

Abstract
Objective. MicroRNA (miRNA) are small noncoding RNA that posttranscriptionally regulate gene expression and serve as potential mediators and markers of disease. Recently, plasma miR-24-3p and miR-125a-5p concentrations were shown to be elevated in rheumatoid arthritis (RA) and useful for RA diagnosis. We assessed the utility of 7 candidate plasma miRNA, selected for biological relevance, for RA diagnosis and use as markers of disease activity and subclinical atherosclerosis in RA.
Methods. The cross-sectional study included 168 patients with RA and 91 control subjects of similar age, race, and sex. Plasma concentrations of miR-15a-5p, miR-24-3p, miR-26a-5p, miR-125a-5p, miR-146a-5p, miR-155-5p, and miR-223-3p were measured by quantitative PCR. Utility of plasma miRNA concentrations for RA diagnosis was assessed by area under the receiver-operating characteristic curve (AUROC). Associations between plasma miRNA concentrations and RA disease activity and coronary artery calcium score were assessed by Spearman correlations.
Results. Plasma concentrations of miR-15a-5p, miR-24-3p, miR-26a-5p, miR-125a-5p, miR-146a-5p, miR-155-5p, and miR-223-3p were significantly increased in patients with RA. The highest AUROC for diagnosis of RA (AUROC = 0.725) was found in miR-24-3p, including among rheumatoid factor–negative patients (AUROC = 0.772). Among all patients with RA, the combination of miR-24-3p, miR-26a-5p, and miR-125a-5p improved the model modestly (AUROC = 0.747). One miRNA, miR-155-5p, was weakly inversely associated with swollen joint count (p = 0.024), but no other miRNA were associated with disease activity or coronary artery calcium score.
Conclusion. The combination of miR-24-3p, miR-26a-5p, and miR-125a-5p had the strongest diagnostic accuracy for RA. Candidate miRNA had little or no association with RA disease activity or subclinical atherosclerosis.
MicroRNA (miRNA) are small (about 22 nucleotides in length) noncoding RNA that bind to 3′ untranslated regions of mRNA and cause destabilization of transcription machinery or transcript degradation1,2,3. Each miRNA has the capacity to bind to many different mRNA transcripts, thus potentially affecting multiple distinct pathways. miRNA are differentially expressed within many cell types and are stable within extracellular fluids such as plasma, where they are protected within exosomes4, microvesicles5, lipoproteins6, and Argonaute2 protein complexes7. The association of miRNA with lipid and protein carriers in plasma confers extraordinary stability8,9. Their stability in plasma and known biological function within cells make them highly relevant to disease mechanisms and ideal candidates for diagnostic tests, disease biomarkers, and therapeutic targets.
Circulating miRNA have great potential as biomarkers in patients with rheumatoid arthritis (RA) to aid in diagnosis and disease activity monitoring, as well as prediction of cardiovascular risk, the main cause of early death in patients with RA10,11. Currently, there is little information regarding plasma miRNA in RA. More is known about cellular miRNA alterations and how these affect important cellular functions in RA. Examples include the role of miR-15a-5p in cellular apoptosis12,13, miR-24-3p in maintenance of autoreactive B cells14, miR-125a-5p and miR-223-3p in macrophage cytokine production15, and miR-26a-5p, miR-146a-5p, and miR-155-5p in interleukin 17 (IL-17)–producing T cells16. Alterations of several of these miRNA, such as miR-146a-5p and miR-155-5p, have been suggested to also play a role in the development of cardiovascular disease in RA17.
One study has reported that miR-24-3p and miR-125a-5p have diagnostic potential for RA18. We hypothesized that these 2 miRNA, along with miR-15a-5p, miR-26a-5p, miR-146a-5p, miR-155-5p, and miR-223-3p, may be useful biomarkers for RA diagnosis and disease activity. Because many of the miRNA with a role in the pathogenesis of RA19 overlap with those implicated in the development of atherosclerosis20,21, we also hypothesized that these miRNA may also serve as biomarkers of subclinical atherosclerosis in patients with RA.
MATERIALS AND METHODS
Study population
This was a cross-sectional study that included 168 patients with RA and 91 control subjects. This cohort is part of a group of patients extensively characterized for cardiovascular risk22. Recruitment and study procedures have been described22. All subjects were older than 18 years of age and patients with RA fulfilled American College of Rheumatology 1987 classification criteria for RA23. RA and control groups were frequency-matched for age, race, and sex and control subjects did not have RA or other inflammatory disease. The study was approved by the Vanderbilt Institutional Review Board and all subjects gave written informed consent.
Clinical and laboratory data
Clinical information and laboratory measurements were obtained as described22. Disease activity of RA was determined by the 28-joint Disease Activity Score (DAS28) using erythrocyte sedimentation rate (ESR) as the marker of inflammation24. Body mass index (BMI) was calculated and expressed as kg/m2. Framingham risk score for 10-year percent risk of a cardiovascular event was determined as described25,26.
Fasting cholesterol panel, ESR, and high-sensitivity C-reactive protein (CRP) were measured by the Vanderbilt University Medical Center Clinical Laboratory or by ELISA (Millipore). The degree of insulin resistance was calculated by the homeostatic model assessment of insulin resistance [HOMA; fasting glucose (mmol/l) × fasting insulin (μU/ml)/22.5]27. Coronary artery calcium score was measured by electron beam computed tomography with an Imatron C-150 scanner (GE/Imatron) as described22 and quantified in Agatston units28.
RNA isolation, cDNA synthesis, and quantitative PCR
Plasma (collected in EDTA-containing tubes) from each subject was stored at −80°C. RNA was extracted from 250 μl of plasma using a total RNA purification kit, in a 96-well format (Norgen). All plasma RNA samples were extracted at the same time. RNA was collected in a total volume of 100 μl in sequential 50 μl elutions. A volume of 5 μl of RNA from each subject was polyadenylated and used for first-strand cDNA synthesis (Quanta Biosciences). The cDNA was diluted 1:20 in Tris-EDTA buffer and stored at −20°C.
All miRNA assays (miR-15a-5p, miR-24-3p, miR-26a-5p, miR-125-5p, miR-146a-5p, miR-155-5p, and miR-223-3p) used 5 μl diluted cDNA in 20 μl final reaction volume (Quanta Biosciences) in a 96-well format on Bio-Rad CFX96 instruments. Cycling conditions consisted of a 3-min incubation at 95°C; 50 cycles of amplification at 95°C for 10 s then 60°C for 30 s; 95°C for 1 min; 55°C for 1 min, followed by an 80-step melt curve in 0.5°C increments from 55°C to 95°C. Technical replicates were performed in triplicate. Proportional numbers of RA and control cDNA samples, a no-cDNA template negative control, and a 4-point, 10-fold dilution standard of whole blood cDNA were included on each of 10 PCR plates for each miRNA assay. Quality control results for the miRNA assays are shown in Supplementary Table 1, available online at jrheum.org.
Quantitative PCR (qPCR) miRNA data were converted to molar concentrations using 1 zeptomole to 1 attomole serial dilution of qPCR miRNA mimics. Single-stranded DNA mimics were synthesized for miR-15a-5p, miR-24-3p, and miR-223-3p, each of which included the universal PCR primer sequence, a 2-base dA spacer, and the reverse complement of the miRNA assay primer sequence (IDT Inc.). Quality control results for the mimic standard dilutions are shown in Supplementary Table 2 (available online at jrheum.org), with nearly identical results for each. A composite curve including the 3 mimic dilution standards was used to convert qPCR data to molar amounts for each miRNA assay. All assays and analyses were done using applicable minimum Information for Publication of Quantitative Real-Time PCR Experiments guidelines29.
Statistical methods
Descriptive statistics were calculated as mean ± SD for continuous variables, and frequency and proportions for categorical variables. Wilcoxon rank sum tests were used to compare continuous variables and Pearson’s chi-square test to compare categorical variables.
To determine the utility of plasma miRNA for diagnosis of RA, receiver-operating characteristic (ROC) curves were plotted and area under the curve (AUROC) was calculated for each miRNA. For combinations of miRNA, logistic regression was used with the dependent variable as disease status (RA versus control), and the independent variable as the miRNA of interest. The predicted probability for RA diagnosis determined from the logistic regression was plotted in an ROC curve and AUROC was calculated. Spearman correlation coefficients for continuous variables and Wilcoxon rank sum tests for categorical variables were used to determine the association between plasma miRNA concentrations and variables of interest pertaining to RA disease activity and cardiovascular risk.
Statistical analyses were performed using IBM SPSS Statistics v22. Two-sided p values ≤ 0.05 were considered statistically significant.
RESULTS
Clinical characteristics
As described22,30, clinical characteristics of patients with RA and control subjects are presented in Table 1. Patients and controls were of similar age, race, and sex. Patients with RA had moderate disease activity with a mean DAS28 score of 3.79, and higher CRP than controls (p < 0.001; Table 1). The majority of patients with RA were rheumatoid factor (RF)-positive (69%), and taking methotrexate (MTX; 71%) and prednisone (54%; Table 1). Patients with RA had greater waist circumference and lower low-density lipoprotein cholesterol (LDL-C) than control subjects (Table 1).
Patient characteristics. Presented as mean ± SD, unless otherwise indicated.
Diagnostic capacity of candidate miRNA for RA
Patients with RA had higher plasma concentrations compared to control subjects of miR-15a-5p (2.7-fold, p < 0.001), miR-24-3p (3.5-fold, p < 0.001), miR-26a-5p (1.8-fold, p < 0.001), miR-125a-5p (1.2-fold, p = 0.003), miR-146a-5p (2.5-fold, p < 0.001), miR-155-5p (2.7-fold, p < 0.001), and miR-223-3p (2.5-fold, p < 0.001; Table 2). The AUROC for RA diagnosis using individual miRNA ranged from 0.610 to 0.725, with miR-24-3p having the highest AUROC (Table 2). The combination of miR-24-3p, miR-26a-5p, and miR-125a-5p had the highest AUROC for RA diagnosis (AUROC = 0.747, 95% CI 0.683–0.810; Figure 1). The combination of miR-24-3p and miR-125a-5p, as reported18, had a similar AUROC for RA diagnosis (AUROC = 0.732, 95% CI 0.669–0.796).
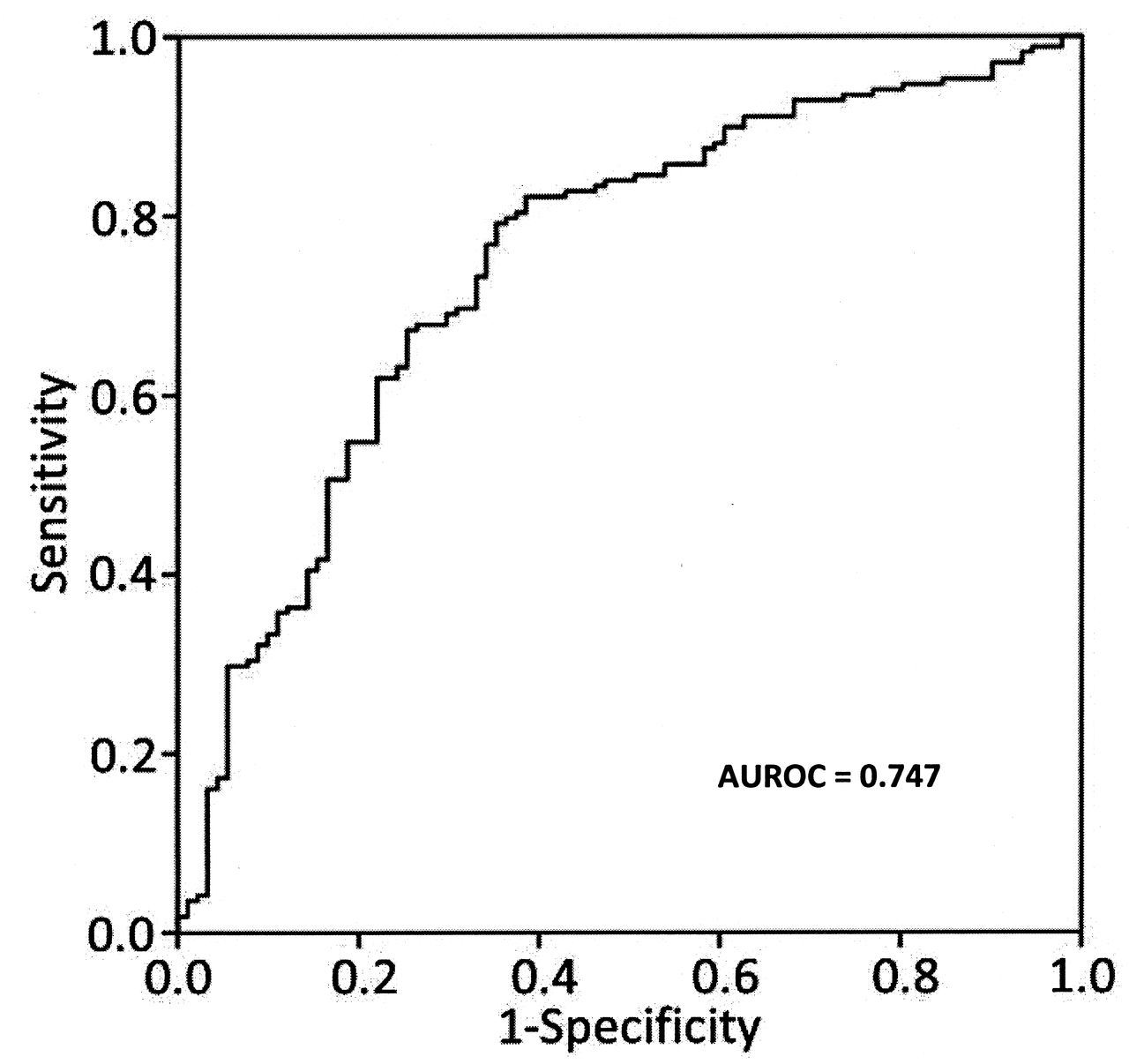
Predictive capacity of the combination of miR-24-3p, miR-26a-5p, and miR-125a-5p for RA diagnosis. Receiver-operating characteristic curve was made using the combination of plasma concentrations of miR-24-3p, miR-26a-5p, and miR-125a-5p. The area under the curve (AUROC) = 0.747 for diagnosis of RA with this combination of miRNA. miRNA: microRNA; RA: rheumatoid arthritis.
Candidate plasma microRNA (miRNA) concentrations in RA versus control plasma and area under the receiver-operating characteristic curve for RA diagnosis. miRNA concentrations presented as mean ± SD.
Comparing patients with RA who were RF-negative to control subjects, all miRNA were significantly elevated (all p < 0.003) except for miR-125a-5p (Supplementary Table 3, available online at jrheum.org). Moreover, miR-24-3p maintained the highest AUROC for RA diagnosis (AUROC = 0.772, 95% CI 0.688-0.857; Supplementary Table 3, and Supplementary Figure 1, available online at jrheum.org), although the combination of miR-24-3p, miR-26a-5p, and miR-125a-5p was similar (AUROC = 0.764, 95% CI 0.680–0.848).
Relationship to disease-related factors and medications in miRNA expression
We evaluated the utility of the 7 candidate miRNA for use as biomarkers of disease activity. Only miR-155-5p was weakly inversely correlated with swollen joint count in patients with RA (ρ −0.174, p = 0.02), and no other miRNA were correlated with DAS28 score, tender joint count, global health score, ESR, or CRP (all p > 0.08; Supplementary Table 4, available online at jrheum.org). Moreover, medication use including MTX, leflunomide, hydroxychloroquine, anti-tumor necrosis factor (TNF)-α agents, corticosteroids, and nonsteroidal antiinflammatory drugs were not associated with altered concentrations of any of the 7 miRNA evaluated (all p > 0.1).
Relationship to subclinical atherosclerosis and CV risk factors in miRNA expression
We next determined whether these 7 miRNA were associated with cardiovascular risk factors in patients with RA. None of the 7 miRNA were associated with coronary artery calcium score in RA (all p > 0.1; Supplementary Table 5). We found that miR-26a-5p was weakly associated with Framingham risk score (ρ 0.150, p = 0.05). There was a weak association with systolic blood pressure for miR-125a-5p (ρ 0.198, p = 0.01), but none with the diagnosis of hypertension (all p > 0.1). Two miRNA, miR-15a-5p and miR-24-3p, were modestly associated with waist circumference (ρ 0.185, p = 0.02 for miR-15a-5p; and ρ 0.208, p = 0.01 for miR-24-3p; Supplementary Table 5, available online at jrheum.org). None of the candidate miRNA were associated with traditional lipid profile (total cholesterol, LDL-C, high-density lipoprotein cholesterol, or triglycerides), smoking status, degree of insulin resistance (HOMA), or diabetes in patients with RA (all p > 0.05).
DISCUSSION
We found that miR-15a-5p, miR-24-3p, miR-26a-5p, miR-125a-5p, miR-146a-5p, miR-155-5p, and miR-223-3p concentrations were elevated in the plasma of patients with RA. The combination of miR-24-3p, miR-26a-5p, and miR-125a-5p performed best to differentiate between patients with RA and control subjects, although the performance of the other miRNA did not differ meaningfully from these. Among RF-negative patients, miR-24-3p was a strong marker of RA. Among the miRNA tested, only miR-155-5p was weakly inversely associated with RA disease activity (swollen joint count). Moreover, there was little to no association between the plasma concentrations of the candidate miRNA and subclinical atherosclerosis or cardiovascular risk factors.
Our findings are consistent with a study by Murata, et al in which concentrations of miR-24-3p and miR-125a-5p had the best diagnostic utility for RA, and miR-26a-5p was also helpful18. However, we found that miR-24-3p rather than miR-125a-5p or a combination of miRNA was a better diagnostic tool in seronegative RA, which differs slightly from the previous study, which found that miR-125a-5p or the combination of miR-24-3p and miR-125a-5p was more accurate than miR-24-3p alone in seronegative (anticitrullinated peptide antibody) RA18. Comparing the current study with Murata, et al18, the fold increase comparing RA to control subjects in miR-24-3p was 3.5 in the current study and 3.75 in the prior study; the fold change in miR-26a-5p was 1.8 in the current study and 2.85 in the prior study; and the fold change in miR-125a-5p was 1.2 in the current study and 2.7 in the prior study. In the same study, plasma concentrations of miR-125a-5p did not correlate with indices of inflammation or disease activity, consistent with our findings.
In contrast to our results, miR-24-3p was positively correlated with some indices of disease activity including CRP, global health, and DAS28, but not ESR or tender or swollen joint count18. The previous study18 selected initial candidate miRNA from profiling results of a very small number of subjects (3 patients with RA and 3 control subjects); thus, important miRNA may not have been identified and studied. Therefore, we examined miRNA that were most strongly associated with RA in the previous study and also selected additional candidate miRNA that have been identified as having biological relevance to RA.
Two smaller studies compared selected circulating miRNA in patients with RA and control subjects. One included 30 patients with RA, 30 patients with osteoarthritis, and 30 healthy control subjects in a study measuring plasma miRNA8, and the second included 34 patients with treatment-naive early RA, 28 patients with late RA, and 16 healthy control subjects in a study measuring serum miRNA31. Both studies found that miR-146a-5p, miR-155-5p, and miR-223-3p levels were not different in patients with established RA compared to control subjects; however, both of these studies compared RA and control subjects without age- or sex-matching (e.g., about 15–18–year mean age difference between groups in both studies), and these factors may alter circulating miRNA32,33. Also, there have been problems with the reproducibility of findings with miR-146a-5p, miR-155-5p, and miR-223-3p in other studies. For example, in another inflammatory autoimmune disease, systemic lupus erythematosus, findings with plasma miR-146a-5p and miR-223-3p were not replicated in exploratory and validation cohorts34. Moreover, the relatively low abundance of plasma miR-155-5p may make it less reproducible across studies.
A recent study evaluated miRNA as possible predictors of response to therapy in RA35. Microarrays of miRNA were performed on sera of 10 patients with RA before and 6 months after starting disease-modifying antirheumatic drug (DMARD) or anti-TNF-α therapy. A subset of differentially expressed miRNA with relevance to inflammation, immune response, musculoskeletal system, or connective tissue were chosen to validate in a larger cohort of 85 patients with RA on paired serum samples. In this study, miR-146a-5p and miR-223-3p, among others, were significantly increased after DMARD/anti-TNF-α therapy, and miR-223-3p (along with miR-23) were predictors of response35.
The plasma miRNA that were most strongly associated with RA in our study (miR-24-3p, miR-26a-5p, and miR-125a-5p) appear to be reproducible18 and relevant to processes underlying RA. The miR-24-3p mediates plasma cell survival and is increased with plasma cell exposure to IL-614. Thus, miR-24-3p may contribute to RA by maintaining autoreactive plasma cells. One factor that may contribute to the high plasma levels of miR-26a-5p, miR-155-5p, and miR-146a-5p in patients with RA is increased IL-17–producing T cells16. Within macrophages, miR-125a-5p may have a role in modulating the inflammatory response. For example, in mouse bone marrow–derived macrophages, activation of Toll-like receptors 2 and 4 increased miR-125a-5p expression, and miR-125a-5p promoted an antiinflammatory cell phenotype36. Conversely, miR-125a-5p amplified the inflammatory response by repressing a negative regulator of NF-κB signaling in human THP-1 cells37.
The other plasma miRNA examined, which were elevated among patients with RA, also have important biologic functions in RA. One of the most widely studied is miR-146a-5p, which is increased in many cell types in RA such as synovial fibroblasts, peripheral blood mononuclear cells, CD4+ T cells, and Th17 cells, and acts as a negative regulator of nuclear factor-κB (NF-κB) activation (reviewed38). Another is miR-155-5p, a major regulator of B cell development and function, T cell dependent antibody responses, and T cell functions (reviewed39). Also, miR-223-3p modifies inflammation through several pathways, by decreasing monocyte IL-1b production and T cell IL-10 production (reviewed39,40).
In addition to their association with RA and inflammation, many of the miRNA we examined have a relationship to cardiovascular disease. Two key examples are miR-223-3p and miR-146a-5p. The miRNA miR-223-3p decreases cholesterol biosynthesis and enhances cholesterol efflux41. Moreover, delivery of miR-223-3p to endothelial cells decreased adhesion molecule expression42, a key factor in the development of atherosclerosis. Concentrations of miR-146a-5p were increased in the plasma and peripheral blood mononuclear cells of patients with acute coronary syndrome43, and miR-146a-5p affects endothelial function by regulation of nitric oxide production44. Nevertheless, these plasma miRNA were not associated with coronary artery calcium score.
Our study has some limitations. For example, we used a candidate miRNA approach to evaluate key miRNA thought to be important in the development of RA. A drawback of this method is that the miRNA field is rapidly expanding; therefore, potentially important miRNA were likely not included. Also, we did not study patients with other inflammatory autoimmune diseases such as systemic lupus erythematosus or psoriatic arthritis, to determine whether the miRNA examined here may differentiate between RA and other inflammatory autoimmune diseases. Future studies to evaluate this will be interesting, particularly given our findings in seronegative RA, a condition in which alternative diagnoses are often considered and an additional diagnostic tool would be very useful.
The miRNA miR-15a-5p, miR-24-3p, miR-26a-5p, miR-125a-5p, miR-146a-5p, miR-155-5p, and miR-223-3p are all elevated in the plasma of patients with RA. The strongest diagnostic accuracy for RA exists in miR-24-3p, miR-26a-5p, and miR-125a-5p, and miR-24-3p had the strongest diagnostic accuracy for seronegative RA. Among the candidate miRNA evaluated, miR-155-5p was inversely associated with swollen joint count. None of the candidate miRNA were associated with coronary artery atherosclerosis in RA.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Footnotes
Funding from the Arthritis Foundation Clinical to Research Transition Award, American College of Rheumatology Research Foundation; US National Institutes of Health Grants: P60 AR056116, P01HL116263, KL2TR000446, and Clinical and Translational Science Award UL1TR000445 from the US National Center for Advancing Translational Sciences. This article’s contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
- Accepted for publication June 4, 2015.








{kind=link}