significant clinical improvement nonetheless. Because we combined different causes for knee arthritis, it might be hypothesized that different underlying diseases have different dose-response relations. However, we investigated efficacy in different subgroups, revealing no different efficacy between the 2 doses and underlying diseases (data not shown).
Although this is a small investigator-driven low-budget study, it is well-conducted according to present standards.
Our study demonstrated a 12-week equal benefit from 40 mg and 80 mg intraarticular triamcinolone acetonide for knee arthritis. Therefore, based on our study, there is no need to change the currently preferred dose of 40 mg triamcinolone acetonide for knee arthritis.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
The authors gratefully acknowledge the contributions from the involved research nurses, clinical pharmacists, and rheumatologists, and all patients who participated in this study.
- Accepted for publication June 3, 2015.








{kind=link}