
Abstract
Objective. To assess the usefulness of the MAdrid Sonographic Enthesitis Index (MASEI) in classifying patients as having psoriatic arthritis (PsA) and comparing entheseal abnormalities between patients with PsA, psoriasis alone (PsC), and healthy controls (HC).
Methods. Patients with PsC were assessed to exclude inflammatory arthritis. The MASEI scoring system was used to quantify the extent of ultrasonographic (US) entheseal abnormalities. The total MASEI score was categorized into items that reflected inflammatory abnormalities (MASEI-inflammatory) and chronic damage (MASEI-damage). Nonparametric tests were used to compare MASEI scores across the groups. A cutoff point of MASEI ≥ 20 was used to calculate the sensitivity and specificity of the MASEI to classify patients as having PsA.
Results. Patients with PsA (n = 50), PsC (n = 66), and HC (n = 60) were assessed. Total MASEI scores were higher in patients with PsA than in those with PsC, and both those groups were higher than HC (p < 0.0001). MASEI-inflammatory showed a similar trend (p < 0.0001). MASEI-damage was higher in patients with PsA compared to both patients with PsC and HC (p < 0.0001); however, no difference was observed between patients with PsC and HC. No significant difference in MASEI scores was found across the 3 groups in patients with a body mass index > 30. The sensitivity of the MASEI score to correctly classify patients as having PsA was 30% and the specificity was 95% when compared to HC and 89% when compared to PsC.
Conclusion. The severity of US entheseal abnormalities is highest in patients with PsA followed by PsC and is lowest in healthy controls. MASEI can specifically classify patients as having PsA.
- ULTRASOUND
- ENTHESITIS
- SPONDYLOARTHRITIS
- PSORIASIS
Enthesitis is considered the primary lesion in spondyloarthritis (SpA), including psoriatic arthritis (PsA)1. The clinical diagnosis of enthesitis is neither specific nor sensitive and often relies on typical abnormalities found in ultrasound (US) or MRI studies2. The Outcome Measures in Rheumatology (OMERACT) 7 consensus definition for US enthesopathy includes abnormalities that reflect both active inflammation and structural damage3. Hypoechogenicity and thickening of the tendon/ligament resulting from edema and increased power Doppler signal at the enthesis that represents hypervascularization are considered active inflammatory findings, while bone erosions, calcifications, and enthesophytes reflect irreversible damage that occasionally coexists with active inflammation4,5.
Because of the limitations of clinical assessment of the entheses, there is increasing interest in using US to improve the diagnosis of enthesitis and thus facilitate early diagnosis of SpA. In PsA, a potential window of opportunity allows early diagnosis by identifying patients with psoriasis and subclinical inflammatory features that may subsequently evolve to clinical arthritis. Several semiquantitative scoring systems have been developed to quantify the extent of a patient’s enthesitis. The MAdrid Sonographic Enthesitis Index (MASEI) scores greyscale abnormalities and power Doppler signal in 6 entheseal sites, mostly in the lower limbs6. De Miguel, et al reported that at a cutoff point of 20 or more, MASEI correctly classified patients as having SpA with a sensitivity of 53% and a specificity of 83.3% among a group of patients with mixed probability of having SpA7. The development and validation of MASEI was conducted on patients with SpA, but the performance of the method among patients with PsA has not been extensively assessed. Complicating matters, entheseal lesions are commonly found in patients with psoriasis who do not have clinical signs of enthesitis or synovitis8,9,10. The significance of such abnormalities is unclear because other factors, such as age and obesity, may contribute to the development of these changes. A small study suggested that subclinical enthesitis among patients with psoriasis may predict the development of PsA11.
In this cross-sectional study we aimed to assess the utility of the MASEI scoring system in correctly classifying patients with PsA among patients with psoriatic disease [patients with PsA and psoriasis alone (PsC)] and healthy controls (HC) and to compare the extent of US entheseal abnormalities across the groups and in subgroups stratified by age and body mass index (BMI).
MATERIALS AND METHODS
Patients and setting
A total of 50 patients with PsA, 66 patients with PsC, and 60 HC were included in this cross-sectional study. The study was conducted in Toronto, Canada, from June 2011 to October 2012 and enrolled consecutive patients with PsA and PsC from 2 large prospective cohorts that have been previously described12,13. Adult patients with PsA who satisfied the Classification of Psoriatic Arthritis (CASPAR) criteria14 were recruited from the University of Toronto Psoriatic Arthritis cohort. The patients are followed according to a standard protocol every 6–12 months12. Patients with PsC were recruited from the University of Toronto Psoriasis Cohort13. All of the participants with PsC had a diagnosis of psoriasis confirmed by a dermatologist and have been assessed by a rheumatologist to exclude a diagnosis of PsA. This cohort was established with the aim of studying risk factors for the development of PsA. Patients are recruited mainly from dermatology clinics and phototherapy centers. All participants are followed according to the same protocol as in the PsA cohort and are assessed annually for symptoms or signs of arthritis. HC without a history of psoriasis or inflammatory arthritis were recruited from hospital personnel and underwent a clinical assessment to exclude inflammatory arthritis. The collected information included demographic information, comorbid conditions, medications, height, weight, and disease-related information including age at diagnosis of psoriasis and PsA; counts of tender, swollen, and damaged joints; and current psoriasis activity, determined by using the Psoriasis Area and Severity Index. The study was approved by the University Health Network Research Ethics Board and all participants gave informed consent.
US assessment
US scanning of the entheses was performed by 2 rheumatologists trained in musculoskeletal ultrasound (LE, AH) using a MyLab 70XVG scanner (Esaote) equipped with a 6–18 MHz linear transducer (Esaote). The following enthesis sites that are included in the MASEI scoring system were scanned bilaterally: patella (at insertions of the quadriceps femoris and patellar tendons), Achilles tendon and plantar fascia insertions on the calcaneus, and triceps tendon insertion to the olecranon process. Each tendon was scanned in both longitudinal and transverse planes, and the scan images were stored. Each examination took about 20 min. The patients were placed in a supine position to assess the patellar and quadriceps entheses. The knee was placed in 70° flexion to assess greyscale abnormalities and in full extension to assess vascularization. Then the patients were placed in a prone position with the feet over the end of the examination table for assessment of the Achilles tendon and plantar fascia entheses. The triceps tendon enthesis was assessed with the elbow flexed to 90°.
All of the following greyscale US findings indicative of enthesopathy according to MASEI were documented (Figure 1): thickening and structural changes of the tendon insertion, calcific deposits at the tendon insertion, bony changes including erosions and enthesophyte formation as defined6. To simplify matters, ossifications and enthesophytes at the enthesis were also termed calcifications. Bursitis was defined as a well-circumscribed, localized anechoic or hypoechoic area at the site of an anatomical bursa, which was compressible by the transducer. The thickness of the enthesis was measured at the insertion of the deeper tendon margin into the bone in a longitudinal axis. Vascularization was assessed at the cortical bone insertion because this site is more specific for enthesitis compared to the presence of a signal at other sites, such as the bursa and the tendon15. Power Doppler settings were standardized with a Doppler frequency of 8–12.5 MHz, pulse repetition frequency of 750 Hz, and a wall filter of 2. A pulse repetition frequency of 500 Hz was used in the first 10 participants (2 with psoriasis, 4 with PsA, and 4 HC). Gain was adjusted until the background signal was removed. Reading of the US scans was performed independently from the scanning by a single reader (LE). Because psoriatic plaque frequently affected the scanned sites, it was difficult to blind the sonographer to the presence of psoriasis. Therefore, the US scans were recorded in digital media and read at a separate location and later date after blinding for personal data.
{kind=link}
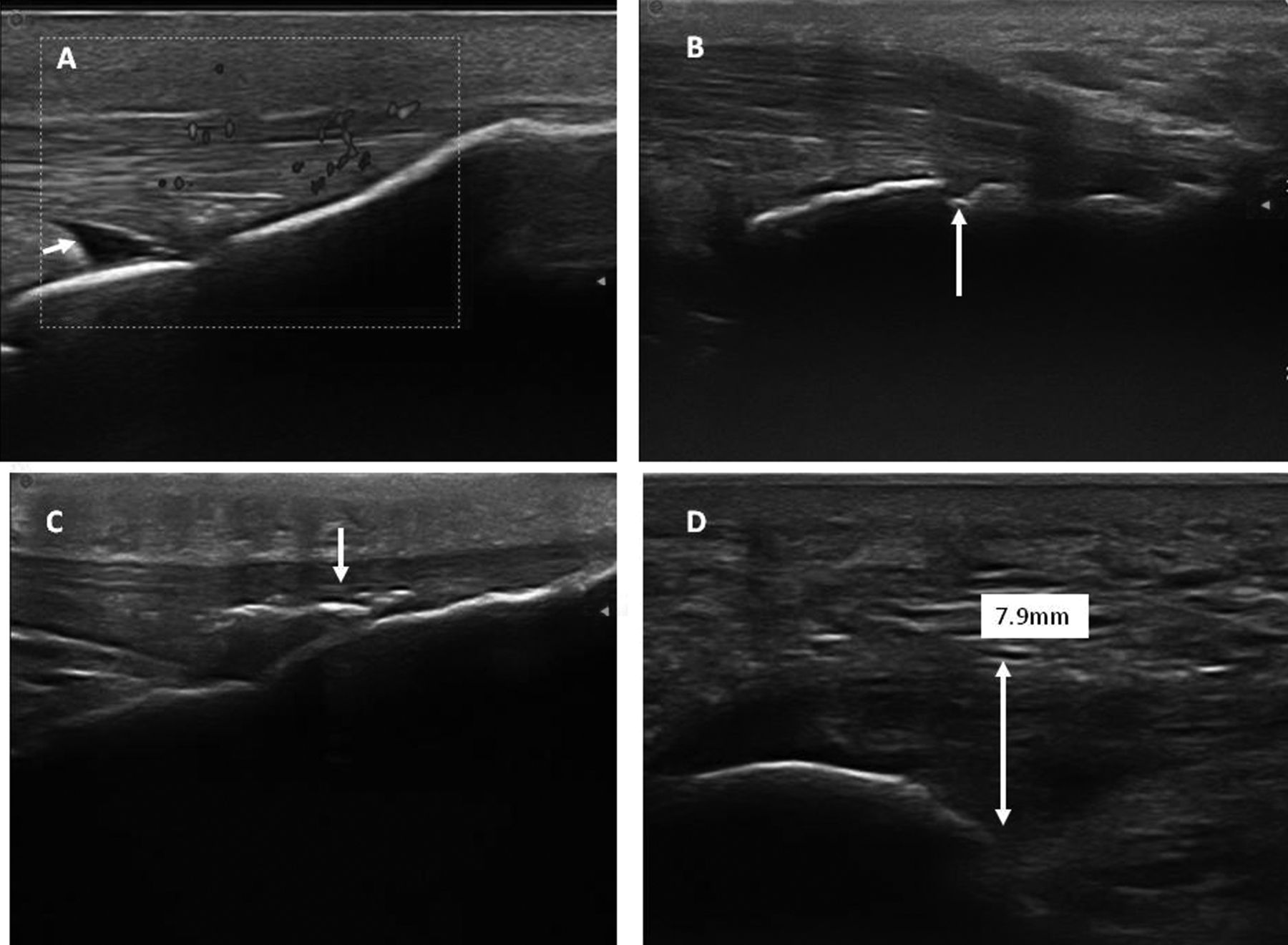
Ultrasonographic appearance of entheseal abnormalities. A. Power Doppler signal at the insertion site of the patellar tendon to the tibial tuberosity and infrapatellar bursitis (arrow). B. Posterior calcaneal erosion (arrow), Achilles tendon insertion. C. Calcification, patellar tendon insertion to tibial tuberosity (arrow). D. Thickening and structural tendon abnormalities at the plantar fascia insertion to the calcaneous.
The MASEI was used to generate a global score that reflected the severity and extent of entheseal abnormalities from all scanned sites on both sides in each subject. The total MASEI score was further categorized into the following: inflammatory changes including entheseal thickening; structural changes; bursitis and vascularization (MASEI-inflammatory); and chronic damage, including calcifications, enthesophytes, and erosions (MASEI-damage).
Intraobserver variation was checked by rereading 15 images of the study subjects (5 images from each group) on different days. The intraobserver intraclass correlation coefficient for MASEI was 0.8. Because a single assessor (LE) scanned and scored the images of 97% of the patients, interobserver variation was not assessed.
Statistical analysis
Continuous data were described by median (range) or mean (SD) according to the distribution, and categorical variables were expressed as frequencies and percentages. Comparisons between the 2 categories were made using 2-tailed t tests for normally distributed data or the Mann-Whitney U test for non-normally distributed variables. The chi-square test was used to compare categorical variables. The Kruskal-Wallis test was used to compare MASEI scores across the 2 groups. A cutoff point of MASEI ≥ 20, as suggested by de Miguel, et al7, was used to calculate the sensitivity, specificity, and positive likelihood ratios to classify patients as having PsA. To determine the effect of age and BMI on MASEI score, the study population was classified into subcategories according to age (< 40 yrs, 40–50 yrs, and > 50 yrs) and BMI (< 25, 25–30, and > 30). A multivariate ordinal logistic regression model was fit with MASEI as the ordinal outcome and with disease status as a covariate adjusting for age, sex, and BMI. MASEI was categorized into the 4 following groups based on quartiles: < 3, 3–6, 7–13, and > 13. The effect of each factor was measured through OR that were estimated along with their respective 95% CI and reported with p values. The statistical computation was performed using SAS 9.2.
RESULTS
The characteristics of the study populations are presented in Table 1.
Characteristics of the study population.
Differences in enthesitis scores across the groups
Total MASEI scores were higher in patients with PsA than PsC, with both being higher than in HC (MASEI, 13 vs 6 vs 3.5, respectively, p < 0.0001, Table 2). A similar trend was found in the inflammatory scores of MASEI with the highest score found in patients with PsA followed by patients with PsC and the lowest score in HC (MASEI-inflammatory, 6 vs 2 vs 1, p < 0.0001). MASEI-damage was higher in PsA patients compared to both patients with PsC and HC (8.5 vs 4 vs 3, respectively, p < 0.0001). However, no statistically significant difference was observed between patients with PsC and HC. The frequency of individuals who had at least 1 entheseal site with inflammatory findings (MASEI-inflammatory ≥ 1) was high in all 3 groups; however, the highest frequency was found in patients with PsA (90%) followed by patients with PsC (72%), and was lowest in the HC (48.3%, p < 0.0001). The presence of power Doppler signal in at least 1 entheseal site was also more frequent in patients with PsA compared to PsC and HC (40% vs 18.8% vs 8.3%, respectively, p < 0.0001); however, no statistically significant difference was observed between patients with PsC and HC (p = 0.1).
Enthesopathic abnormalities by group.
The frequency of each of the individual US abnormalities comprising the MASEI, except calcification (p = 0.15) and bursitis (p = 0.31), was higher in patients with PsA compared to PsC and HC, including structure (p < 0.0001), thickness (p < 0.0001), erosions (p < 0.0001), and power Doppler (p = 0.04). The sites that most frequently showed inflammatory abnormalities (MASEI-inflammatory ≥ 1) were the tibial tuberosity insertion (70% of patients with PsA, 63% of patients with PsC), plantar aponeurosis insertion (48% of patients with PsA, 23% of patients with PsC), and Achilles tendon insertion (44% of patients with PsA, 24% of patients with PsC).
Sensitivity and specificity of MASEI
The sensitivity of a MASEI score ≥ 20 to correctly classify patients as having PsA was 30% among patients with psoriatic disease and remained 30% when compared to HC. However, the specificity was 95%, relatively high, when compared to HC and 89% when compared to patients with psoriatic disease (PsA and PsC). The positive likelihood ratio (LR) was 5.8 and 2.63 when compared to HC and patients with PsC, respectively.
The correlation between age and MASEI
Enthesopathic changes correlated moderately with age (r = 0.33, p < 0.001). Similar to the trend observed in the entire study population, the total MASEI scores were higher in patients with PsA, followed by patients with PsC, with both being higher than HC in subjects below the age of 40 years (9 vs 3 vs 2, respectively, p = 0.005, Table 3) and in those between 40 to 50 years of age (12.5 vs 6 vs 4, respectively, p = 0.02). Among participants who were older than 50 years, significantly higher scores were observed in patients with PsA compared to patients with PsC and HC (16 vs 7 vs 8, respectively, p = 0.0008). However, no difference was observed between patients with PsC and HC. MASEI-inflammatory showed a similar trend, but MASEI-damage showed a difference across the groups only in patients who were older than 50 years.
MAdrid Sonographic Enthesitis Index (MASEI) score by age group.
The correlation between BMI and MASEI
A moderately positive correlation was found between BMI and MASEI score (r = 0.47, r < 0.001). The total MASEI scores were higher in patients with PsA than those with PsC, with both being higher than HC in subjects with BMI < 25 (7 vs 4 vs 2, respectively, p = 0.02, Table 4) and in those with BMI of 25 to 30 (13 vs 5 vs 5, respectively, p = 0.006). However, no significant difference in MASEI scores was observed across the groups in people with a BMI > 30 (18 vs 9.5 vs 12, respectively, p = 0.18). Similarly, no significant differences in MASEI-inflammation or MASEI-damage were observed across the groups with BMI > 30.
MAdrid Sonographic Enthesitis Index (MASEI) score by body mass index (BMI) group.
Multivariate analysis
The PsA group was associated with a higher MASEI category compared to patients with PsC after adjusting for age, sex, and BMI (PsA vs PsC, OR 3.36, p = 0.0002, 95% CI 1.6, 7.1). However, no significant difference in MASEI score was observed between patients with PsC and HC in the multivariate analysis (p = 0.59). Male sex (p = 0.02), older age (p < 0.0001), and higher BMI (p < 0.0001) were also associated with a higher MASEI category in the multivariate analysis (Table 5).
The association between MAdrid Sonographic Enthesitis Index (MASEI) and disease status by logistic regression model.
DISCUSSION
Limitations in clinical assessment of the entheses have prompted the use of US to detect the presence of enthesitis. Subclinical enthesitis is common in patients with psoriasis who do not have clinically detectable inflammatory arthritis. The use of US as a tool to detect subclinical enthesitis and possibly to predict the development of PsA in patients with psoriasis is attractive, because it may facilitate early diagnosis and potentially even the prevention of PsA if appropriate treatment is instituted. However, US entheseal abnormalities do not necessarily equal enthesitis, and it is still unclear which abnormalities best differentiate between the different types of enthesopathy16. It has been suggested that hypervascularization at an enthesis is a specific sign for enthesitis as opposed to other forms of enthesopathy; however, it is still unclear whether its presence predicts the development of clinical enthesitis or arthritis15,17.
In our study we aimed to explore the usefulness of the MASEI score in differentiating patients with PsA from those with PsC and from HC. We selected the MASEI score because it is the most commonly used validated scoring system that also includes power Doppler assessment. Further, we attempted to investigate differences at the patient level by combining measurements at a group of entheses rather than at the individual enthesis level, because the former are more relevant for clinical use. The study found that the total MASEI score and the inflammatory component of MASEI showed a trend with the highest score found in patients with PsA, followed by patients with PsC, and the lowest scores were found in HC. The MASEI-damage score was also highest in PsA. However, no difference was found between PsC and HC, probably reflecting the high frequency of enthesophytes and calcifications in HC pointing to the low specificity of these abnormalities.
In accordance with a previous publication, aging and obesity significantly correlated with MASEI scores10. This finding can have significant implications as to the utility of this scoring system among older and obese individuals. A significant proportion of the HC who were older than 50 years showed entheseal abnormalities. In fact, their MASEI score was similar to that in patients with PsC. This finding may be explained by the high prevalence of entheseal abnormalities that are secondary to degenerative/mechanical factors rather than inflammation in that age group. MASEI is also less specific in obese individuals (BMI > 30) because no statistically significant difference was observed in both inflammatory and damage scores, as well as in the total MASEI score, across the 3 groups. In accordance with our findings, Gisondi, et al reported that enthesitis score, as measured by the Glasgow Ultrasound Enthesitis Scoring System (GUESS), correlates with BMI among patients with psoriasis alone10. The underlying causes of this correlation may be due to increased mechanical stress on the entheses of the lower limbs due to heavier weight, although obesity is also associated with systemic inflammation and high levels of proinflammatory cytokines18. Therefore, we cannot rule out the possibility that inflammation is a mediator mechanism for the increased entheseal abnormalities in obese individuals. The high prevalence of obesity in patients with psoriasis may complicate the assessment of enthesitis and limit the use of MASEI in obese patients with psoriatic diseases19.
Early diagnosis of PsA among patients with psoriasis can improve clinical outcome20. A significant proportion of patients with PsC have noninflammatory musculoskeletal symptoms that can mimic inflammatory arthritis and enthesitis, while others may exhibit subclinical inflammatory enthesitis without having any symptoms8,21. The application of the CASPAR criteria requires fulfillment of 1 of the 3 stem definitions: inflammatory arthritis, enthesitis, or spondylitis14. The diagnosis of enthesitis on the basis of findings on physical examination lacks sensitivity and specificity. Thus, the use of imaging of the entheses may improve the ability to diagnose PsA among patients with psoriasis. We have found that a total MASEI score showed high specificity at a cutoff point of 20 or more among patients with psoriatic disease and healthy individuals. These findings support its use as a specific tool in addition to clinical and laboratory findings for the classification of PsA. It should be noted, however, that currently there is no accepted scoring system for enthesitis. Further, the distinction between inflammatory and structural US entheseal abnormalities was based on indirect evidence, such as response to therapy, as no correlation with histological data is available4. In addition, our study enrolled patients with longstanding PsA, whereas it has been suggested that the prevalence of subclinical enthesitis may not be high among patients with early PsA22. The clinical importance of subclinical enthesitis in patients with PsC and the ability of US assessment of the entheses to improve the early diagnosis of PsA requires further study.
The MASEI score can differentiate patients with PsA from those with PsC and HC. We have confirmed previous studies that reported high frequencies of entheseal abnormalities in patients with PsC compared to HC. Age and BMI correlate significantly with entheseal abnormalities and may limit the use of the MASEI score in older and obese individuals. Longitudinal studies are required to assess the ability of subclinical entheseal abnormalities to predict the development of inflammatory arthritis in patients with psoriasis.
Footnotes
-
Funded by a grant from Abbvie Canada. Jai Jayakar was supported by a Canadian Rheumatology Association-Roche Summer Research Studentship Award. The Psoriatic Arthritis Program is funded in part by The Arthritis Society, Canadian Institutes of Health Research and the Krembil Foundation.
- Accepted for publication October 25, 2013.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.