

Abstract
Objective. The incidence of type 2 diabetes (T2D) in adults with rheumatoid arthritis (RA) was investigated, and the results were compared with non-RA controls to confirm whether RA is a risk factor for diabetes mellitus (DM) in Taiwan.
Methods. We used a databank of 1 million individuals randomly selected from 23 million Taiwanese citizens covered by the National Health Insurance plan in 2005. All persons older than age 20 years in 1998 and not diagnosed with either RA or T2D before 1998 were included. They were divided into 2 cohorts, 1 with RA and the other without. Those who had T2D before RA were excluded. Each patient in the RA cohort was followed from the RA diagnosis until the end of 2009, or until dropping out of the insurance coverage. RA was ascertained by at least 3 visits using ICD-9 code 714.0, plus at least 2 visits with prescription of antirheumatic drugs in a period of 12 months. T2D was ascertained by at least 3 visits with diabetes codes within 1 year, while hypertension (HTN) and disorders of lipid metabolism (DLM) were determined by at least 3 visits using corresponding ICD codes during the study period. Kaplan-Meier plots, log-rank tests, and Cox regression were used to study the effects of age, sex, glucocorticoid use, HTN, DLM, and RA on T2D risk.
Results. The subjects include 600,695 adults. Of these, 4193 were diagnosed with RA, and among them 799 were diagnosed with T2D. The RA to non-RA risk ratio for T2D was 1.68 (95% CI 1.53–1.84) in men and 1.46 (95% CI 1.39–1.54) in women.
Conclusion. RA appears to be associated with an increased risk for T2D in Taiwan.
Rheumatoid arthritis (RA) is a chronic inflammatory disease that mainly affects joints with synovium1. It predisposes patients to insulin resistance and may place patients at a higher risk for diabetes mellitus (DM)2. Because DM is a major risk factor for cardiovascular disease (CVD), which is the leading cause of mortality in RA3, a better assessment of DM risk in patients with RA may lead to earlier and aggressive intervention to prevent its occurrence, subsequently decreasing mortality for patients with RA.
Inflammation in RA is characterized by increased levels of mediators and cytokines4,5,6,7, e.g., tumor necrosis factor-α and interleukin 6 (IL-6), which cause dyslipidemia and accelerate atherosclerosis, resulting in hypertension (HTN). In addition, these cytokines appear to block the function of insulin at the receptor level, which may induce insulin resistance. Mortality from CVD in patients with RA may result from insulin resistance, DM, dyslipidemia, atherosclerosis, or HTN.
Several studies have focused on the risk of DM in RA. Using health insurance data, 1 study calculated a 1.4 prevalence ratio for diabetes in an RA cohort composed of 28,208 patients compared with the non-RA cohort8. In another study, a calculated HR of 1.5 was obtained using linked healthcare use data9. However, other studies showed no significant association between RA and T2D10,11,12.
Taiwan started its compulsory National Health Insurance (NHI) system in 1995. More than 95% of the hospitals and clinics in Taiwan implement the NHI, and more than 98% of the people are covered by this system13. The NHI databank is considered reliable14.
We used this databank to examine the risk of T2D for patients with RA in Taiwan. In addition, we studied the effects of age, sex, use of glucocorticoids (GC), HTN, disorders of lipid metabolism (DLM), and RA on T2D risk.
MATERIALS AND METHODS
The databank we used contains medical information from 1 million residents in Taiwan, randomly selected by the National Health Research Institute. We removed those who were younger than age 20 years or who had a diagnosis of either T2D or RA by 1998. RA was ascertained by International Classification of Diseases, 9th edition, code 714.0 in at least 3 visits plus at least 2 visits with prescription of antirheumatic drugs in any 12-month period. Medication period must last more than 6 months. This diagnosis plus medication criterion was adopted from a previous report15. T2D was ascertained by admission with a T2D code or at least 3 visits with T2D code within 1 year. The criteria were suggested by Lin, et al16.
HTN and DLM were identified by admission with HTN and DLM codes (4010, 4011, 4019 for HTN and 2720–2729 for DLM) or at least 3 visits with these codes during the study period. We excluded those who had the diagnosis of T2D prior to the diagnosis of RA.
We then assembled 600,336 subjects (300,135 men and 300,201 women) from the databank. Among them, 3839 had RA (1130 men and 2709 women), and the rest were defined as non-RA. We calculated the age-standardized and age-specific incidence of T2D in RA and non-RA cohorts. Patients with RA were followed up from the diagnosis, and the non-RA from January 1, 1998, until the diagnosis of T2D or the censor events (i.e., dropout from the NHI or the end of 2009).
We defined age as the age in 1998, and a GC user as a person who had at least 3 visits with prescription of GC within 12 months. For the RA cohort, we used the Kaplan-Meier method to estimate the event-free probability of T2D after an RA diagnosis. The log-rank test was used to compare among groups of different ages or sexes. Cox regression was applied to study the effects of RA, HTN, and DLM on T2D risk. The HR for T2D were obtained with the Cox model.
RESULTS
Patients with RA had a higher risk for T2D
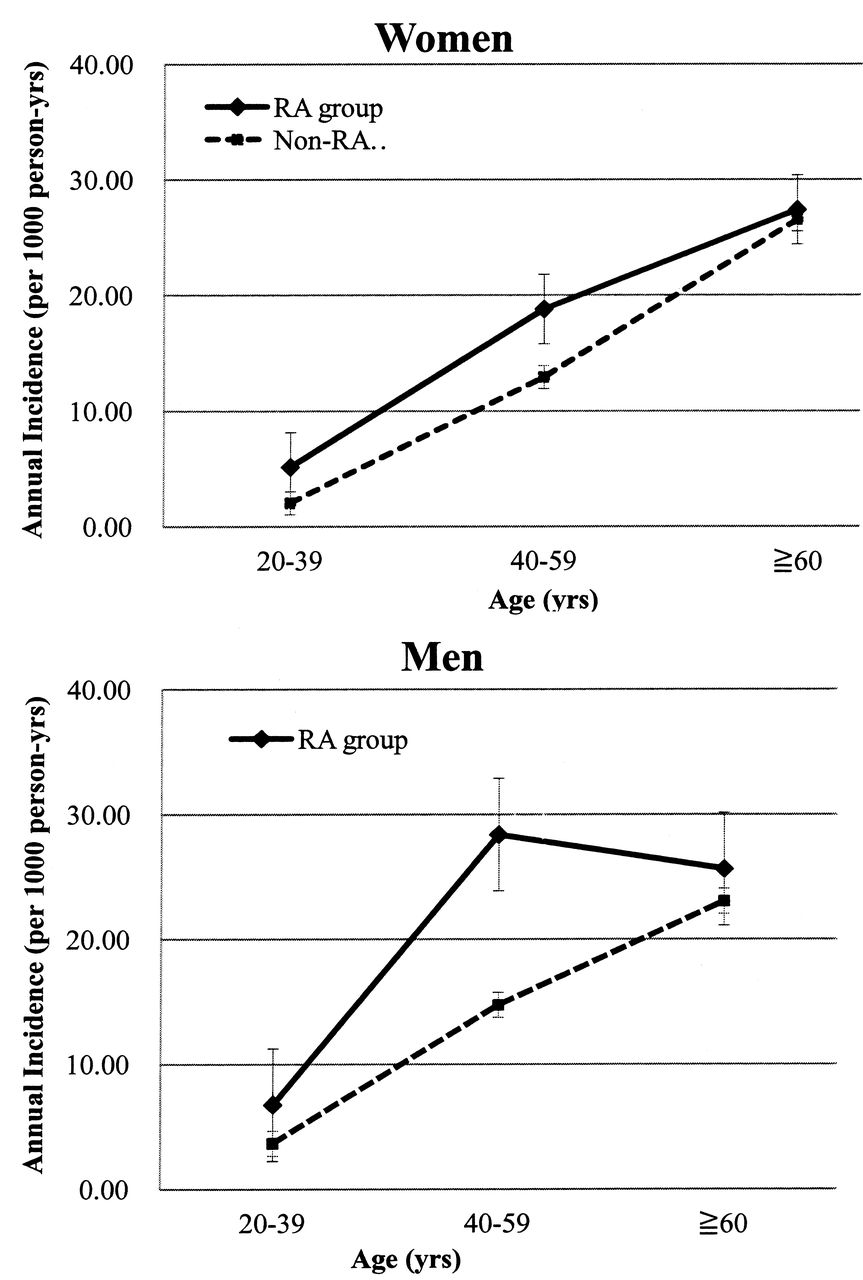
Figure 1 and Table 1 show the incidence of T2D in the RA and non-RA cohorts. Overall, the incidence of T2D increased with age. One exception is that middle-aged men with RA had a higher incidence of T2D than older men with RA. The relative risk of T2D was 1.68 for men with RA and 1.46 for women with RA. The relative risk was higher in the young and middle-aged groups. For older men or women with RA, the effect of RA on the risk for T2D was minimal.

Annual incidence of type 2 diabetes (per 1000 person-yrs) in rheumatoid arthritis (RA) and non-RA groups, in women and men.
Incidence rate of type 2 diabetes (T2D; per 1000 person-yrs) in rheumatoid arthritis (RA) group and non-RA group, by age.
Disease duration and age on the risk of developing T2D
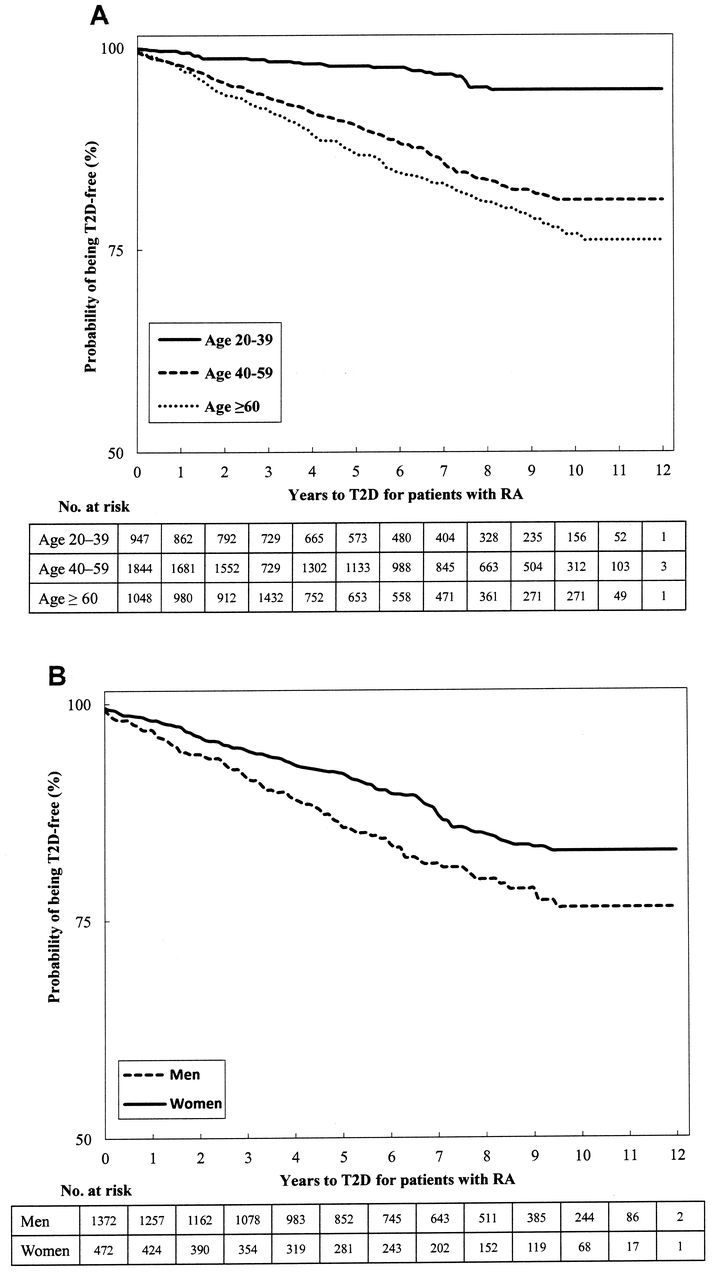
Figure 2A shows the effects of disease duration and age on the risk of developing T2D. As expected, aged people with RA were more likely to develop T2D than younger people with RA. After the RA diagnosis, 2.1% of the young patients, 7.1% of the middle-aged patients, and 10.9% of older patients had developed T2D in 5 years, and 3.7%, 11.4%, and 15.2% of patients from the respective age groups had developed T2D in 10 years.
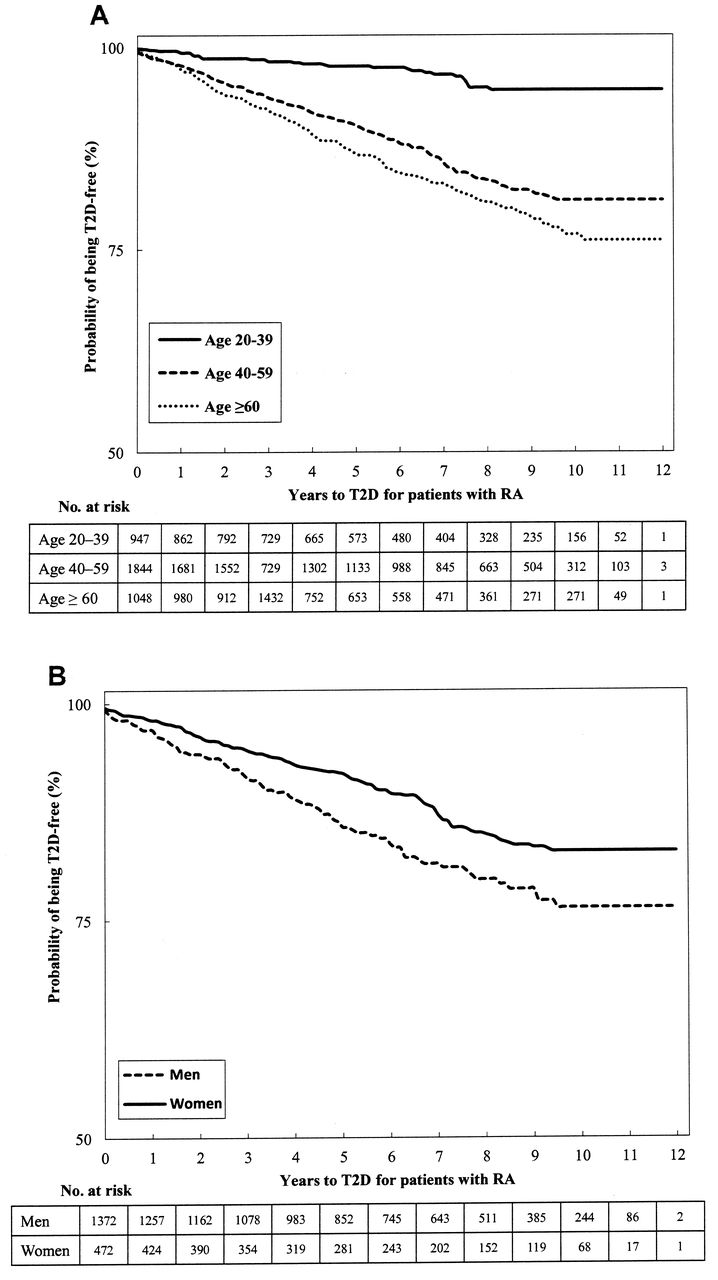
Kaplan-Meier plot of type 2 diabetes (T2D) for patients with rheumatoid arthritis (RA). A. For 3 age groups. B. For men and women age 40–59 years. Log-rank test indicates significant difference for both sexes, with p < 0.0001 and 0.003, respectively.
Sex and the risk of developing T2D
We did not find a significant difference between men and women in the risk of developing T2D for the young adults and older adults. However, there was a significant difference between middle-aged men and women with RA. As shown in Figure 1, middle-aged men with RA are more likely to develop T2D than middle-aged women with RA. Figure 2B shows that for patients with RA, men had a higher T2D hazard than women.
HTN and DLM significantly increase T2D risk
We used Cox regression to study the effects of age, sex, RA, HTN, DLM, and GC use on T2D risk. Table 2 lists the HR obtained from the univariate model and multivariate model with interactions. HTN and DLM are both significantly associated with a higher T2D risk, with HR 2.42 and 4.21, respectively. Comorbidities of both HTN and DLM increased the HR in patients with RA to 22 (95% CI 20–26).
Hazard ratios (HR) for type 2 diabetes from Cox regression, for effects of RA, hypertension (HTN), disorder of lipid metabolism (DLM), and GC usage.
The role of GC use
GC use is a strong risk factor for T2D in patients with RA, based on results from both univariate and multivariate models (Table 2). The multivariate model revealed that GC use has significant interactions with HTN and age. HTN without GC use had a higher HR for T2D than HTN with GC use (HR 2.51 vs 2.03). Nevertheless, HTN, DLM, RA, and GC use are all risk factors for T2D.
We used the Wald chi-square test to verify the proportional hazard assumption for the multivariate Cox model. Because of the large difference in sample sizes between the 2 cohorts, the normal procedure for the Wald test could not apply. To overcome the problem, we used a smaller sample, containing 5000 subjects from the non-RA cohort, to meet the proportional hazard assumption with p value 0.223.
DISCUSSION
Patients with RA are reported to carry a higher cardiovascular risk17, and there is a gap in our understanding of why such a higher risk exists. In addition, RA patients with DM were less likely to be tested for glycosylated hemoglobin18, indicating that rheumatologists need a higher level of awareness of DM and more aggressive intervention. To raise awareness, information is needed on the DM risk for patients with RA and how other clinical factors may modify the risk.
The results of our study, based on a comprehensive national databank, confirm an elevated risk for T2D among patients with RA. T2D incidence increased with age for both sexes. For women with RA, there was an increased risk for T2D and decreased relative risk for T2D with age. But for men with RA, the highest risk for T2D and highest relative risk occurred in middle age (40–60 years). The estimated HR of RA to non-RA in the oldest male group was 1.11; however, this was not statistically significant. Older populations are more likely to have multiple diseases, e.g., coronary heart disease or HTN, and to take multiple medicines, e.g., thiazide or β-blockers, thus diluting the risk of RA for T2D in these populations.
Our study has some limitations. The databank did not include American College of Rheumatology classification criteria. However, our prevalence calculations for RA are consistent with the literature19. We did not address the RA disease severity, disease activity, and patterns of medication use over time, except GC use. In addition, the database did not contain information on body mass index. We also did not obtain actual blood glucose values, especially after glucose challenge. However, the databank allowed us to address the effect of disease duration for risk of developing T2D. As expected, older patients (> 60 years) had the highest risk of developing T2D with the same duration of disease, compared with younger patients with RA. These results can inform rheumatologists of the longterm prognosis of DM risk among their patients with RA. We also studied whether men or women have a higher risk of developing T2D. The only significant difference was between middle-aged men and women with RA. Middle-aged men with RA have a much higher risk of developing T2D than middle-aged women with RA. This result may help physicians to encourage their middle-aged male patients with RA to take more exercise, control body weight, and eat a healthy diet.
The major cause of death for patients with RA is CVD. Besides DM, HTN and hyperlipidemia are well-known risk factors for CVD. To decrease mortality from CVD and improve patient survival, we need to control these risk factors. Our results showed that having HTN or hyperlipidemia increases the risk for DM in patients with RA. If a patient with RA has both conditions, the hazard rate for DM increases 23-fold. These factors are lifestyle-related. A sedentary life, with a diet high in calories and fat, may result in a high body mass index. Metabolic syndrome is the term used to illustrate the concept20. However, it is difficult to change one’s long-accustomed lifestyle, so patients need a strong motivation. An accurate assessment of the risk can certainly promote early and active intervention from doctors and patients, thus lowering the risk for DM and CVD. The information provided here can help physicians assess the DM risk for their patients with RA and alert those with a higher risk to lead a healthy lifestyle, thus taking aggressive preventive measures. At the same time, physicians are also urged to take measures, e.g., to test glycosylated hemoglobin.
Acknowledgment
Our study is based on the National Health Insurance Research Database provided by the Bureau of National Health Insurance of Taiwan.
Footnotes
-
Supported by the National Science Council of Taiwan (NSC99-2314-B018-001-MY3).
- Accepted for publication May 13, 2013.








{kind=link}
{kind=link}