

Abstract
Objective. Many studies have highlighted the hypolipidemic action of hydroxychloroquine (HCQ). We investigated the effect of HCQ on the lipid profile of patients with Sjögren syndrome (SS).
Methods. The present retrospective observational study included 71 female patients with SS treated with HCQ. The levels of total cholesterol (TC), high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol, triglycerides (TG), and atherogenic index (TC/HDL) were measured at baseline, after 6 months, and 1, 3, and 5 years after initiation of HCQ treatment. Analysis to investigate changes over time was performed in the entire patient group and in the separate subgroups: those receiving (21 patients) and those not receiving (50 patients) hypolipidemic treatment.
Results. For the entire group of patients a statistically significant decrease in TC was noted (levels before treatment 220 ± 41 mg/dl, and at 5 yrs 206 ± 32 mg/dl, p = 0.006). A statistically significant difference was observed in the levels of HDL (57 ± 14 mg/dl vs 67 ± 17 mg/dl, p < 0.001) and in atherogenic index (4.0 ± 1.3 vs 3.3 ± 0.9, p < 0.001). Patients not receiving a hypolipidemic agent during the same period demonstrated a decrease in TC (214 ± 40 mg/dl vs 208 ± 34 mg/dl, p = 0.049), an increase in HDL levels (55 ± 15 mg/dl vs 67 ± 18 mg/dl, p < 0.001), and a decrease in atherogenic index (4.0 ± 1.4 vs 3.3 ± 0.9, p < 0.001). In the subgroup of patients receiving hypolipidemic treatment, the respective changes in their lipid profile were not significant in the first years but became significant in the long term.
Conclusion. Use of HCQ in patients with SS was related to a statistically significant decrease in TC, an increase in HDL, and improvement in the atherogenic index.
- SJOGREN SYNDROME
- HYDROXYCHLOROQUINE
- TOTAL CHOLESTEROL
- HIGH-DENSITY LIPOPROTEIN CHOLESTEROL
- LOW-DENSITY LIPOPROTEIN CHOLESTEROL
Sjögren syndrome (SS) is an autoimmune disease that primarily affects the exocrine glands. The salivary and the lacrimal glands are mainly impaired in SS and they rapidly become functionally insufficient1,2. Apart from the glandular manifestations, SS may be also characterized by extraglandular manifestations such as musculoskeletal symptoms (arthralgias or arthritis), pulmonary disease, peripheral nerve dysfunction, Raynaud phenomenon, cutaneous vasculitis, and gastrointestinal system involvement3,4,5,6,7. The syndrome can occur as a distinct disease entity (primary SS, pSS) or in the context of an underlying autoimmune disease such as rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE; secondary SS)8.
Despite considerable recent advances in our understanding of disease pathophysiology and pathogenesis, SS treatment remains empirical9,10. Hydroxychloroquine (HCQ) remains one of the most commonly used disease-modifying antirheumatic drugs (DMARD) for the treatment of various autoimmune rheumatic diseases, including SS. HCQ is reported to demonstrate a well-defined disease-modifying effect on rheumatic diseases and simultaneously exhibits both antithrombotic and metabolic (hypolipidemic and hypoglycemic) actions11,12,13,14,15. The use of HCQ in pSS has been shown to be beneficial in several aspects of the disease, such as constitutional symptoms (fatigue), arthralgias, glandular involvement, salivary flow, and laboratory abnormalities16,17. Regarding laboratory abnormalities in SS, HCQ treatment results in a reduction in levels of acute-phase reactants and rheumatoid factor, suppression of hypergammaglobulinemia17,18, and as recently reported, reductions in salivary and serum levels of B cell activating factor16. To our knowledge, there is only 1 report in which no benefit in clinical symptoms and signs was shown in patients with SS treated with HCQ18.
The effect of HCQ on the lipid profile of patients with autoimmune rheumatic diseases has become an area of intensive research due to the evidence of excess cardiovascular risk in these patients19,20,21,22,23. In patients with active autoimmune diseases, specific patterns of dyslipidemia have been reported. For example, the characteristic pattern of the lipid profile in patients with SLE includes elevated levels of triglycerides (TG) and very low-density lipoprotein cholesterol (VLDL) and suppressed high-density lipoprotein cholesterol (HDL) levels. Of note, these changes have been related to SLE activity24,25. A decrease in HDL levels has been a consistent finding in patients with RA26,27 and has been related to accelerated atherosclerosis28. A significant decrease in total cholesterol (TC) and HDL levels has been observed in patients with pSS29,30. Dyslipidemia in SS was found to be associated with the presence of anti-Ro/SSa antibodies and anti-La/SSb antibodies in 1 study29, but opposite findings were reported by another study30. The use of antimalarials for the treatment of autoimmune diseases and particularly of SLE has been associated with a decrease in TC, VLDL, and LDL levels, and a parallel increase of HDL levels31,32. In patients with SLE, chloroquine diphosphate administered either alone or with corticosteroids improved HDL levels. Additionally, it seems that this drug has a lowering effect on TG and VLDL levels through inhibition of corticosteroid-induced hepatic synthesis of lipoproteins33.
According to several studies, apart from dyslipidemia, patients with primary SS show a higher prevalence of diabetes mellitus (DM) than healthy persons30,34. As expected, the prevalence of dyslipidemia and DM appears even higher in patients with SS who were treated with corticosteroids34. Antimalarial treatment may prevent the occurrence of these metabolic alterations (dyslipidemia and DM)34. HCQ treatment has been associated with improvement of insulin sensitivity in obese individuals who are nondiabetic, and thus with reduction in the risk for developing DM14,15,35. It is notable that both hypertriglyceridemia and DM have been associated with a higher prevalence of extraglandular manifestations in SS, especially renal, liver, and vasculitic involvement30.
Based on the available data derived from patients with SLE regarding the effect of HCQ treatment on lipids, we sought to determine the effect of HCQ on the lipid profile of nondiabetic patients with pSS.
MATERIALS AND METHODS
In the present retrospective observational study, 71 female adult (> 18 yrs) patients from a total of 806 patients with primary SS who attended the Rheumatology Department of the University Hospital of Ioannina were included. All included patients fulfilled the American European Consensus Criteria for SS36,37. The following inclusion criteria were considered:
-
Treatment with HCQ for arthralgias and/or for symptoms of dry eyes and dry mouth (sicca symptoms) on a longterm basis (at least 5 yrs). Thus, patients who discontinued HCQ owing to inefficacy, toxicity, or other reasons before completing 5 years of HCQ therapy were excluded from the study.
-
(a) No hypolipidemic treatment intake before or during HCQ treatment or (b) Intake of hypolipidemic agent only under the following circumstances:
-
Initiation of a hypolypidemic agent at least 12 months before start of HCQ therapy
-
Intake of the same lipid-lowering treatment for the entire 5-year period
-
Intake of the same lipid-lowering treatment in a stable dose for the entire 5-year period
-
-
Negative current and past history of DM.
From the 71 SS patients under HCQ therapy that were included in our study, 50 (70.4%) patients were not receiving hypolipidemic treatment during the whole 5-year period; 21 patients (29.6%) were receiving hypolypidemic treatment (statins): 18 (85.7%) of the 21 patients were receiving atorvastatin and 3 (14.3%) were receiving rovastatin.
Patients’ records were reviewed and demographic, clinical, and laboratory characteristics at baseline and at the end of the followup period were recorded. The following characteristics were collected for each patient: sex, age, glandular, and extraglandular disease manifestations and autoantibody profile. Data concerning treatment with DMARD, steroids, and hypolipidemic agents were also recorded.
Data concerning the lipid profile such as TC, HDL, LDL, TG, and atherogenic index (TC/HDL) were collected before initiation of HCQ treatment as well as after 6 months, and 1, 3, and 5 years. It is notable that in our clinic patients have lipid profiles obtained on a regular basis. Serum lipids are determined in overnight fasting blood samples. TC, TG, and HDL are determined on an Olympus AU560 Clinical Chemistry Analyser, while LDL are estimated using the Friedewalt formula38,39.
To estimate the changes in lipid profile variables over time, appropriate analysis with the Friedman test was applied for the entire patient group, as well as separately for patients who were not receiving hypolipidemic treatment (n = 50) and for patients who were receiving hypolipidemic treatment (statins; n = 21). Linear regression analysis was performed to explore the relationship between the 5-year change in each variable of the lipid profile (ΔTC levels, ΔHDL levels, ΔLDL levels, ΔTG levels) and a set of independent variables [age, steroid intake (as a categorical variable) and time-averaged C-reactive protein (CRP)] separately in these 2 subgroups. Area under the curve methods based on the trapezoid rule were applied to determine the time-averaged measures of CRP collected at all visits over the 5-year observational period. Comparisons between groups were made with chi-square test for categorical variables and Mann-Whitney U test for continuous variables. Statistical analysis was performed using SPSS Statistics, version 17.0.
RESULTS
From a total of 806 patients with primary SS who attended our Rheumatology Department, 103 patients with SS were treated with HCQ. Thirty-two of them were excluded from the present study. Ten patients discontinued HCQ treatment at 36 months because of eye toxicity. Fifteen patients were withdrawn after 27 months of HCQ treatment because of loss of efficacy, and 7 patients were lost from followup. Thus, 71 patients were included. All 71 patients were women with a mean ± SD age of 64 ± 11 years. The mean disease duration was 12.2 ± 5.8 years. These 71 patients had received HCQ for arthralgias and/or for their symptoms of dry eyes and dry mouth (sicca symptoms) for 7.2 ± 3.6 (mean ± SD) years. The clinical and laboratory features of the 71 patients as well as concomitant therapy with other DMARD or steroids at initiation of HCQ treatment are depicted in Table 1. Of note, these 71 patients did not differ from the whole cohort of 806 patients with SS in demographic characteristics, clinical manifestations, or immunological profile (data not shown). The main clinical/laboratory characteristics as well as baseline lipid levels of the 2 subgroups are also presented in Table 1. No statistically significant differences were found when these characteristics were compared between the 2 subgroups (Table 1).
Characteristics of patients with Sjögren syndrome under hydroxychloroquine (HCQ) treatment.
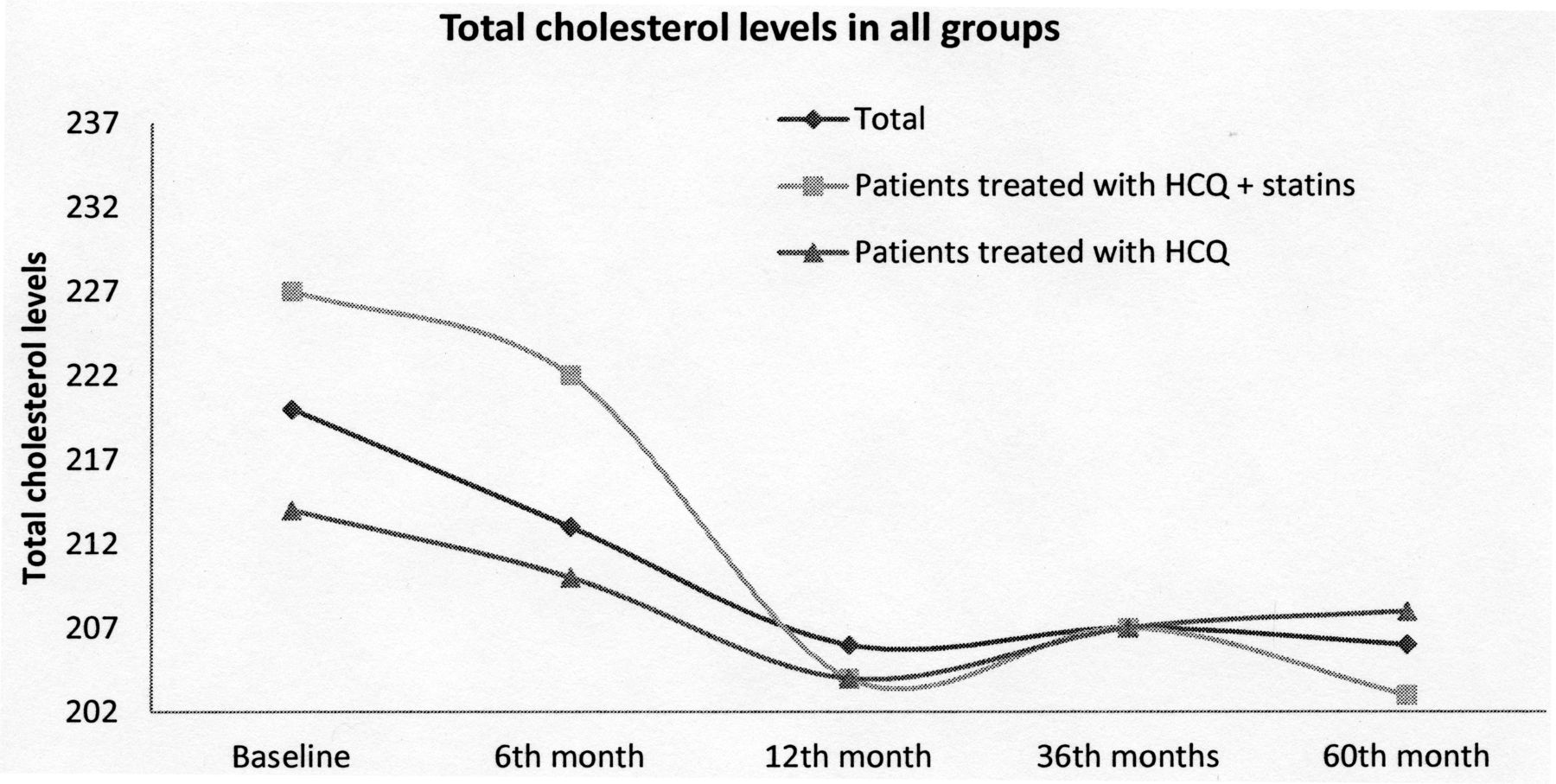
A statistically significant improvement in variables of the lipid profile was observed in the group of 71 patients during HCQ therapy; levels of TC and the atherogenic index were decreased, while HDL levels were increased (Table 2). It is notable that this improvement was already observed at 6 months of HCQ therapy. More specifically, TC levels were decreased from baseline levels of 220 ± 41 mg/dl to 213 ± 40 mg/dl at 6 months and to 206 ± 39 mg/dl at 12 months (p = 0.01). Additionally, HDL levels were increased from 57 ± 14 mg/dl to 61 ± 14 mg/dl after 12 months of HCQ treatment. The atherogenic index also showed a progressive reduction over time; it was reduced from baseline levels of 4.0 ± 1.3 to 3.8 ± 1.1 at the sixth month and further reduced to 3.5 ± 0.8 at the 12th month (p = 0.001). LDL and TG levels were also improved, although these changes did not reach statistical significance (Table 2). Improvement in variables of lipid profile in the 71 patients was sustained after 36 and 60 months of HCQ treatment (Table 2). A statistically significant decrease in TC was noted (levels before treatment 220 ± 41 mg/dl and at 5 years 206 ± 32 mg/dl, p = 0.006; Figure 1). A statistically significant difference was also observed in the levels of HDL (57 ± 14 mg/dl vs 67 ± 17mg/dl, p < 0.001; Figure 2) and in the atherogenic index (4.0 ± 1.3 vs 3.3 ± 0.9, p < 0.001) in the same period (Figure 3).
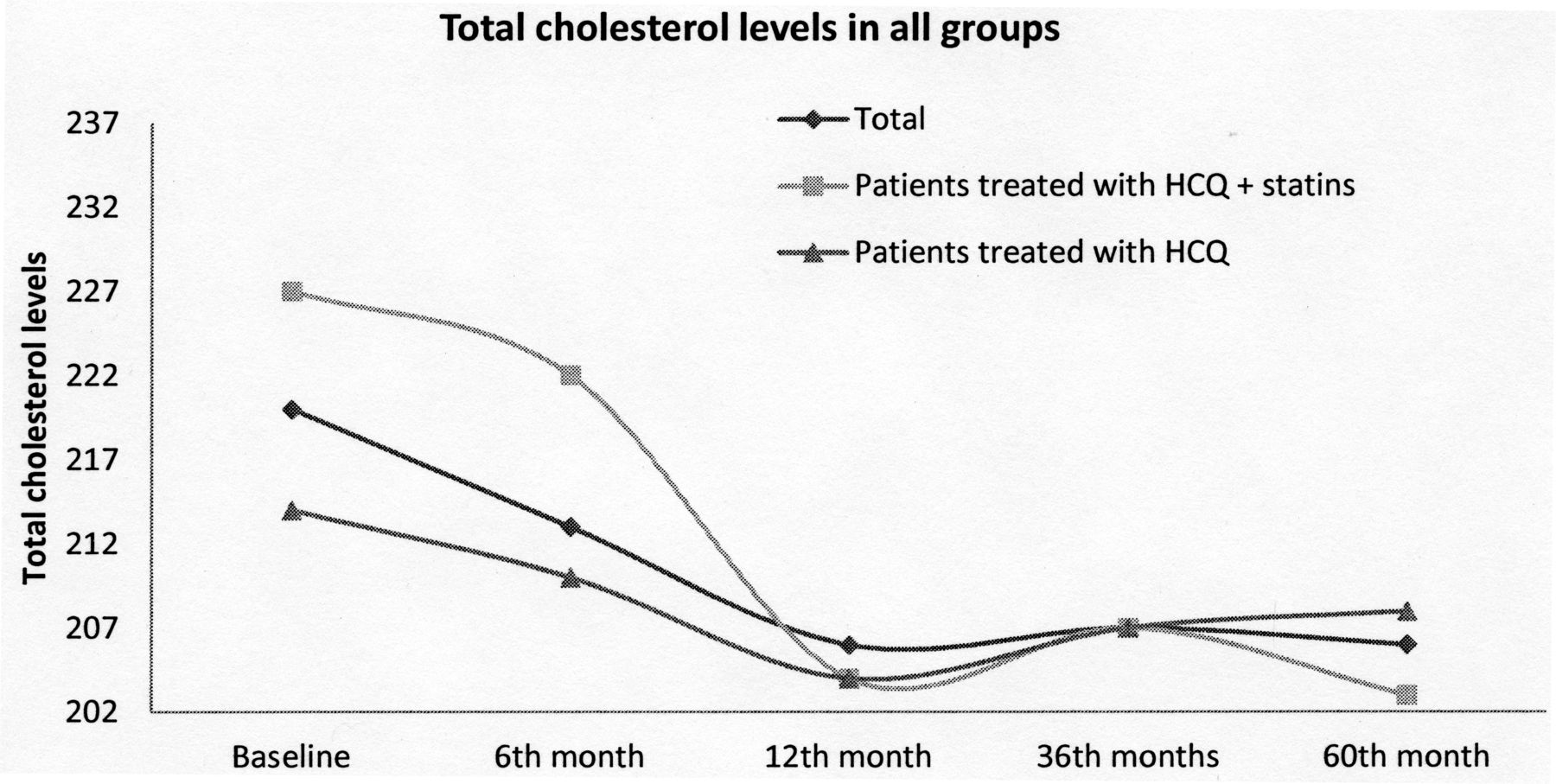
Changes over time in the levels of total cholesterol (TC) in the 3 groups of patients. In the entire group of patients and in the subgroup of patients who were not receiving hypolipidemic treatment, changes in TC levels from baseline to each time point were statistically significant (p < 0.05). In the subgroup of patients receiving hypolipidemic treatment, changes in TC levels were not statistically significant in all comparisons. Comparison of TC levels between the 2 subgroups at baseline as well as at 6, 12, 36, and 60 months did not reveal statistically significant differences. HCQ: hydroxychloroquine.

Changes over time in levels of high-density lipoprotein cholesterol (HDL) in the 3 groups of patients. In the entire group of patients and in the subgroup of patients who were not receiving hypolipidemic treatment, changes in HDL levels from baseline to each timepoint were statistically significant (p < 0.05). In the subgroup of patients receiving hypolipidemic treatment, changes over time in HDL levels were not statistically significant except for the comparison between baseline and 60 months (p < 0.05). Comparison of HDL levels between the 2 subgroups at baseline as well as at 6, 12, 36, and 60 months did not reveal statistically significant differences. HCQ: hydroxychloroquine.

Changes over time in the levels of atherogenic index in the 3 groups of patients. In the entire group of patients and in the subgroup of patients not receiving hypolipidemic treatment, changes in atherogenic index from baseline to each timepoint were statistically significant (p < 0.05). In the subgroup of patients receiving hypolipidemic treatment, changes over time in atherogenic index were not statistically significant except for the comparison between baseline and 60 months (p < 0.05). Comparison of atherogenic index between the 2 subgroups at baseline as well as at 6, 12, 36, and 60 months did not reveal statistically significant differences. HCQ: hydroxychloroquine.
Changes over time in lipid profile variables in the entire group of 71 patients under HCQ treatment.
Patients who were not receiving hypolipidemic treatment showed statistically significant changes during the same time interval (baseline to 5 yrs); a decrease in TC (214 ± 40 mg/dl vs 208 ± 34 mg/dl, p = 0.049; Figure 1), an increase in HDL levels (55 ± 15 mg/dl vs 67 ± 18 mg/dl, p < 0.001; Figure 2), and a decrease in levels of atherogenic index (4.0 ± 1.4 vs 3.3 ± 0.9, p < 0.001; Figure 3).
On the other hand, in the group of patients who were receiving concomitant hypolipidemic treatment (statins), the reduction in TC levels was not statistically significant during the entire 5-year period of observation (227 ± 39 mg/dl vs 203 ± 27 mg/dl, p = 0.109). The changes over time that were observed in the atherogenic index and in HDL levels were also not significant until the third year. However, the comparison at the timepoints 0 and 5 years revealed a statistically significant improvement in the levels of atherogenic index (4.0 ± 0.9 vs 3.2 ± 0.9, p = 0.013) and in HDL levels (58 ± 12 mg/dl to 68 ± 17 mg/dl, p = 0.011). The respective changes are schematically presented in Figures 1–3.
Eight of 50 patients (16.0%) who were not receiving hypolipidemic treatment were receiving steroids. The daily dose of steroids in these 8 patients was relatively stable during the study. At baseline the mean ± SD daily dose of prednisolone was 6.4 ± 3.1 mg/dl, at 6 months it was 6.1 ± 3.3 mg/dl, at 12 months it was reduced to 5.1 ± 2.9 mg/dl, at 36 months it was further reduced to 4.4 ± 2.7 mg/dl, and at 60 months it was 3.7 ± 3.0 mg/dl [p = not significant for all comparisons apart from the comparison between baseline and 60 months (p = 0.045)]. On the other hand, only 3 of the 21 patients (14.3%) under concomitant therapy with statins were receiving steroids. At baseline the mean ± SD daily dose of prednisolone was 5.5 ± 3.7 mg/dl. Steroid administration was discontinued in 1 patient at the 10th month while the remaining 2 patients continued steroid intake in the same dose for the entire period of followup.
The results of linear regression analysis showed that steroid intake made no significant unique contribution to prediction of 5-year change in levels of TC, HDL, LDL, or TG; neither in the subgroup of patients who were not receiving hypolipidemic treatment; nor in the subgroup of patients under concomitant therapy with statins (p = not significant for all analyses). Similar results were obtained for age and time-averaged CRP (a marker of disease activity; p was not significant for all analyses).
DISCUSSION
During the last decade research focused on the hypolipidemic effect of HCQ in RA and SLE. These patients frequently present an abnormal lipid profile, due to the augmented inflammatory burden of these diseases, which partially explains why they are at a greater cardiovascular risk. Besides, disease activity has also been shown to aggravate the pattern of dyslipidemia observed in these patients, especially in patients with SLE. In the study by Borba and Bonfá, active disease enhanced an increase in VLDL and TG levels and a decrease in HDL levels, compared to patients with inactive SLE25. Further, a significant correlation was found between SLE disease activity index scores and all lipid fractions25. In a recent study by Cruz, et al, it was suggested that patients with pSS may quite often present an abnormal lipid profile, which is associated with elevated levels of acute-phase reactants such as erythrocyte sedimentation rate40.
Of note, the exact mechanism by which antimalarials display their hypolipidemic action remains elusive and needs further investigation. It has been suggested that chloroquine, an agent structurally similar to HCQ, is an inhibitor of cholesterol biosynthesis in rat hepatocytes41. In human fibroblasts and mouse adrenal cell cultures, chloroquine has multiple effects on cholesterol metabolism. Chloroquine inhibits lysosomal hydrolysis of cholesteryl esters through an increase in the pH within lysosomes and inactivates acid proteases. Additionally, chloroquine stimulates the activity of hydroxymethylglutaryl CoA (HMG-CoA) reductase and retards its degradation41. Apart from the above mechanisms, another Toll-like receptor (TLR)-independent mechanism by which antimalarial agents may exhibit their hypolipidemic action includes upregulation of the LDL receptor gene transcription, stimulation of LDL receptors’ capacity, and enhancement of LDL removal from plasma by LDL receptors42,43. The hypolipidemic action of antimalarials may also be attributable to TLR antagonism, a well-established effect of these agents. It has been shown by in vitro studies that a TLR 9-mediated increase in expression of perilipin 3, a member of the PAT family of proteins implicated in excessive accumulation of lipids in macrophages, may sequentially lead to formation of foam cells, which is a hallmark of atherosclerosis44. Thus the antagonistic effect of HCQ on TLR may halt atherosclerosis through significant involvements in lipid metabolism42,43. Several authors have also suggested that the hypolipidemic effect of HCQ is potentially attributable to systemic inflammation control. Nevertheless, the antiinflammatory effect of HCQ is relatively weak19.
In 1990 Wallace, et al, described a statistical significant association between HCQ treatment in patients with RA or SLE and low serum levels of TC, LDL, and TG, which was unaffected by steroid intake or changes in diet or weight45. In the study by Morris, et al, HCQ treatment of 709 patients with RA was associated with a significant reduction in TC levels and atherogenic index, and with an increase in HDL levels19. In the longitudinal study of Cairoli, et al, an improvement in the lipid profile of 24 patients with SLE was shown 3 months after initiation of HCQ treatment. There was a statistically significant decrease in both TC and LDL levels (p = 0.023 and p = 0.023, respectively)20. This effect was maintained after 12 months of treatment with antimalarials. In the study by Chong, et al, which included 100 patients with lupus nephritis, it was demonstrated that HCQ treatment was associated with lower TC, LDL, and HDL levels46.
In our study, patients treated with statins and HCQ did not reach statistically significant differences in the variables of their lipid profile during the first 3 years. However, in the long term (5 yrs), several variables of lipid profile were significantly improved. The lack of significant effects of HCQ on several outcomes in the statin-treated group could be due to the relatively small number of patients in this group, because the magnitude of the reduction in TC levels was actually higher than in the group of patients not receiving hypolipidemic treatment. Thus, the number of subjects in this group of patients with SS was too small to draw conclusions from the results. On the other hand, a drug interaction cannot be excluded. It is known that statins are competitive inhibitors of HMG-CoA reductase, the rate-limiting step in cholesterol biosynthesis. Most statins have modest HDL-raising properties. TG concentrations fall by an average of 20–40% depending upon the statin and dose used47. All the SS patients in the study had already been treated with statins before initiation of HCQ treatment. The interaction of the 2 drugs concerning their effect on lipid metabolism remains unknown.
To our knowledge, the present study is the first to investigate the hypolipidemic effect of HCQ in patients with pSS. It is limited because it is a retrospective study. The effect of “good health” measures possibly adopted by several patients with adverse cardiovascular risk factors after enrollment to promote better lipid profiles (such as weight loss, exercise, low cholesterol diet) could not be measured. Further, baseline TC levels in the whole cohort were relatively low (owing to either a lack of hypercholesterolemia or to treatment with statins). Thus, the actual effect of HCQ monotherapy in patients with high TC levels could not be addressed. Despite the limitations, the results of our study clearly demonstrate that HCQ treatment in patients with SS leads to a significant decrease in TC levels and atherogenic index and a significant increase in HDL levels. Additionally, the effect of HCQ on lipid profile was found to be unaffected by steroid intake, age, or disease activity (expressed by time-averaged CRP). Further, the main advantages of the current study are the long period (5 years) of HCQ treatment and the sustained effect of HCQ on patient lipid profiles.
The findings of the current study suggest a potential benefit of HCQ in attenuating the risk of dyslipidemia in patients with SS. These results are attractive, considering the acceptable safety profile and disease-modifying effect of HCQ. Therefore, patients with SS and coexisting dyslipidemia may benefit from HCQ treatment.
- Accepted for publication January 11, 2014.








{kind=link}
{kind=link}
{kind=link}