

Abstract
Objective. Increased levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) are associated with cardiovascular morbidity and mortality. Inflammation may also affect levels of NT-proBNP. We investigated the relationship of NT-proBNP with inflammation, disease activity, disease severity, and progression of Takayasu arteritis (TA).
Methods. Plasma levels of NT-proBNP were determined in 68 patients with TA and in 90 control subjects. Disease activity and disease severity in patients with TA were defined according to the National Institutes of Health and Ishikawa’s criteria, respectively.
Results. NT-proBNP levels were higher in patients with active disease (915.0 ± 328.0 pmol/l) and patients in remission (618.2 ± 243.4 pmol/l) than in controls (427.2 ± 81.4 pmol/l) (p < 0.001). Patients with severe TA showed significantly higher NT-proBNP levels than those with mild-moderate TA (924.0 ± 332.4 pmol/l vs 653.8 ± 269.1 pmol/l; p = 0.001). In patients with longitudinal data, NT-proBNP levels at the active phase were significantly higher than those at the stable phase (944.1 ± 216.7 pmol/l vs 552.1 ± 178.2 pmol/l; p = 0.001). Inflammatory markers, including C-reactive protein, erythrocyte sedimentation rate, and white blood cell count, were independently associated with NT-proBNP levels after adjustment for other confounding factors (R2 adjusted = 0.307, p = 0.001).
Conclusion. NT-proBNP levels were significantly increased in patients with active TA exhibiting complications. NT-proBNP levels were independently associated with inflammation. These results indicate that NT-proBNP may be a useful marker to assess the status, severity, and progression of TA.
Takayasu arteritis (TA) is a chronic nonspecific inflammatory disease, which primarily involves the aorta, its main branches, and pulmonary and coronary arteries. Vessel wall inflammation causes luminal stenosis, occlusion, dilation, or aneurysm formation1. Patients with TA suffer premature mortality because of cardiovascular diseases (CVD)2,3,4. Increased CVD in patients with TA cannot be explained by traditional cardiovascular risk factors alone; as such, an active disease status may contribute to the development and progression of these complications3,4. Therefore, accurate assessment and aggressive control of disease activity are clinically important to decrease vasculitic lesions and mortality caused by TA. However, conventional measures of disease status such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) have been reported to lack sensitivity and specificity5,6. In the analysis of the US National Institutes of Health (NIH) study, ESR was elevated in only 72% of patients with active disease and was still high in 56% of patients in remission5. It is therefore crucial to identify more sensitive and conventional markers of underlying disease activity to improve the clinical management of patients with TA.
N-terminal pro-brain natriuretic peptide (NT-proBNP), a diuretic peptide synthesized and secreted mainly in the cardiac ventricles in response to myocyte stretch7, has been considered a useful marker to evaluate the risk of CVD8,9,10. Studies have suggested that NT-proBNP is also associated with inflammatory factors11,12,13,14. Previous studies showed that the plasma levels of NT-proBNP are higher in patients with systemic inflammatory diseases, such as rheumatoid arthritis (RA) and systemic lupus erythematosus, than in control groups15,16. Solus, et al15 also found that NT-proBNP concentrations are correlated with inflammatory markers and disease activity in patients with RA. TA is characterized by vasculitic lesions, which may increase arterial stiffness in central elastic arteries17. Increased arterial stiffness can lead to earlier arrival of the reflected pulse waves and increase left ventricular afterload, thus stimulating BNP release18. Thus, we determined whether NT-proBNP concentrations are increased in patients with TA. We also investigated whether these concentrations are associated with inflammatory markers, disease activity, severity, and progression.
MATERIALS AND METHODS
Patients and controls
Among a cohort of 156 patients who satisfied the American College of Rheumatology classification criteria for TA19 in Fuwai Hospital from 2011 to 2013, 68 patients were included in this study. Ninety unrelated subjects matched for age, sex, and body mass index (BMI) who had routine health examinations over the same period were enrolled as healthy controls without clinical risk factors or echocardiographic abnormalities. Patients with cardiac failure, coronary artery disease, renal dysfunction (serum creatine > 1.5 mg/dl), and other inflammatory diseases were excluded. Echocardiography was performed in all participants. The following patients were also excluded: those who had moderate/severe valvular disease; those exhibiting < 55% left ventricular ejection fraction; and those with left ventricular end-diastolic diameter > 55 mm. The study protocol was approved by the Institutional Ethics Committee of the Fuwai Hospital, and all participants signed an informed consent.
Classification criteria
TA is classified into 4 types according to the Lupi-Herrera criteria: type I, arteritis affecting the aortic arch and its major branches; type II, arteritis affecting the thoracic and abdominal aorta; type III, arteritis affecting the whole aorta; and type IV, arteritis affecting the pulmonary artery20.
Disease activity and severity assessment
The disease activity in patients with TA was assessed according to the NIH criteria5. Active disease was considered if a patient presented new onset or worsening of at least 2 of the following features: (1) systemic symptoms without infection; (2) characteristics of vascular ischemia or inflammation, such as claudication, vascular pain (carotodynia), bruit, or asymmetry in pulses or blood pressure; (3) an increase in ESR; and (4) typical angiographic characteristics.
The disease severity of TA was classified into 4 groups according to Ishikawa’s criteria: group I, patients without a complication; group II, patients with a single complication, which was subdivided according to the severity of complication (Group IIa, with mild or moderate form, and Group IIb, severe form); and group III, those with 2 or more complications21. For comparison, groups I and IIa were combined as a mild-moderate group; Groups IIb and III were combined as a severe group in our study.
Laboratory tests
Blood samples were collected from the participants after an overnight fast to measure complete blood count, ESR, CRP, NT-proBNP, and other biochemical indexes. ESR was determined by Westergren method. CRP was measured using a high sensitivity assay-immunonephelometry. NT-proBNP was determined using specific NT-proBNP assay kits (Biomedica). The intra- and inter-assay coefficient of variation was below 5% and 10%.
Statistical analysis
Continuous data are presented as mean ± standard deviation (SD), and categorical data are expressed as total number (percentage). Kolmogorov-Smirnov test was used to evaluate the normal distribution of the numerical data. Differences between the groups were assessed using one-way ANOVA and posthoc least significant difference tests, independent t-test or Mann-Whitney U test for continuous data, and chi-square test or Fisher’s exact test for categorical variables. In patients whose paired samples were collected, the paired t-test was used to determine the differences in the continuous variables between active and stable stages. Correlations between numerical variables were analyzed using Pearson’s correlation coefficient. Multiple linear regression analysis was used to investigate the independent association between NT-proBNP and inflammatory markers in patients with TA. In Pearson’s correlation coefficient and regression analyses, ESR and CRP were log-transformed to obtain normality. In all of the analyses, a 2-sided significance level of 0.05 was used (SPSS 17.0; SPSS Inc.).
RESULTS
Patient characteristics
Table 1 shows the clinical characteristics of 68 patients with TA and 90 healthy controls. The average age of patients with TA was 36.4 ± 12.6 years and 91.2% were women. A total of 30 patients (44.1%) were in the active phase of the disease, and severe TA was observed in 24 patients (35.3%) at the outset of the study. Based on the classification criteria, Type III (43.3%) was the most frequent type in active TA, whereas Type I (39.5%) was the most common type in inactive TA.
Characteristics of patients with Takayasu arteritis (TA) and controls.
NT-proBNP and TA activity
NT-proBNP concentrations were significantly increased in patients with active TA (915.0 ± 328.0 pmol/l) compared with those in inactive patients (618.2 ± 243.4 pmol/l) (p < 0.001), and the concentrations in both of the TA groups were higher than those in the control subjects (427.2 ± 81.4 pmol/l, p < 0.001; Figure 1). Inflammation measures, including, ESR, CRP, and white blood cell (WBC) count, were significantly higher in patients with active TA than patients in remission (Table 1).
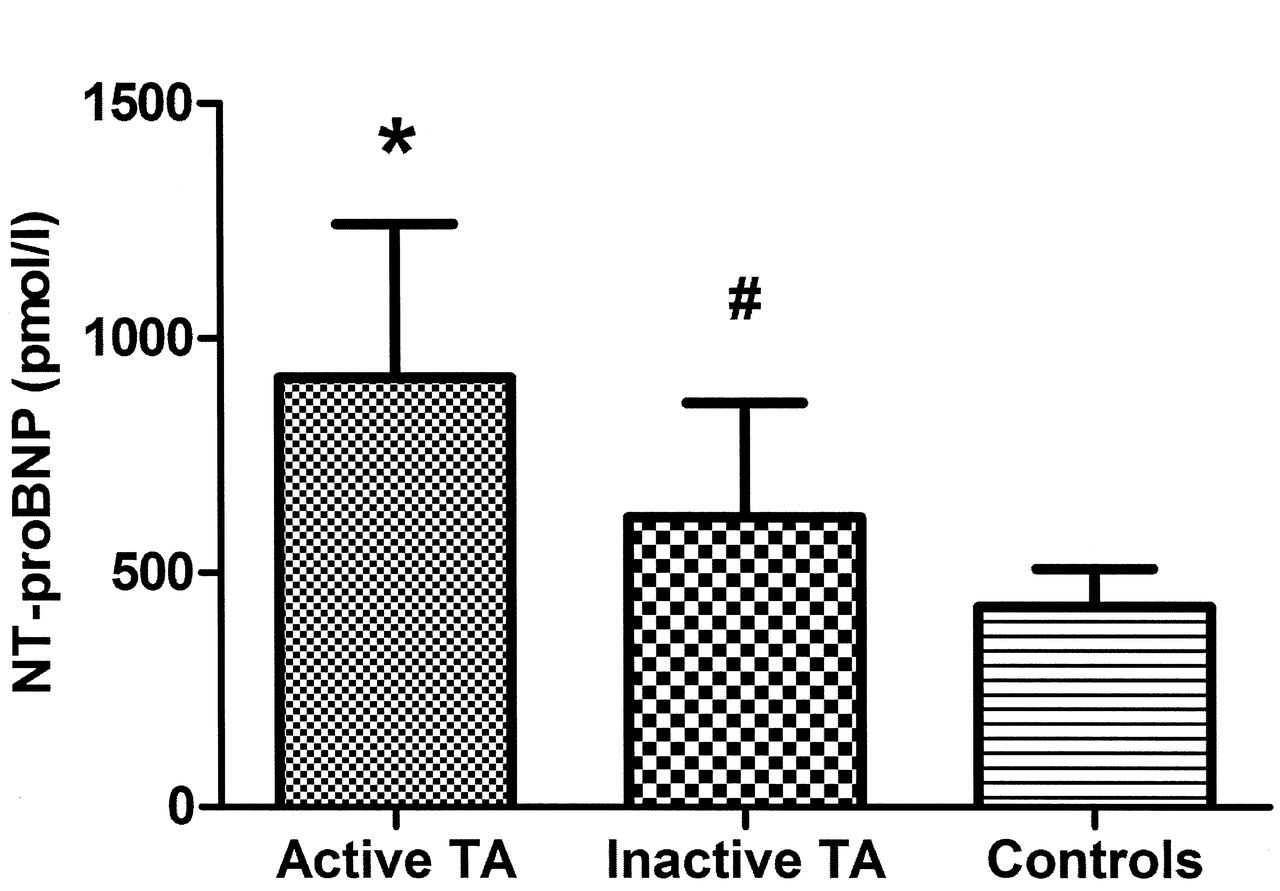
N-terminal pro-brain natriuretic peptide (NT-proBNP) concentrations in patients with Takayasu arteritis (TA) and controls. *p < 0.001 vs inactive TA and controls. #p < 0.001 vs controls.
Longitudinal data were obtained in 10 patients, and the mean interval between different disease stages was 12.6 ± 12.0 months. The mean levels of NT-proBNP at the active stage were significantly higher than those at the stable stage (944.1 ± 216.7 pmol/l vs 552.1 ± 178.2 pmol/l; p = 0.001; Figure 2), as well as levels of ESR (26.3 ± 16.6 mm/h vs 7.5 ± 4.8 mm/h; p = 0.005) and CRP (6.2 ± 4.8 mg/l vs 3.0 ± 2.5 mg/l; p = 0.026).
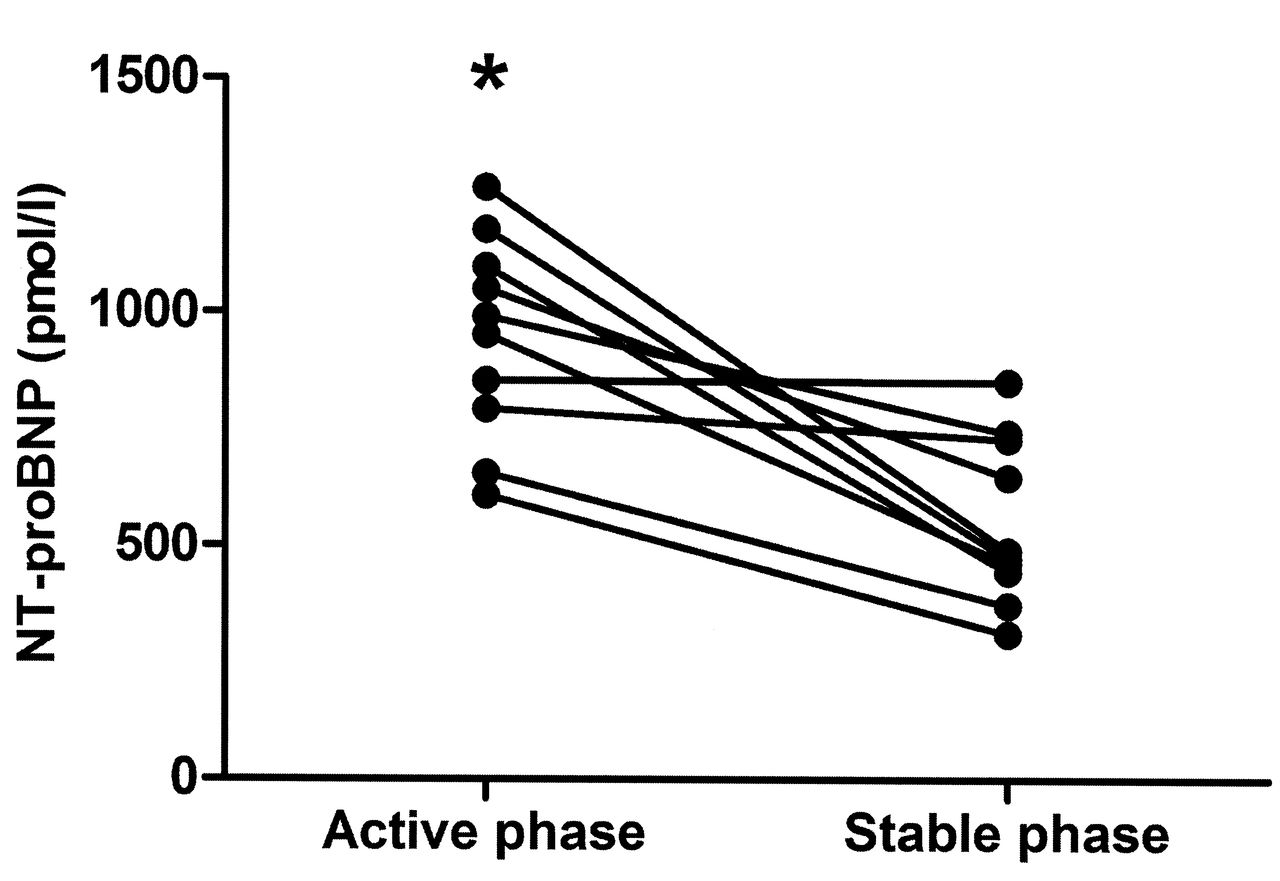
N-terminal pro-brain natriuretic peptide (NT-proBNP) concentrations in patients with Takayasu arteritis studied during both the active and stable phase (n = 10). *p = 0.001 vs stable phase.
NT-proBNP and TA classification
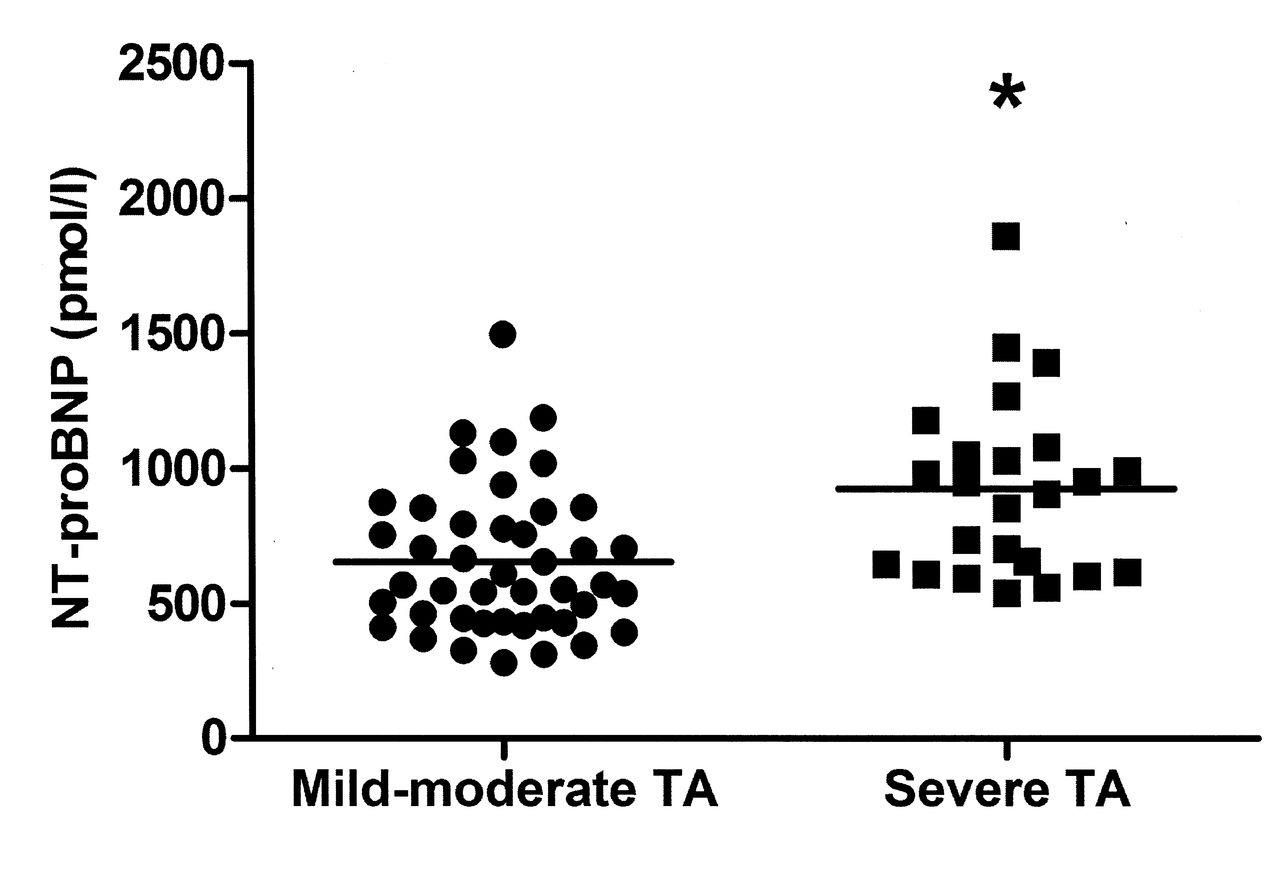
Considering the extent of arterial involvement, we found that NT-proBNP levels were higher in patients with Type III TA (846.7 ± 376.3 pmol/l) than in patients with Type I (592.9 ± 231.4 pmol/l) or Type II TA (799.6 ± 274.0 pmol/l) (p = 0.016; Figure 3). No significant differences were found in the NT-proBNP concentrations between patients with and those without pulmonary artery involvement (897.2 ± 487.6 pmol/l vs 723.6 ± 277.6 pmol/l, respectively; p = 0.299). On the basis of the complications attributed to TA, we observed that patients with severe TA exhibited significantly higher NT-proBNP levels than those with mild-moderate TA (924.0 ± 332.4 pmol/l vs 653.8 ± 269.1 pmol/l; p = 0.001; Figure 4). The CRP concentrations were increased in patients with severe disease, although the difference was not significant (6.3 ± 5.4 mg/l vs 4.3 ± 4.4 mg/l; p = 0.421).

N-terminal pro-brain natriuretic peptide (NT-proBNP) concentrations in patients with type I, type II, and type III Takayasu arteritis (TA). *p = 0.006 vs type I TA. #p = 0.038 vs type I TA.
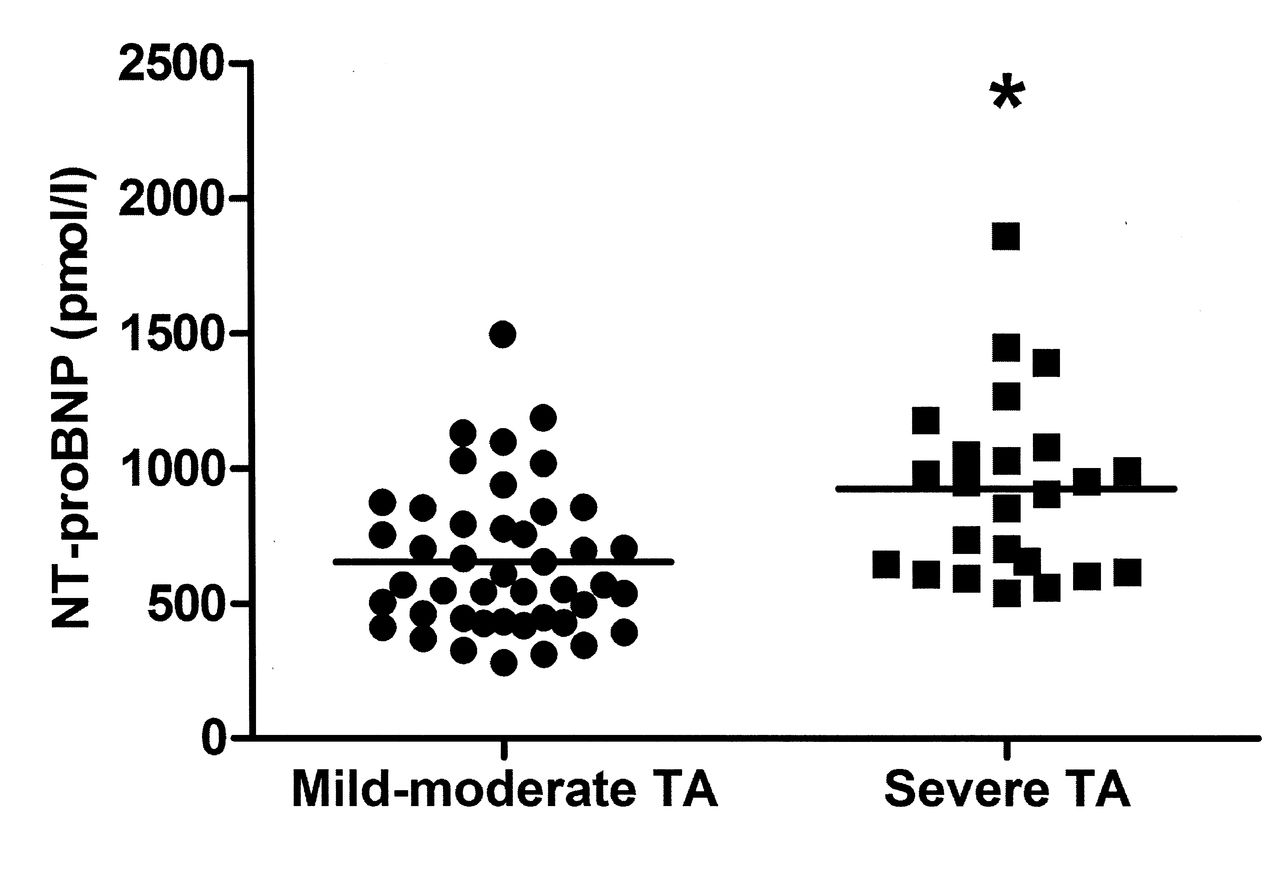
N-terminal pro-brain natriuretic peptide (NT-proBNP) concentrations in patients with mild-moderate and severe Takayasu arteritis (TA). *p = 0.001 vs mild-moderate TA.
NT-proBNP and inflammatory markers of TA
A significantly positive correlation was found between NT-proBNP and log (CRP; r = 0.392, p = 0.001), as well as log (ESR; r = 0.333, p = 0.006) and WBC count (r = 0.243, p = 0.046) in patients with TA. The results of multiple linear regression analysis showed that inflammatory markers, namely, log (CRP), log (ESR), and WBC count, were independently associated with NT-proBNP levels in patients with TA after these variables were adjusted for age, sex, BMI, and other confounding factors (Table 2).
Multiple regression analysis to evaluate associations with NT-proBNP in Takayasu arteritis.
DISCUSSION
In this study, NT-proBNP concentrations were increased in patients with active TA even without CVD compared with those in patients with inactive TA and the control subjects. Patients with TA exhibiting worse extensive arterial involvement or complications also showed significantly higher NT-proBNP levels. In addition, inflammatory markers, namely, CRP, ESR, and WBC count, were independently associated with NT-proBNP levels in TA.
Originally, NT-proBNP was considered a useful cardiac biomarker to diagnose and evaluate congestive heart failure22,23. More recently, concentrations of NT-proBNP were also used to predict mortality in the general population as well as in cohorts of patients with acute coronary syndromes and stable coronary heart disease8,9,10, suggesting that, in addition to being a marker of ventricular dysfunction, it is also a marker of cardiovascular risk. Recent evidence suggests that apart from myocardial stretch and ischemia, inflammation may also contribute to increased NT-proBNP concentrations in chronic inflammatory diseases15,24.
Our results showed that NT-proBNP concentrations in patients with TA were significantly higher than those in healthy controls. These results are consistent with those in previous studies, in which other systemic inflammatory diseases without hemodynamic stress have been observed15,16. However, this variation cannot be explained by differences in age, sex, BMI, or serum creatine. Considering RA and ankylosing spondylitis, we also observed that plasma NT-proBNP levels were independently associated with inflammatory markers, namely, CRP, ESR, and WBC count, in patients with TA15,24. The underlying mechanisms of the relationship between NT-proBNP and inflammation remain unclear. Concentrations of plasma proinflammatory cytokines, such as tumor necrosis factor-α (TNF-α), interleukin 6 (IL-6), and chemokine regulated on activation, normal T cell expressed and secreted (RANTES), are increased in patients with TA25,26. Studies have also shown that TNF-α and IL-6 can significantly increase the mRNA expression and secretion of BNP, which is independent of hemodynamic influence from cultured rat ventricular myocytes11,12. In addition, the plasma levels of RANTES are significantly correlated with BNP levels during acute allograft rejection13. Mehra, et al14 found that plasma BNP levels were associated with genes related to cardiac structural remodeling, vascular injury, inflammation, and alloimmune processes in 28 heart transplant recipients with clinical quiescence. Therefore, the presence of inflammation should be considered as a noncardiac source of an increase of NT-proBNP27.
Plasma levels of NT-proBNP were also significantly increased in patients with TA during the stable phase of disease compared with control subjects. CRP concentrations were also higher in patients with remission than in controls, but this was not statistically significant. Thus, we speculate that NT-proBNP may correlate better with arterial injury and aortic stiffness. TA is associated with increased arterial stiffness in central elastic arteries and persists when TA is clinically quiescent17. Studies show that increased plasma BNP levels are accompanied by deterioration of elastic properties in patients with coronary artery disease28 and hypertension18, as well as in healthy individuals29. Increased arterial stiffness leads to early induction of reflected pulse waves and increases ventricular afterload; as a result, the synthesis and release of BNP are stimulated18. Although only 10 patients were subjected to remeasurement of NT-proBNP levels at different disease phases in our study, the decrease in such levels suggested that active control of inflammatory status may reduce the risk of vasculitic lesions and cardiovascular complications.
Patients with TA exhibiting severe complications showed higher NT-proBNP levels. The CRP concentrations were increased in patients with severe disease, although the difference was not significant. The presence of serious complications is strongly associated with poor prognosis in patients with TA3. Therefore, our findings suggest that NT-proBNP may be an indicator of disease severity. Monitoring of circulating levels of NT-proBNP may assist early evaluation of potential complications in patients with TA.
Several limitations in this study should be noted. Considering that our study design was cross-sectional, our results may be limited. Followup data were available for only 10 patients. Hence, further longitudinal studies involving a larger number of patients than in our study should be conducted to investigate whether NT-proBNP can provide prognostic information for TA. Based on our criteria, some patients were excluded from the study, which may limit the use of NT-proBNP. However, we intended to investigate the independent relationship between NT-proBNP and inflammation in TA, and other factors affecting NT-proBNP levels should be excluded, especially at the earlier stage of the disease.
NT-proBNP levels were significantly increased in patients with active TA and in severe cases. NT-proBNP levels were also independently associated with inflammation. These results indicated that NT-proBNP may be a useful marker to assess the activity, severity, and progression of TA.
Footnotes
-
Supported by the National Natural Science Foundation of China (grant no. 81170285) and the Research Fund for the Doctoral Program of Higher Education of China (grant no. 20101106110012).
- Accepted for publication April 17, 2014.








{kind=link}
{kind=link}
{kind=link}
{kind=link}